
!
1!
May 2017, Special Issue
Comparing Health-Related Policies and Practices in Sports:
The NFL and Other Professional Leagues
Christopher R. Deubert, I. Glenn Cohen, and Holly Fernandez Lynch
This is a special version of Comparing Health-Related Policies and Practices in Sports: The NFL and
Other Professional Leagues (“the Report”). The Report, part of the Football Players Health Study at
Harvard University, was self-published in May 2017 and can be found on this website:
footballplayershealth.harvard.edu or through Amazon.com. This version is being published through the
Harvard Journal of Sports and Entertainment Law (“JSEL”) to ensure the Report is accessible to
attorneys, law students, the legal community and other academic audiences.
There are ways in which this version is different from the initially published Report and a typical JSEL
article. While several JSEL students were involved in cite checking the majority of the Report, JSEL did
not cite check the entire Report. This possible deficiency was compensated by the Report’s extensive
review and fact checking process, as described in the Introduction. Additionally, the actual Report was
professionally designed, including color graphics and other design elements which could not be included
here. The endnotes were formatted in such a way as to aid the design process and thus do not necessarily
match the style outlined in The Bluebook: A Uniform System of Citation (20th ed. 2015).

!
2!
TABLE CONTENTS
ENSURING INDEPENDENCE AND DISCLOSURE OF CONFLICTS ................................... 11
EXECUTIVE SUMMARY .......................................................................................................... 13
PREFACE: The Football Players Health Study at Harvard University ........................................ 25
INTRODUCTION ........................................................................................................................ 28
A. The Leagues ..................................................................................................................... 28
B. The Unions ....................................................................................................................... 29
C. Collective Bargaining Agreements ................................................................................ 30
D. Audience........................................................................................................................... 31
E. Goals and Process ........................................................................................................... 32
1. Identify ....................................................................................................................... 32
2. Describe ..................................................................................................................... 32
3. Evaluate ..................................................................................................................... 34
4. Recommend ............................................................................................................... 34
F. Scope................................................................................................................................. 35
CHAPTER 1: CLUB MEDICAL PERSONNEL ......................................................................... 36
A. Club Medical Personnel in the NFL .............................................................................. 39
1. Types of Medical Personnel ..................................................................................... 39
2. Medical Personnel’s Obligations ............................................................................. 40
3. Players’ Obligations ................................................................................................. 42
4. Relationship between Medical Personnel and Clubs ............................................ 42
5. Sponsorship Arrangements ..................................................................................... 43
B. Club Medical Personnel in MLB ................................................................................... 46
1. Types of Medical Personnel ..................................................................................... 46
2. Medical Personnel’s Obligations ............................................................................. 48
3. Players’ Obligations ................................................................................................. 49
4. Relationship between Medical Personnel and Clubs ............................................ 50
5. Sponsorship Arrangements ..................................................................................... 51
C. Club Medical Personnel in the NBA ............................................................................. 51
1. Types of Medical Personnel ..................................................................................... 51
2. Medical Personnel’s Obligations ............................................................................. 53
3. Players’ Obligations ................................................................................................. 54
!
3!
4. Relationship between Medical Personnel and Clubs ............................................ 56
5. Sponsorship Arrangements ..................................................................................... 57
D. Club Medical Personnel in the NHL ............................................................................. 57
1. Types of Medical Personnel ..................................................................................... 57
2. Medical Personnel’s Obligations ............................................................................. 59
3. Players’ Obligations ................................................................................................. 60
4. Relationship between Medical Personnel and Clubs ............................................ 61
5. Sponsorship Arrangements ..................................................................................... 61
E. Club Medical Personnel in the CFL .............................................................................. 62
1. Types of Medical Personnel ..................................................................................... 62
2. Medical Personnel’s Obligations ............................................................................. 62
3. Players’ Obligations ................................................................................................. 63
4. Relationship between Medical Personnel and Clubs ............................................ 63
5. Sponsorship Arrangements ..................................................................................... 63
F. Club Medical Personnel in MLS ................................................................................... 64
1. Types of Medical Personnel ..................................................................................... 64
2. Medical Personnel’s Obligations ............................................................................. 65
3. Players’ Obligations ................................................................................................. 66
4. Relationship with Clubs ........................................................................................... 67
5. Sponsorship Arrangements ..................................................................................... 68
G. Analysis ............................................................................................................................ 68
H. Recommendations ........................................................................................................... 71
CHAPTER 2: INJURY RATES AND POLICIES ....................................................................... 72
A. Injuries in the NFL ......................................................................................................... 75
1. Injury Tracking System ........................................................................................... 75
2. Injury Statistics ......................................................................................................... 76
3. Injury-Related Lists ................................................................................................. 79
4. Injury Reporting Policies ......................................................................................... 80
B. Injuries in MLB .............................................................................................................. 81
1. Injury Tracking System ........................................................................................... 81
2. Injury Statistics ......................................................................................................... 81
3. Injury-Related Lists ................................................................................................. 83
4. Injury Reporting Policies ......................................................................................... 83
C. Injuries in the NBA ......................................................................................................... 84
!
4!
1. Injury Tracking System ........................................................................................... 84
2. Injury Statistics ......................................................................................................... 84
3. Injury-Related Lists ................................................................................................. 86
4. Injury Reporting Policies ......................................................................................... 86
D. Injuries in the NHL ......................................................................................................... 86
1. Injury Tracking System ........................................................................................... 86
2. Injury Statistics ......................................................................................................... 86
3. Injury-Related Lists ................................................................................................. 88
4. Injury Reporting Policies ......................................................................................... 89
E. Injuries in the CFL ......................................................................................................... 89
1. Injury Tracking System ........................................................................................... 89
2. Injury Statistics ......................................................................................................... 89
3. Injury-Related Lists ................................................................................................. 90
4. Injury Reporting Policies ......................................................................................... 90
F. Injuries in MLS ............................................................................................................... 90
1. Injury Tracking System ........................................................................................... 90
2. Injury Statistics ......................................................................................................... 90
3. Injury-Related Lists ................................................................................................. 92
4. Injury Reporting Policies ......................................................................................... 92
G. Analysis ............................................................................................................................ 92
H. Recommendations ........................................................................................................... 97
CHAPTER 3: HEALTH-RELATED BENEFITS ...................................................................... 100
A. NFL Health-Related Benefits ....................................................................................... 103
1. Retirement Benefits ................................................................................................ 104
2. Insurance Benefits .................................................................................................. 107
3. Disability Benefits ................................................................................................... 108
4. Workers’ Compensation Benefits ......................................................................... 110
5. Education-Related Benefits ................................................................................... 110
6. Joint Health-Specific Committees ......................................................................... 110
B. MLB Health-Related Benefits ...................................................................................... 111
1. Retirement Benefits ................................................................................................ 111
2. Insurance Benefits .................................................................................................. 113
3. Disability Benefits ................................................................................................... 113
4. Workers’ Compensation Benefits ......................................................................... 114
!
5!
5. Education-Related Benefits ................................................................................... 114
6. Joint Health-Specific Committees ......................................................................... 114
C. NBA Health-Related Benefits ...................................................................................... 114
1. Retirement Benefits ................................................................................................ 114
2. Insurance Benefits .................................................................................................. 115
3. Disability Benefits ................................................................................................... 116
4. Workers’ Compensation Benefits ......................................................................... 116
5. Education-Related Benefits ................................................................................... 117
6. Joint Health-Specific Committees ......................................................................... 117
D. NHL Health-Related Benefits ...................................................................................... 118
1. Retirement Benefits ................................................................................................ 118
2. Insurance Benefits .................................................................................................. 119
3. Disability Benefits ................................................................................................... 119
4. Workers’ Compensation Benefits ......................................................................... 120
5. Education-Related Benefits ................................................................................... 120
6. Joint Health-Specific Committees ......................................................................... 120
E. CFL Health-Related Benefits ........................................................................................... 120
1. Retirement Benefits ................................................................................................ 120
2. Insurance Benefits .................................................................................................. 120
3. Disability Benefits ................................................................................................... 121
4. Workers’ Compensation Benefits ......................................................................... 121
5. Education-Related Benefits ................................................................................... 121
6. Joint Health-Specific Committees ......................................................................... 121
F. MLS Health-Related Benefits ...................................................................................... 121
1. Retirement Benefits ................................................................................................ 121
2. Insurance Benefits .................................................................................................. 121
3. Disability Benefits ................................................................................................... 122
4. Workers’ Compensation Benefits ......................................................................... 122
5. Education-Related Benefits ................................................................................... 122
6. Joint Health-Specific Committees ......................................................................... 122
G. Analysis .......................................................................................................................... 122
H. Recommendation ........................................................................................................... 126
CHAPTER 4: DRUG AND PERFORMANCE-ENHANCING SUBSTANCE POLICIES ...... 127
A. The NFL’s Drug Policies .............................................................................................. 129
!
6!
1. Substances Prohibited ............................................................................................ 130
2. Types of Tests and Prohibited Conduct ............................................................... 130
3. Number of Tests ...................................................................................................... 131
4. Administration ........................................................................................................ 132
5. Therapeutic Use ...................................................................................................... 132
6. Treatment ................................................................................................................ 133
7. Discipline ................................................................................................................. 134
8. Confidentiality ........................................................................................................ 135
B. MLB’s Drug Policies ..................................................................................................... 136
1. Substances Prohibited ............................................................................................ 136
2. Types of Tests and Prohibited Conduct ............................................................... 136
3. Number of Tests ...................................................................................................... 136
4. Administration ........................................................................................................ 137
5. Therapeutic Use ...................................................................................................... 137
6. Treatment ................................................................................................................ 137
7. Discipline ................................................................................................................. 138
8. Confidentiality ........................................................................................................ 139
C. The NBA’s Drug Policies .............................................................................................. 139
1. Substances Prohibited ............................................................................................ 139
2. Types of Tests and Prohibited Conduct ............................................................... 139
3. Number of Tests ...................................................................................................... 140
4. Administration ........................................................................................................ 140
5. Therapeutic Use ...................................................................................................... 140
6. Treatment ................................................................................................................ 140
7. Discipline ................................................................................................................. 141
8. Confidentiality ........................................................................................................ 142
D. The NHL’s Drug Policies .............................................................................................. 143
1. Substances Prohibited ............................................................................................ 143
2. Types of Tests and Prohibited Conduct ............................................................... 143
3. Number of Tests ...................................................................................................... 144
4. Administration ........................................................................................................ 144
5. Therapeutic Use ...................................................................................................... 145
6. Treatment ................................................................................................................ 145
7. Discipline ................................................................................................................. 145
!
7!
8. Confidentiality ........................................................................................................ 146
E. The CFL’s Drug Policies .............................................................................................. 147
1. Substances Prohibited ............................................................................................ 147
2. Types of Tests and Prohibited Conduct ............................................................... 147
3. Number of Tests ...................................................................................................... 147
4. Administration ........................................................................................................ 148
5. Therapeutic Use ...................................................................................................... 148
6. Treatment ................................................................................................................ 148
7. Discipline ................................................................................................................. 148
8. Confidentiality ........................................................................................................ 149
F. MLS’ Drug Policies ....................................................................................................... 149
1. Substances Prohibited ............................................................................................ 149
2. Types of Tests and Prohibited Conduct ............................................................... 149
3. Number of Tests ...................................................................................................... 150
4. Administration ........................................................................................................ 150
5. Therapeutic Use ...................................................................................................... 150
6. Treatment ................................................................................................................ 150
7. Discipline ................................................................................................................. 151
8. Confidentiality ........................................................................................................ 151
G. Analysis .......................................................................................................................... 151
H. Recommendation ........................................................................................................... 154
CHAPTER 5: COMPENSATION .............................................................................................. 155
A. Compensation in the NFL ............................................................................................ 157
1. The NFL’s Salary Cap ........................................................................................... 157
2. Rookie Compensation ............................................................................................ 158
3. Veteran Compensation ........................................................................................... 159
4. Minimum, Maximum, and Average (Mean) Salaries .......................................... 160
5. Guaranteed Compensation .................................................................................... 161
B. Compensation in MLB ................................................................................................. 163
1. MLB’s Tax Threshold ............................................................................................ 163
2. Rookie Compensation ............................................................................................ 164
3. Veteran Compensation ........................................................................................... 164
4. Minimum, Maximum, and Average (Mean) Salaries .......................................... 165
5. Guaranteed Compensation .................................................................................... 166
!
8!
C. Compensation in the NBA ............................................................................................ 166
1. The NBA’s Salary Cap ........................................................................................... 166
2. Rookie Compensation ............................................................................................ 167
3. Veteran Compensation ........................................................................................... 168
4. Minimum, Maximum, and Average (Mean) Salaries .......................................... 169
5. Guaranteed Compensation .................................................................................... 171
D. Compensation in the NHL ........................................................................................... 172
1. The NHL’s Salary Cap ........................................................................................... 172
2. Rookie Compensation ............................................................................................ 173
3. Veteran Compensation ........................................................................................... 173
4. Minimum, Maximum, and Average (Mean) Salaries .......................................... 174
5. Guaranteed Compensation .................................................................................... 175
E. Compensation in the CFL ............................................................................................ 175
1. The CFL’s Salary Cap ........................................................................................... 175
2. Rookie Compensation ............................................................................................ 176
3. Veteran Compensation ........................................................................................... 176
4. Minimum, Maximum, and Average (Mean) Salaries .......................................... 176
5. Guaranteed Compensation .................................................................................... 177
F. Compensation in MLS .................................................................................................. 178
1. MLS’ Salary Cap .................................................................................................... 179
2. Rookie Compensation ............................................................................................ 179
3. Veteran Compensation ........................................................................................... 179
4. Minimum, Maximum, and Average (Mean) Salaries .......................................... 179
5. Guaranteed Compensation .................................................................................... 179
G. Analysis .......................................................................................................................... 180
H. Recommendation ........................................................................................................... 181
CHAPTER 6: ELIGIBILITY RULES ........................................................................................ 182
A. Player Eligibility Rules in the NFL ............................................................................. 186
B. Player Eligibility Rules in MLB .................................................................................. 189
C. Player Eligibility Rules in the NBA ............................................................................. 192
D. Player Eligibility Rules in the NHL ............................................................................. 194
E. Player Eligibility Rules in the CFL ............................................................................. 196
F. Player Eligibility Rules in MLS ................................................................................... 197
G. Analysis .......................................................................................................................... 198

!
9!
H. Recommendations ......................................................................................................... 199
CONCLUSION ........................................................................................................................... 200
APPENDIX A – COMPILATION OF RECOMMENDATIONS ............................................. 202
I. Club Medical Personnel ............................................................................................... 202
II. Injury Rates and Policies.............................................................................................. 203
III. Health-Related Benefits ............................................................................................. 205
IV. Drug and Performance-Enhancing Drug Policies ................................................... 206
V. Compensation ................................................................................................................ 207
VI. Eligibility Rules .......................................................................................................... 209
APPENDIX B – COMPILATION OF SUMMARY TABLES .................................................. 210
APPENDIX C – GLOSSARY OF TERMS AND RELEVANT PERSONS AND
INSTITUTIONS ......................................................................................................................... 214
About the Authors
Christopher R. Deubert is the Senior Law and Ethics Associate for the Law and Ethics Initiative of the
Football Players Health Study at Harvard University. Previously, Deubert practiced commercial litigation,
sports law, securities litigation, and labor/employment litigation at Peter R. Ginsberg Law, LLC f/k/a
Ginsberg & Burgos, PLLC in New York City. His sports practice focused primarily on representing
National Football League (NFL) players in League matters, including appeals for Commissioner
Discipline, under the NFL’s Policy and Program on Substances of Abuse and under the NFL’s Policy on
Anabolic Steroids and Related Substances (now known as the Policy on Performance-Enhancing
Substances), and related litigation. Deubert also previously worked for Sportstars, Inc., one of the largest
NFL-player representation firms, performing contract, statistical, and legal analysis, and he performed
similar work during an internship with the New York Jets. Deubert graduated with a joint
JD/MBA degree from Fordham University School of Law and Graduate School of Business in 2010, and
a BS in Sport Management from the University of Massachusetts in 2006.
I. Glenn Cohen is a professor at Harvard Law School; Faculty Director of the Petrie-Flom Center for
Health Law Policy, Biotechnology, and Bioethics; and, Co-Lead of the Law and Ethics Initiative of the
Football Players Health Study. His award-winning work at the intersection of law, medicine, and ethics—
in particular, medical tourism and assisted reproduction—has been published in leading journals, such as
the Harvard Law Review, Stanford Law Review, New England Journal of Medicine, Journal of the
American Medical Association, American Journal of Bioethics, and American Journal of Public Health.
He was previously a fellow at the Radcliffe Institute for Advanced Study and a faculty scholar in
bioethics with the Greenwall Foundation. He is the author, editor, and/or co-editor of several books from
Oxford, Columbia, John Hopkins, and MIT University Presses. Prior to joining the Harvard faculty,
Cohen served as a clerk to Chief Judge Michael Boudin, United States Court of Appeals for the First
Circuit, and as an appellate lawyer in the Civil Division of the Department of Justice. He graduated from
the University of Toronto with a BA (with distinction) in Bioethics (Philosophy) and Psychology and
earned his JD from Harvard Law School.
Holly Fernandez Lynch is Executive Director of the Petrie-Flom Center for Health Law Policy,
Biotechnology, and Bioethics; Faculty at the Harvard Medical School Center for Bioethics; and, Co-Lead
!
10!
of the Law and Ethics Initiative of the Football Players Health Study. Her scholarly work focuses on the
regulation and ethics of human subjects research and issues at the heart of the doctor-patient relationship.
Her book, Conflicts of Conscience in Health Care: An Institutional Compromise, was published by MIT
Press in 2008; she is also co-editor with I. Glenn Cohen of Human Subjects Research Regulation:
Perspectives on the Future (MIT Press 2014), FDA in the 21st Century: The Challenges of Regulating
Drugs and New Technologies (Columbia University Press 2015), and Nudging Health: Health Law and
Behavioral Economics (Johns Hopkins University Press 2016). Lynch practiced pharmaceuticals law at
Hogan & Hartson, LLP (now Hogan Lovells), in Washington, DC, and worked as a bioethicist in the
Human Subjects Protection Branch at the National Institutes of Health’s Division of AIDS. She also
served as senior policy and research analyst for President Obama’s Commission for the Study of
Bioethical Issues. Lynch is currently a member of the Secretary’s Advisory Committee on Human
Research Protections at the US Department of Health and Human Services. She graduated Order of the
Coif from the University of Pennsylvania Law School, where she was a Levy Scholar in Law and
Bioethics. She earned her master’s degree in bioethics from the University of Pennsylvania’s School of
Medicine, and her BA with a concentration in bioethics, also from the University of Pennsylvania.

!
11!
Acknowledgements
First, the authors would like to thank the staff and research assistants who assisted in the creation of this
Report: Daniel Ain; Tom Blackmon; Jay Cohen; Louis Fisher; Nicholas Hidalgo; Scott Sherman; Jamie
Smith-George; and, Samuel Stuckey. These individuals assisted with a variety of administrative and
research tasks. Relatedly, the authors would like to thank Professor Peter Carfagna for helping to
coordinate research assistance by his students. Particular thanks are due to Justin Leahey, Project
Coordinator for the Law & Ethics Initiative of the Football Players Health Study, who provided important
administrative and research assistance throughout the creation of the Report.
Second, the authors would like to thank the members of the Law & Ethics Advisory Panel for their
comments and guidance during the creation of this Report: Nita Farahany; Joseph Fins; Ashley Foxworth;
Walter Jones; Isaiah Kacyvenski; Bernard Lo; Chris Ogbonnaya; and, Dick Vermeil.
Third, the authors would like to thank the expert reviewers of this Report who provided valuable
comments during the editing process: Marc Edelman, Zicklin School of Business, Baruch College, City
University of New York; and, Michael McCann, University of New Hampshire School of Law.
Fourth, the authors would like to thank the professors and academic professionals who reviewed and
provided comments for parts of this Report: Neil Longley; Stephanie Morain; and, Karen Roos.
Relatedly, the authors would like to thank The Hastings Center, who initially proposed the idea of this
Report.
Fifth, the authors would like to thank the professionals who helped finalize this Report: Lori Shridhare
from the Football Players Health Study at Harvard University; Cristine Hutchison-Jones, who provided
proofreading and editing services; and, Fassino/Design, Inc., which designed and formatted the Report.
Finally, the authors would like to thank the leagues and players unions that agreed to provide relevant
information and/or review this Report prior to its publication. In the Introduction, we provide more detail
as to those leagues and unions that provided relevant information and/or reviewed this Report prior to its
publication. The cooperation of the leagues and players unions was essential to the accuracy, fairness, and
comprehensiveness of this Report.
ENSURING INDEPENDENCE AND DISCLOSURE OF CONFLICTS
The 2011 Collective Bargaining Agreement between the National Football League Players Association
(“NFLPA”) and the National Football League (“NFL”) set aside funds for medical research. The NFLPA
directed a portion of those funds to create the Football Players Health Study at Harvard University, of
which this Report is a part. Our analysis has been independent of any controlling interest by the NFLPA,
the NFL, or any other party; this independence was contractually protected in Harvard’s funding
agreement with the NFLPA. Per that contract, the NFLPA was only entitled to prior review of this Report
to ensure that no confidential information was disclosed.
1
Additional information about how this Report
came to be is provided in the Preface.
The present Report is part of the Law and Ethics Initiative of the Football Players Health Study at
Harvard University. Additional background information about the Football Players Health Study is
provided in the Preface. We provide more specific information about the Law and Ethics Initiative here.
!
12!
The Statement of Work agreed to between the NFLPA and Harvard included as one of the Law and Ethics
Initiative’s projects to “Conduct Comparative Sports League Analysis.” More specifically, Harvard
described the work to be done as follows:
We will analyze governance and stakeholder obligations in other
professional sports leagues in order to identify best practices and situate
the ethics framework developed for professional football. This project
will examine, for example, how medical practices in other leagues may
result in the encouragement and tolerance of behavior that is risky to
health. The project will examine influences among health behaviors of
players and team policies regarding player health.
This project description was intended to be preliminary. The actual scope of this Report developed over
time, as expected, as the result of considerable research, internal discussion, and conversations with
experts. Beyond agreeing to the Statement of Work, the NFLPA did not direct the scope or content of this
Report.
As is typical with sponsored research, we provided periodic updates to the sponsor in several formats:
Pursuant to the terms of Harvard-NFLPA agreement, the NFLPA does receive an annual report on the
progress of the Football Players Health Study as well as one Quad Chart progress report each year.
Additionally, on two occasions (August 22, 2014, and January 23, 2015), we presented a summary of the
expected scope and content of the Report to the Football Players Health Study Executive Committee,
comprised of both Harvard and NFLPA personnel. Those meetings did not alter our approach in
constructing this Report, the conclusions reached, or the recommendations made. Moreover, none of the
comments made during those meetings altered the content of the Report.
In the Introduction, Section E(2): Describe, we discuss our research process for this Report. Additional
information about our communications with the NFLPA and NFL is also relevant here. During the course
of our research, we had multiple telephone and email communications with both NFLPA and NFL
representatives to gain factual information. These communications were not about the progress, scope, or
structure of our Report.
We also concluded that it was essential to provide the applicable stakeholders the opportunity to
substantively review the Report. These stakeholders are the leagues discussed in this Report: the National
Football League (“NFL”); Major League Baseball (“MLB”); the National Basketball Association
(“NBA”); the National Hockey League (“NHL”); the Canadian Football League (“CFL”); and, Major
League Soccer (“MLS”). This was necessary to try to fully account for the realities at hand, avoid factual
errors, and fairly consider all sides. Accordingly, we provided each league the opportunity to review the
Report before publication. Additional information about the leagues’ and their corresponding labor
unions’ cooperation with and review of this Report or failure to do so is included in the Introduction,
Section 6(C): Limitations.
The leagues had the opportunity to identify any errors, provide additional information, comment on what
action we expected from them going forward, and raise further suggestions or objections. Sometimes
these comments led to valuable changes in the Report. We found other comments unpersuasive and they
did not result in any changes. It is critical to recognize that no external party, including the NFLPA and
NFL, had the ability to direct or alter our analysis or conclusions.
In addition, we subjected the draft Report to peer review by outside experts. We engaged two independent
experts in sports law to review the Report for accuracy, fairness, comprehensibility, and its ability to
positively impact the health of NFL players. These experts were Marc Edelman, Zicklin School of

!
13!
Business, Baruch College, City University of New York, and, Michael McCann, University of New
Hampshire School of Law.
Finally, the content of this Report is solely the responsibility of the authors and does not represent the
official views of the NFLPA or Harvard University.
Disclosures:
• The Law and Ethics Initiative’s allocated budget is a total of $1,257,045 over three years, which
funds not only the present Report, but also several other projects.
2
• Deubert’s salary is fully supported by the Football Players Health Study at Harvard University.
From August 2010 to May 2014, Deubert was an associate at the law firm of Peter R. Ginsberg
Law, LLC f/k/a Ginsberg & Burgos, PLLC. During the course of his practice at that firm, Deubert
was involved in several legal matters in which the NFL was an opposing party. Of relevance to
this Report, Deubert represented players disciplined pursuant to the NFL’s Policy and Program on
Substances of Abuse and the Policy on Anabolic Steroids and Related Substances (now known as
the Policy on Performance-Enhancing Substances). Also, since 2007, Deubert has provided
research assistance to the Sports Lawyers Association, whose Board of Directors includes many
individuals with interests related to this work.
Lastly, in March 2017, as this Report’s content was finalized except for incorporating some
changes related to new collective bargaining agreements in MLB and the NBA, and with the Law
& Ethics Initiative of the Football Players Health Study ending in May 2017 as the funding period
came to a close, Deubert communicated with organizations with interests relevant to this work
about potential job opportunities, including law firms that represent sports leagues, unions, and
players. Following finalization of the Report, Deubert also communicated with some of the
sports unions themselves about potential job opportunities. All changes to the Report, including
those that occurred during or after March 2017, were reviewed and approved by Cohen and
Lynch.
• 20% of Cohen’s salary is supported by the Football Players Health Study at Harvard University.
Cohen has no other conflicting interests to report.
• 30% of Lynch’s salary is supported by the Football Players Health Study at Harvard University.
Lynch has no other conflicting interests to report.
EXECUTIVE SUMMARY
INTRODUCTION
What can the NFL and NFLPA learn from the policies and practices of other elite professional sports
leagues about protecting and promoting player health? This is the fundamental question motivating this
Report, authored by members of the Law & Ethics Initiative of the Football Players Health Study at
Harvard University.
3
This Report, Comparing Health-Related Policies and Practices in Sports: The NFL and Other
Professional Leagues, seeks to answer that question. The leagues share considerable similarities—at their
core, they are organizations that coordinate elite-level athletic competitions for mass audiences. In this
respect, the leagues are competitors within the professional sports industry, with each of them competing
!
14!
for fans’ dollars and attention. The policies by which the leagues operate, and their practices, are thus
often very similar. However, as in any industry, there are also differences between the leagues. This
Report seeks to identify and understand those different policies and practices that have the possibility to
affect player health such that the leagues may be able to learn from one another.
While leagues and their games are different in many important respects, making it impractical and unfair
to opine as a definitive matter on which of the leagues’ policies and practices in their totality best protect
player health, the Report generally concludes that the NFL’s policies concerning player health appear
superior to the other leagues. Nevertheless, through the nine recommendations contained in this Report,
we hope to elucidate several ways in which the NFL can learn from other leagues and further improve
player health.
This Report has four functions. First, to identify the various policies that do or could influence the health
of players in the various leagues. Second, to describe the policies and their relation to protecting and
promoting player health. Third, to evaluate the capacity of these policies to protect and promote player
health, in particular, by comparing policies on similar issues. And fourth, to recommend changes to
policies that affect NFL players grounded in our evaluation of certain approaches taken by other leagues
that appear to be more favorable. Where possible, we perform the same analysis concerning the leagues’
practices related to player health.
In this Executive Summary, we provide only summaries of the key issues discussed in the Report, while
the Report covers more issues and provides more complexity, nuance, and all relevant citations. Appendix
A of the Report is a compilation of the Report’s recommendations with explanatory text and Appendix B
is a compilation of tables summarizing and comparing the leagues’ policies and practices.
In the remainder of this summary Introduction, we identify the leagues and player unions relevant to our
analysis and summarize the areas of potential improvement we found when comparing the policies and
practices of the NFL to the other leagues. Then, we provide a summary of each of the issues analyzed in
the Report: (1) Club Medical Personnel; (2) Injury Rates and Policies; (3) Health-Related Benefits; (4)
Drug and Performance-Enhancing Substance Policies; (5) Compensation; and, (6) Eligibility Rules.
A. The Leagues
This Report analyzes the policies and practices of the following professional sports leagues:
• The National Football League (“NFL”): The world’s premier professional football league,
consisting of 32 member clubs. The NFL’s 2017 revenues are expected to reach $14 billion.
• Major League Baseball (“MLB”): The world’s premier professional baseball organization,
consisting of 30 member clubs. MLB’s 2016 revenues were an estimated $10 billion.
• National Basketball Association (“NBA”): The world’s premier professional basketball league,
consisting of 30 member clubs. The NBA’s 2016–17 revenues are projected to be approximately
$8 billion.
• National Hockey League (“NHL”): The world’s premier professional hockey league, consisting
of 30 member clubs. The NHL’s 2015–16 revenues were an estimated $4.1 billion.

!
15!
• Canadian Football League (“CFL”): A professional football league consisting of 9 member
clubs, all of which are located in Canada. The CFL’s revenues are an estimated $200 million
annually.
• Major League Soccer (“MLS”): A professional soccer league consisting of 20 clubs. As is
explained in further detail in the Report, MLS is uniquely organized—rather than having each
club owned and controlled by a different person or entity (like in the other sports leagues), all of
the clubs in the MLS are owned and controlled by Major League Soccer, LLC. MLS’ 2016
revenues were an estimated $600 million.
We chose these leagues because of their similarity to the NFL, both structurally and legally. The NFL,
MLB, NBA, and NHL are particularly similar. Each of these leagues has been operating for nearly a
century (or more in the case of MLB) and is an entrenched part of the American sports and cultural
landscape. Their revenue streams also dwarf those of any other professional sports leagues, including the
CFL and MLS. For these reasons, the NFL, MLB, NBA, and NHL are commonly referred to collectively
as the “Big Four” sports leagues. We nevertheless acknowledge that other sports and sports leagues can
provide lessons for the NFL and the other sports leagues concerning player health. The CFL was
included in our analysis because it is the only other long-standing and continuous professional football
league. Finally, the MLS was included because it is a major North American professional sports league.
B. The Unions
Each of the leagues discussed in this Report has an important counterpart. The leagues are the constructs
of the individual clubs (or operator-investors in MLS) and thus are principally interested in protecting and
advancing the rights of the clubs. To protect and advance their rights and interests, the players in each of
the leagues have formed a players association, a labor union empowered with certain rights and
responsibilities under federal labor laws. The players associations are:
• National Football League Players Association (“NFLPA”)
• Major League Baseball Players Association (“MLBPA”)
• National Basketball Players Association (“NBPA”)
• National Hockey League Players Association (“NHLPA”)
• Canadian Football League Players Association (“CFLPA”)
• Major League Soccer Players Union (“MLSPU”)
C. Areas for Improvement
As stated earlier, the NFL’s player health provisions are generally the most protective of player health
among the relevant comparators. Nevertheless, we also identified many areas in which the policies and
practices of the NFL concerning player health could potentially be improved by comparison to the other
leagues:
1. The CFL CBA, unlike the NFL CBA, requires that pre-season physicals “to determine the status
of any pre-existing condition” be performed by a neutral physician.
2. The standard of care articulated in the NHL and MLS CBAs, unlike the NFL CBA, seemingly
!
16!
requires club doctors to subjugate their duties to the club to their duties to the player at all times.
3. MLB, unlike the NFL, has a concussion-specific short-term injury list.
4. The MLB, NHL, and CFL injury reporting policies, unlike the NFL, do not require the disclosure
of the location on the body of a player’s injury.
5. MLB, the NBA, and the NHL, unlike the NFL, generally offer health insurance to players for life.
6. Among the Big Four leagues, the retirement plan payments offered by the NFL are the lowest.
7. MLB and NHL players, unlike in those in the NFL, are vested in their pension plans on the first
day they play in the league.
8. The NBA and CFL, unlike the NFL, offer treatment to players who have violated their
performance-enhancing substance policies.
9. The amount of player compensation that is guaranteed in the NFL is substantially lower than in
the other Big Four leagues.
10. The NFL has the most prohibitive eligibility rule of the leagues (except the CFL).
In the full Report, for each of these possible improvements we discuss whether the NFL’s policies might
be justifiably different than the other leagues’.
Chapter 1: Club Medical Personnel
This Chapter discusses the role of club medical staff, including both doctors and athletic trainers, in each
of the sports leagues as set forth in the leagues’ various controlling policies, most principally, their CBAs.
In particular, we focus on: (1) the types of medical personnel required, if any; (2) the medical personnel’s
obligations; (3) the obligations of the players concerning club medical personnel; (4) the relationship
between the medical personnel and the clubs; and, (5) the existence of sponsorship arrangements between
medical personnel and the clubs, if any.
Our focus here is on the structural issues that are generally governed by the CBA or other policies rather
than how each individual club hires and supervises its medical personnel and how individual medical
personnel interact with individual players, matters that are not the subject of extensive reporting or
publicly available research. By understanding what is required or permitted pursuant to the CBA or other
policies we can understand the scope of possible practices, including those that might be concerning as
they relate to player health.
Our analysis suggests that the NFL’s policies concerning club medical personnel are overall, by
comparison to the other leagues, the most protective of player health in almost all cases by providing
players with superior control and information about their healthcare. Nevertheless, there are four areas in
which the NFL might appear deficient as compared to one or more of the other leagues. Two of these
apparent deficiencies (access to medical records and prescription medication monitoring) are not a
problem in practice. We believe that a third deficiency – the inherent conflict of interest in the structure
of club medical staffs and related standard of care provisions – are not adequately addressed by any of the
leagues. This issue and our proposed recommendation is discussed at length in our report Protecting and
Promoting the Health of NFL Players: Legal and Ethical Analysis and Recommendations. Thus, here, we
focus on the lone issue resulting in a recommendation for the NFL.
While the CFL Standard Player Contract requires players to submit to a pre-season physical by the club’s
doctors, the CFL CBA also requires that pre-season physicals “to determine the status of any pre-existing
condition” be performed by a neutral physician. The stated purpose of this requirement is to help
determine “in the future” whether there was “an aggravation of… [a] pre-existing condition.” In contrast,
NFL club doctors perform all pre-season physicals and would be the ones to opine about a player’s prior
!
17!
injury history. We believe the CFL’s approach is preferred, and thus recommend that the NFL consider
adopting such an approach:
• Recommendation 1-A: Pre-season physicals for the purpose of evaluating a player’s prior
injuries should be performed by neutral doctors.
Chapter 2: Injury Rates and Policies
An important measurement of player health is the incidence and type of injuries players may sustain in
the course of their work. Additionally, given the importance of player injuries, the manner in which
player injuries are handled administratively and reported can indicate a league’s approach to player health
issues more generally. In this Chapter, we examine the leagues’: (1) injury tracking systems; (2) injury
rates; (3) injury-related lists; and, (4) policies concerning public reporting of injuries. In summarizing our
analysis, it is important to note that there are important limitations in analyzing and comparing the
leagues’ injury data, described at length in the full Report, including but not limited to the underreporting
of injuries (concussions in particular), and differences between the leagues, including scheduling,
electronic medical record systems, and injury definitions.
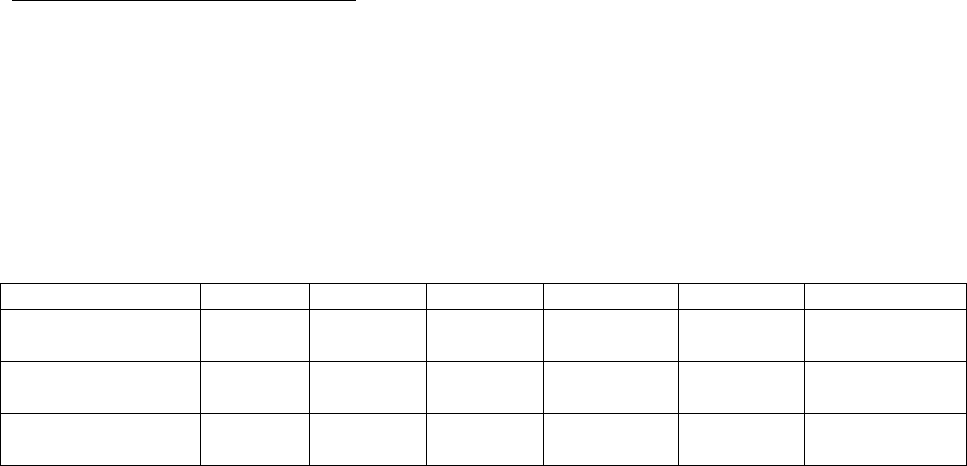
Statistic
NFL
MLB
NBA
NHL
CFL
4
UEFA
5
Mean Injuries Per
Game
5.90
0.45
0.16
0.59
N/A
0.53
Concussions Per
Game
0.625
0.007
0.007
0.067
0.704
0.010
Rate of Concussion
Per Player-Game
6
0.00679
0.00026
0.00035
0.00180
0.00800
0.00072
This Table provides some of the key injury statistics in comparing the leagues, though we provide many
more statistics and caveats in the Report itself. The NFL’s injury rates are much higher than those of the
other leagues. The mean number of injuries suffered per game in the NFL is approximately 3.4 times
higher than the combined rates of MLB, the NBA, NHL, and UEFA combined. Similarly, the NFL’s
concussion per game rate is approximately 6.9 times higher than the combined rates of those same
leagues. We excluded the CFL from this comparison because it is also a football league, but we note that
the CFL’s concussion per game rate is actually higher than the NFL’s.
At the same time, the NFL’s rate of concussions per player-season is 0.073, lower than the NHL’s of
0.108. Thus, if one compared one NFL player and one NHL player, the NHL player would be more likely
to suffer a concussion in his next regular season than the NFL player during his next season. However,
this difference is due to the fact that the NHL plays substantially more regular season games than the NFL
(82 versus 16). When comparing concussion statistics on a per game basis, an NFL player is
approximately 3.8 times more likely to suffer a concussion in a regular season game as compared to an
NHL player (0.00679/0.00180).
One other caveat is worth emphasizing. Due to data availability these statistics and those in the Report are
limited to the leagues’ regular season games, which underestimates injury rates. As we emphasize in the
full Report, there are a significant number of injuries and concussions sustained during NFL practices and
during the pre-season (90 concussions in 2015 practices and pre-season games).
Injury Tracking Systems
!
18!
Each of the Big Four leagues and the MLS has an injury tracking system of some kind. Discussions with
experts on this issue indicated that the injury tracking systems are generally comparable; each of them is a
sophisticated and modern system that should enable accurate reporting and provide interesting and useful
data. The differences may come in how the leagues use the data that is available to them.
The NFL and NBA employ Quintiles, a health information technology firm, to perform sophisticated data
analysis concerning player injuries. While other leagues have occasionally made injury data available for
analysis, our research has not revealed whether the other leagues perform an ongoing annual analysis like
Quintiles does for the NFL and NBA.
Injury-Related Lists
The NFL, NBA, and NHL all permit their clubs to declare players inactive one game at a time, which is
generally advantageous to players. We use the NFL as an example. In the NFL, clubs have a 53-man
Active/Inactive List, only 46 of whom can be active for the game each week. The remaining seven
players are placed on the Inactive List for the game, i.e., benched, either for injury or skill purposes, but
are available to play in the next week’s game. This arrangement permits players the opportunity to remain
on the roster but to rest and treat an injury without immediately rushing back to play. At the same time,
because clubs are constantly struggling with having the best players available as well as likely having
multiple injured players, players will still likely feel pressure to return as soon as possible so that the club
can deactivate other injured players and avoid seeking a replacement.
The Active/Inactive List is also interrelated with the Injured Reserve list, designated for players with
longer-term injuries. Generally, once a player is on Injured Reserve, he is no longer eligible to play that
season. However, by placing the player on Injured Reserve, the club can replace the player on the 53-man
Active/Inactive List. Thus, there are important implications in determining whether the player’s injury is
short-term and the club only has to declare him inactive for a game or two, or whether the player’s injury
is more severe and requires the player to be placed on Injured Reserve (which also allows the club to
obtain a replacement player to join the 53-man roster).
The interplay between the short-term Inactive List and the longer term Injured Reserve list is particularly
important concerning concussions. As discussed in the full Report, concussions present uncertain
recovery times, are challenging to diagnose and treat, and present particularly acute long-term concerns.
MLB is the only sport with a concussion-specific injured list. Because of these concussion-specific
concerns, we recommend that the NFL also adopt a concussion-specific injured list.
Injury Reporting Policies
There are three variations in the leagues’ injury reporting policies.
First, the NFL, NBA, NHL, and MLS require clubs to disclose publicly players’ injury statuses.
Second, the NFL, NBA, and MLS require clubs to disclose publicly the nature of player injuries. While
the NHL requires clubs to disclose whether a player will miss a game or not return to a game due to
injury, the NFL and NBA (in practice) require that the club identify the player’s body part that is injured.
Below, we make a recommendation concerning this issue.
Third, in MLB, the NBA, the NHL, and MLS, the CBAs specifically describe what type of information
the clubs are permitted to disclose publicly. The NFL CBA is silent on this issue. Instead, NFL clubs
seemingly rely on players’ to execute waivers providing the clubs with permission to disclose publicly
player health information.

!
19!
In the full Report, we discuss in detail three concerns related to the NFL’s Injury Reporting Policy: (1) a
general concern about an individual’s medical information being made publicly available; (2) the
possibility that players will target other players’ injuries that have been publicly disclosed; and, (3) the
Injury Reporting Policy’s role in preventing gamblers from receiving inside information about player
health issues. Ultimately, we believe that it is debatable whether the NFL’s gambling-related concerns
are sufficiently substantial today to justify overriding a player’s right to have his health information
treated confidentially. We lack the relevant expertise, insight, and information, however, to recommend
that the NFL no longer obligate clubs to report information on the status of players. Instead, we
recommend the NFL consider the issue more closely, in addition to other injury-related issues:
• Recommendation 2-A: The NFL, and to the extent possible, the NFLPA, should: (a)
continue to improve its robust collection of aggregate injury data; (b) continue to have the
injury data analyzed by qualified professionals; and, (c) make the data publicly available
for re-analysis.
• Recommendation 2-B: Players diagnosed with a concussion should be placed on a short-
term injured reserve list whereby the player does not count against the Active/Inactive 53
man roster until he is cleared to play by the NFL’s Protocols Regarding Diagnosis and
Management of Concussions.
• Recommendation 2-C: The NFL should consider removing the requirement that clubs
disclose the location on the body of a player’s injury from the Injury Reporting Policy.
Chapter 3: Health-Related Benefits
In this Chapter, we summarize the various health-related benefits available to the players in each of the
leagues. Specifically, for each league, we examine: (1) retirement benefits; (2) insurance benefits; (3)
disability benefits; (4) workers’ compensation benefits; (5) education-related benefits; and, (6) the
existence of health-specific committees jointly run by the league and players association. Each of these
domains is relevant to protecting players should they experience negative health effects during and after
their playing years, and also to promoting their ability to maintain their health and well-being over the
longer term. Given that a decision to play or continue to play professional sports, like many other
decisions, is a matter of weighing risks and benefits, those decisions must be made against a backdrop of
available benefits. It is for this reason that we spend considerable space describing and evaluating the
available benefits in each league.
According to the NFLPA, NFL players have “the very best benefits package in professional sports.” This
claim seems substantially true. First, the NFL offers every benefit that is provided by any of the other
leagues. Second, the NFL offers several benefits that are not provided by any of the other leagues,
including severance pay, long term care insurance, the Former Player Life Improvement Plan, and
neurocognitive disability benefits for former players. Third, there are several benefits that only the NFL
and a limited number of the other leagues provide: (a) only the NFL, MLB, NBA, and NHL provide
health insurance (beyond COBRA) for former players; (b) only the NFL, MLB, and NBA provide players
with mental health and substance abuse treatment; (c) only the NFL and NBA offer a health
reimbursement account; (d) only the NFL and MLB offer disability benefits to former players; (e) only
the NFL and NBA offer education-related benefits for all players; and, (f) only the NFL, NBA, NHL, and
MLS guarantee workers’ compensation benefits to all of their players.
7
!
20!
While overall the NFL thus appears to be the best league for benefits, there are, however, three areas in
which the NFL might appear deficient as compared to one or more of the other leagues.
First, the NFL’s health insurance options for former players appear to be less favorable than those offered
by MLB, the NBA and the NHL. Currently, for players who have vested under the Retirement Plan
(which requires at least three years of Credited Service for players after 1992), the NFL provides the same
health insurance as available to current players for five additional years or the former player can also
obtain health insurance via COBRA. However, COBRA is designed to be a temporary solution and is
generally regarded as expensive relative to other health insurance plans. In contrast, MLB’s Benefit Plan
provides former players the option to continue (or obtain) the same health insurance benefits as current
players for life. While former MLB players have to pay more for their health insurance than current MLB
players, presumably the plans offered are cheaper than COBRA coverage or players would select that
option. Similarly, the NBA’s Retiree Medical Plan is available to former players for life (at varying rates)
and the NHL allows former players who played at least 160 games to continue with the NHL’s insurance
plan for life.
The NFL does offer a variety of health benefits that might partially fill the gap for former players,
including health reimbursement accounts, long term care insurance, benefits for uninsured former players,
and disability benefits. Nevertheless, players often have to go through a difficult process to obtain some
of these benefits after they have already had to pay for the care, or care is delayed until they can obtain
the benefits. We suggest that there may be advantages to allowing former players to continue to obtain
some form of the health insurance that they were able to receive while playing.
Second, as shown in the full Report (Tables 3-J and 3-K) the monthly payments to former NFL players
under the Retirement Plan are seemingly the smallest in the Big Four leagues. Nevertheless, when all of
the benefits available to former players are packaged together, it is likely that the NFL’s benefits are the
most valuable due to the number of benefits that are available. Consequently, lower Retirement Plan
payments might simply reflect the NFLPA’s preferred allocation of total benefits, i.e., a shifting of the
value of benefits away from the Retirement Plan and to other benefits instead. As with health insurance
benefits, the NFL’s Retirement Plan payments require players to undertake relatively little administrative
work to receive benefits and they are a more secure and stable income source and benefit than some of the
other benefits made available by the NFL. Nevertheless, some might believe it is a better use of player
benefit money to fund benefits and programs for former players who are disabled or impaired in some
way as opposed to providing larger Retirement Plan payments to all eligible former players. All of the
benefits available to NFL players must be viewed collectively. For these reasons, we recommend the NFL
and NFLPA consider whether the current allocation of player benefits is the preferred, most just, and most
effective allocation.
Third, MLB and NHL players are vested in their pension plans on the first day they play in those leagues.
By comparison, the NFL requires players to accrue three years of experience (or more depending on when
they played), before they are eligible for retirement benefits (as well as many other benefits). The mean
career of NFL and MLB players are both around five years long. Yet, the NFL’s Retirement Plan likely
excludes and has excluded thousands of former players who did not earn three Credited Seasons. It is
unclear why the NFL requires three years of service (the NBA does as well). The minimum service time
clearly reduces costs for the Retirement Plan, but might also reflect a policy decision as to when an NFL
player has sufficiently contributed to the NFL to deserve pay under the Retirement Plan. Below, we make
a recommendation concerning the vesting requirement for the NFL’s Retirement Plan:
• Recommendation 3-A: The NFL and NFLPA should consider whether change is necessary
concerning player benefit plans.

!
21!
o The NFL and NFLPA should consider providing former players with health insurance options
that meet the needs of the former player population for life.
o The NFL and NFLPA should consider increasing the amounts available to former players
under the Retirement Plan.
o The NFL and NFLPA should consider reducing the vesting requirement for the Retirement
Plan.
Chapter 4: Drug and Performance-Enhancing Substance Policies
This Chapter summarizes the policies of each of the leagues concerning performance-enhancing
substances (“PES”) and drugs of abuse. As explained below, the leagues differ at times in their
categorizations and treatments of different drugs and substances. Where appropriate, we will separate our
analysis of the leagues’ policies by PES and drugs of abuse (collectively “drug policies.”) The leagues’
definitions are discussed at length in the full Report.
With the possible exception of how marijuana is regulated, the Big Four’s drug policies do not vary
substantially. Leagues and unions balance multiple factors in creating drug policies, including but not
limited to deterrence, treatment, privacy, and integrity of the game, and rely on difficult value judgments.
The three features of the policies we view as most important to player health and those which we analyze
are: (1) the availability of Therapeutic Use Exemptions (“TUEs”); (2) the availability of treatment; and,
(3) the opportunity to receive treatment without being subject to initial discipline. With these issues in
mind, we turn to our analysis of how the NFL compares to the other leagues.
Concerning TUEs, the NFL, MLB and the NBA all offer TUEs for both their PES and drugs of abuse
policies. In contrast, the CFL offers TUEs for its PES policy but does not have a drugs of abuse policy.
We also found no evidence that the NHL offers a TUE for its Substance Abuse Program or that the MLS
offers any TUEs. Thus, the NFL’s use of TUEs is at least as good as the other leagues.
All of the leagues, including the NFL, have robust treatment programs for drugs of abuse. However, the
NBA, CFL, and potentially MLS are the only leagues that offer treatment for a player who has violated a
PES Policy. On this issue, the NFL might appear deficient compared to the NBA and CFL. However,
there are other relevant considerations concerning the treatment programs offered to players, discussed
next.
The NFL, NBA, NHL, MLS and maybe MLB provide a safe-harbor for players who voluntarily refer
themselves for treatment for drugs of abuse. These provisions importantly allow players to seek help they
might recognize they need without the fear of immediate adverse employment action.
In contrast, no Big Four league offers a safe-harbor for players who have used PES. It is possible that
these leagues view PES users as players intentionally looking to cheat the game and their competitors,
whereas those using drugs of abuse are in need of medical care. However, there is robust scientific
evidence supporting the need to provide treatment to PES users, as well. PES usage has shown to be
addictive, and has been associated with the use of drugs of abuse (opioids in particular), body dysmorphic
disorder, depression, antisocial traits, mood and personality disorders, other psychological disorders, and
cognitive deficits in impulsivity, risk-taking, and decision-making. As a result, PES users may experience
withdrawal symptoms, and may be at an increased risk of suicide. Consequently, many experts
recommend and provide treatment and counseling for PES users. We adopt that recommendation for
purposes of this Report:

!
22!
• Recommendation 4-A: The NFL should consider amending the PES Policy to provide
treatment to any NFL player found to have violated the PES Policy.
Chapter 5: Compensation
This Chapter examines the form and nature of player compensation in the leagues. In reviewing this
Chapter, it is important to understand that the structures, operations and finances of the “Big Four” are
considerably different from those of the CFL and MLS due to, among other things, their long histories
and the amount of their revenues (billions versus millions).
Compensation is an important component of player health. First, the different compensation structures
and systems in the leagues can influence players’ decisions about their physical and mental health, for
example when to play through injury and when to retire. In their efforts to maximize their earnings (and
sometimes, eligibility for various benefits), some players might sacrifice their short- and/or long-term
physical and mental health. The compensation structures dictate when or if a player faces such a trade-off.
Compensation may also be related to health in a second way. Without adequate savings and benefits
during and after NFL play, players may find themselves insufficiently prepared to meet their physical and
mental health needs, especially in the event of crisis. In addition, as we discussed in greater detail in
Chapter 3, crises in physical and mental health are closely tied to bankruptcy, home foreclosure, and other
serious financial setbacks. NFL players suffer these outcomes as well, despite their relatively high (but
short-lived) compensation.
We are most concerned with how compensation and compensation structures affect player behavior and
decision-making concerning their health, i.e., what are the consequences of the current compensation
regimes on players’ short- and long-term health. Unfortunately, these are questions that we cannot fully
answer at the present.
To effectively and rigorously compare how the different leagues’ compensation structures affect player
health decisions would require the ability to control for a range of variables, including but not limited to
free agency rules, salary and contract limitations, salary cap structure, the level of guaranteed
compensation, career length, career earnings, and injury outcomes. This is a challenging analysis that
requires more data than is currently available and thus we cannot fairly assess which leagues’ overall
compensation structures among the Big Four are best for players.
Some have suggested that NFL player health could be improved through guaranteeing more of their
compensation, which would potentially mitigate pressure to play through injuries in order to protect a
player’s status on the club. On this and related issues, many would argue that MLB’s system is the most
player-friendly, because compensation is almost entirely guaranteed, there is no hard Salary Cap, there is
no maximum salary, and, there is no maximum contract length. It is thus not surprising that, as of
February 2017, the 23 largest contracts among these sports leagues are all for MLB players. However,
MLB players are not guaranteed a share of the revenue like in other leagues and must wait six years
before becoming an Unrestricted Free Agent, the longest wait of the Big Four; thus, it is not clear that
their compensation arrangement is preferable.
The NFL and NFLPA are frequently criticized—by players, the media and academics, among others—for
what is perceived as the lack of guaranteed contracts as compared to the other leagues. However, the issue
is complicated, as discussed in detail in the Report, including the effect of guaranteed compensation on
opportunities for less proven players, and the possibility of reduced compensation and roster sizes. As a
preliminary matter, when discussing the compensation paid to players, one must also consider the other

!
23!
benefits the players receive. As is discussed in Chapter 3 of this Report, the NFL provides a benefits
package superior to those offered in all of the other leagues. We nonetheless make the following
recommendation:
• Recommendation 5-A: The NFL and NFLPA should research the consequences and
feasibility of guaranteeing more of players’ compensation as a way to protect player health.
Chapter 6: Eligibility Rules
Each of the leagues has rules governing when individuals become eligible to play in their leagues. While
we fully acknowledge the unique nature and needs of the leagues and their athletes, we believe the
leagues can learn from the other leagues’ policies.
Leagues’ eligibility rules affect player health in two somewhat opposite directions: (1) by potentially
forcing some players who might be ready to begin a career playing for the leagues to instead continue
playing in amateur or lesser professional leagues with less (or no) compensation and at the risk of being
injured; and, (2) by protecting other players from entering the leagues before they might be physically,
intellectually, or emotionally ready. As discussed in the full Report and recommendation, the NCAA’s
Bylaws are an important factor in considering the eligibility rules and their effects on player health.
The leagues’ eligibility policies vary. MLS has the most liberal eligibility policy, with no minimum age
requirement, while, by requiring several years of college, the NFL and CFL are the most restrictive.
All of the eligibility rules seemingly are at least partially concerned with when a player is “ready” to enter
a professional league. Readiness is an important concept, but difficult to define. In our view, a player is
ready when he is able to enter the league safely, in terms of protecting his health, and maximize his
success across various domains, including physically, mentally, and emotionally. Each of the leagues,
often through negotiations with the unions, has made a judgment as to when they think the typical player
is ready, or at least ready enough. In so doing, the leagues have helped protect clubs from drafting and
investing in players who are not ready, and also potentially helped to protect players who need more time
to prepare for a successful and healthy career. However, without more empirical analysis, we cannot say
for certain when players—individually or collectively—are ready and thus whether the eligibility rule is
fair or successful. No such data currently exists and would be challenging to gather.
The comparison of the leagues’ policies highlights two clear issues with the NFL’s eligibility rule, but,
generally, neither is of the NFL’s making.
First, the NFL’s requirement that players effectively play at least three years of college football might
ensure that only sufficiently physically mature players enter professional football, but it also requires
players to risk their physical health longer without getting paid—and in a sport with higher injuries rates
than that of the other leagues, as discussed in Chapter 2: Injury Rates and Policies. While the NCAA’s
Exceptional Student-Athlete Disability Insurance program tries to alleviate some of these issues, players
have legitimate concerns that they will suffer a career-altering or ending injury before they are able to
reach the professional level and earn any money from their athletic skills. This is at least in part a result of
the NCAA’s prohibition on student-athletes being compensated. Whether the NCAA’s rules are fair is
beyond the scope of this Report, but it is clear that the rules create a problem for players who have the
potential to reach the NFL but who are required—or might prefer—to continue playing college football.
Second, in light of the fact that players are not paid for playing in college, it is understandable that many
want to enter the NFL as soon as possible. Specifically, players will want to enter the NFL after their

!
24!
junior year of college, the first time they are permitted under the NFL’s eligibility rule. However, whether
the player is ready to leave college for the NFL is a difficult question to answer and may not be resolved
until many years later—if ever. If the player is undrafted, NCAA rules effectively prohibit the player from
returning to college football, and the player’s football future is in serious doubt. Once again, although this
problem intersects with the NFL’s eligibility rule, it is the primary result of the NCAA’s rules, not the
NFL’s.
It is challenging to assess the reasonableness of the NFL’s current eligibility rule. The rule seemingly
prevents players from joining the NFL before they are ready, which both protects those players from
injury in the NFL and protects the clubs from investing in players who are not yet ready to play at a
professional level. While there are likely to occasionally be players who are ready to join the NFL before
the end of their junior season, there are going to be outliers to any rule and, without data suggesting
otherwise, we cannot say the NFL’s eligibility rule is unreasonable or not sufficiently considerate of
player health. For this reason our main recommendation is for the NFL to continue to gather data to
permit a better evidence-based evaluation of its current policy, as well to consider the interplay of its rules
with the NCAA’s:
• Recommendation 6-A: The NFL should consider performing or funding research analyzing
when a player might be “ready” for the NFL.
• Recommendation 6-B: The NFL should reconsider the interplay of its eligibility rules with
the NCAA’s rules as they concern player health and take appropriate action if necessary.
Conclusion
This Report begins by explaining the pressing need for research into the overall health of NFL players;
the need to address player health from all angles, both clinical and structural; and the challenges presented
in conducting such research and analysis. The issues and parties involved are numerous, complex, and
interconnected. To address these issues—and ultimately, to protect and improve the health of NFL
players—requires a diligent and comprehensive approach to create well-informed and meaningful
recommendations for change.
We believe part of that comprehensive approach is for the NFL and NFLPA to learn from other
professional sports leagues when possible. In many respects, the leagues and their games are very
different and thus it can be challenging to draw comparisons. Nevertheless, the leagues face a series of
common issues, such as labor negotiations, stadiums and arenas, fan interest, multimedia platforms, and
many others. But perhaps the most important issue is player health. In recent years, each of the leagues
has had to make a fresh and comprehensive examination of its player health policies and practices. We
anticipate the leagues will continue to engage in this examination for many years to come.
As demonstrated by our Report’s analysis and recommendations, the leagues have the opportunity to
learn a great deal from one another in light of their shared interest in player health. Additionally, our
Recommendations are only as useful as their implementation. For these reasons, we make the following
final Recommendations.
• Final Recommendation 1: The leagues and unions should continue to coordinate on player
health issues and to consider each other’s policies and practices.
• Final Recommendation 2: The media, academics, the leagues, and the unions should
continue to police the advancement of player health.
!
25!
***
NFL football has a storied history and holds an important place in this country. The men who play it
deserve to be protected and have their health needs met and it is our fervent hope that they will be met.
We hope this Report furthers that cause.
Summary Table of Recommendations
1. Pre-season physicals for the purpose of evaluating a player’s prior injuries should be performed
by neutral doctors. (Recommendation 1-A).
2. The NFL, and to the extent possible, the NFLPA, should: (a) continue to improve its robust
collection of aggregate injury data; (b) continue to have the injury data analyzed by qualified
professionals; and, (c) make the data publicly available for re-analysis. (Recommendation 2-A).
3. Players diagnosed with a concussion should be placed on a short-term injured reserve list
whereby the player does not count against the Active/Inactive 53 man roster until he is cleared to
play by the NFL’s Protocols Regarding Diagnosis and Management of Concussions.
(Recommendation 2-B).
4. The NFL should consider removing the requirement that clubs disclose the location on the body
of a player’s injury from the Injury Reporting Policy. (Recommendation 2-C).
5. The NFL and NFLPA should consider whether change is necessary concerning player benefit
plans. (Recommendation 3-A).
6. The NFL should consider amending the Performance-Enhancing Substance Policy (“PES
Policy”) to provide treatment to any NFL player found to have violated the PES Policy.
(Recommendation 4-A).
7. The NFL and NFLPA should research the consequences and feasibility of guaranteeing more of
players’ compensation as a way to protect player health. (Recommendation 5-A).
8. The NFL should consider performing or funding research analyzing when a player might be
“ready” for the NFL. (Recommendation 6-A).
9. The NFL should reconsider the interplay of its eligibility rules with the NCAA’s rules as they
concern player health and take appropriate action if necessary. (Recommendation 6-B).
PREFACE: The Football Players Health Study at Harvard University
In response to ongoing concerns about NFL player health, the 2011 Collective Bargaining Agreement
(“CBA”) between the NFL and the National Football League Players Association (“NFLPA”) added a
number of new health, safety, and welfare provisions. One of these provisions sets aside $11 million per
year through 2021 to be dedicated to medical research.
8
Thus, in the summer of 2012, the NFLPA issued
a request for proposals to conduct original research and scientific exploration to be supported by these
funds, focusing on “new and innovative ways to protect, treat, and improve the health of NFL players.”
The NFLPA’s request for proposals specified a number of areas of particular interest, including sports
medicine, repetitive brain trauma, wellness, aging, and cardiovascular disease. At the top of the list,

!
26!
however, was not a particular medical problem, but instead “Medical Ethics (e.g., examination of health
care contexts to obtain a better understanding of internal morality of these practices, accountability, new
interventions that avoid harms currently incurred, appropriate informed consent in the context of
professional athletics, and consideration of medical care in the labor-management context of professional
football.).”
9
To meet the challenge of protecting and improving player health, it is necessary to move beyond clinical
issues to simultaneously address structural and organizational issues as well. This is true for healthcare
more generally, where it is essential to invest not only in scientific research and development to create
new clinical interventions, but also to invest in systems to efficiently administer those interventions to
patients in need, as well as public health approaches that can help minimize the need for intervention in
the first place. Likewise, to make headway in protecting and improving the health of NFL players, we
must go beyond a single-minded focus on their clinical care and instead implement a more comprehensive
strategy capable of addressing the myriad of stakeholders and contextual factors (past, present, League-
wide, and individual) that play a role in their health. These include not only players’ physical issues and
risk factors, but also their relationships with clinicians, professional motivations, financial pressures, and
family responsibilities, as well as the centrality of their health to their careers, the competitive nature of
the business, constraints on alternative opportunities for many players, and the like. The relevant
stakeholders are similarly varied and extensive.
Thus, when submitting its proposal to the NFLPA, our Harvard team included a variety of critical clinical
projects alongside an equally robust set of law and ethics proposals. We agreed from the outset that a
focus on diagnosing and treating player health issues—while essential—would be insufficient on its own
to comprehensively resolve those issues. Instead, our approach has been to also address precisely those
structural and organizational factors that are so important to player health but would be neglected by a
purely clinical approach.
The NFLPA ultimately agreed, selecting Harvard to receive the funding after a multi-round competitive
process involving several universities. In February 2014, Harvard Medical School entered into an
agreement with the NFLPA to create the “Football Players Health Study at Harvard University.” Drawing
on expertise from across Harvard University, the Football Players Health Study is dedicated to
understanding the causes of conditions NFL players face, with the goal of improving their health and
wellbeing.
The “Law and Ethics Initiative,” led by the Petrie-Flom Center for Health Law Policy, Biotechnology,
and Bioethics at Harvard Law School, encompasses a variety of distinct projects with the primary goal of
understanding the legal and ethical issues that may promote or impede player health, and developing
recommendations to promote player health through structural change.
10
The existence of the Law and Ethics component differentiates the Football Players Health Study from
other studies concerning NFL player health. While there have been many important studies concerning
the medical components of player health, we are not aware of any that have conducted a comprehensive
analysis of the relevant legal and ethical environment.
Additionally, in the Section: Ensuring Independence and Disclosure of Conflicts, we discuss the ways in
which the Law and Ethics Initiative interacted with, but was independent of, both the NFLPA and NFL in
creating this Report.
!
27!
In the Introduction that follows, we will describe the scope of this Report, its goals, process, and
limitations. First, however, it is essential to explain the guiding principles of the Football Players Health
Study as a whole.
Most importantly, the Football Players Health Study is interested in health issues beyond concussions and
neurological trauma. Although we recognize that concussions and their possible long-term sequelae are
on the minds of many, and are among the most critical health issues facing players today, we
simultaneously recognize that player health is larger than concussions alone. Players also have concerns
about cardiac health, arthritis and other joint damage, pain management, and a wide variety of other
issues. Moreover, their primary concerns are likely to change over time from their playing days to
retirement to old age. Thus, we have adopted the following mantra for our work: “The Whole Player, The
Whole Life.” Rather than a myopic approach, we are taking a wide and long view in order to make
players as healthy as they possibly can be over every conceivable dimension of their entire lives.
We approached this project as scholars and social scientists whose goal is to improve NFL player health.
We are independent academic researchers first and foremost, regardless of the source of our funding. We
have no “client” in this endeavor, other than players themselves, and we have no agenda other than to
improve the lives of former, current, and future players. Indeed, the Football Players Health Study is
funded pursuant to money set aside under the 2011 CBA for research designed to help players. Because of
the way the clubs and players split revenues from NFL games and other operations, the funds used for the
Football Players Health Study can reduce the amount of money available to current players in the form of
salary.
11
Thus, the players have chosen to pay for the Football Players Health Study. In addition, although
our contractual relationship is with the NFLPA, that very same contract protects our academic integrity
without exception; no external party has any control whatsoever over our conclusions.
One of our primary concerns is that too little is known about player health. Specifically, too little is
known from a rigorous scientific perspective about the risks and benefits of playing professional football
because available data are insufficient in a variety of respects. For example, “[w]e do not know what
factors exacerbate or mitigate an individual’s risk, including genetics, nutrition, lifestyle, as well as length
of time and position played, and injuries sustained during playing years.”
12
Professional football players
are an elite and unique group of men who must be studied directly and often in large numbers before we
can really understand how football has affected them. Only then can we fully address any health problems
they may have. We come to this work with no pre-existing agenda—we have neither any interest in
ending professional football nor any interest in looking the other way if confronted with compelling data
of its downsides. Again, we are interested only in helping players lead the healthiest and most productive
lives they possibly can. We are committed to going where the science takes us.
Finally, we are forward-looking. Our role is not to evaluate fault or assign blame for player health
problems, and the Football Players Health Study is uninvolved in any litigation related to these issues.
Instead, we are working with a single-minded focus to develop a clear path for addressing and
remediating existing player health problems, and for preventing such problems from continuing or
occurring in the future—from both clinical and organizational perspectives. Although this process does
include assignment of shared responsibility for protecting and promoting players’ health to a wide variety
of parties, the past is relevant only to the extent that it demonstrates ways to successfully improve going
forward.
These are the guiding principles motivating every aspect of the Football Players Health Study at Harvard
University.
!

!
28!
INTRODUCTION
This Report seeks to improve the health of NFL players (former, current, and future) by comparing
policies, and, where information is available, practices, in the NFL to other elite professional sports
leagues. The leagues share considerable similarities—at their core, they are organizations that coordinate
elite-level athletic competitions for mass audiences. In this respect, the leagues are competitors within the
professional sports industry, with each of them competing for fans’ dollars and attention. The practices
and policies by which the leagues operate are thus often very similar. However, there are also differences
between the leagues. This Report seeks to identify and understand those different policies and practices
that have the possibility to affect player health. Organizations operating within the same industry often
can learn better practices and policies from one another. While leagues and their games are different in
many important respects, making it impractical and unfair to opine as a definitive matter on which of the
leagues’ policies and practices in their totality best protect player health the Report generally concludes
that the NFL’s policies concerning player health appear superior to the other leagues. Nevertheless,
through the nine recommendations contained in this Report, we hope to elucidate several ways in which
the NFL can learn from other leagues and further protect player health.
With the purpose of this Report in mind, the remainder of this Introduction provides additional
background information on the subject matter of the Report and then further introduces the Report by
describing its audience, articulating the process we used to develop our ultimate recommendations, and
clarifying important points about scope.
A. The Leagues
This Report analyzes the policies and practices of the following professional sports leagues:
• The National Football League (“NFL”): The world’s premier professional football league,
consisting of 32 member clubs. The NFL began play in 1920, has its headquarters in New York
City, and is led by Commissioner Roger Goodell. The NFL’s 2017 revenues are estimated to
reach $14 billion.
13
• Major League Baseball (“MLB”): The world’s premier professional baseball organization,
consisting of 30 member clubs. MLB began play in 1903,
14
has its headquarters in New York
City, and is led by Commissioner Rob Manfred. MLB’s 2016 revenues were an estimated $10
billion.
15
• National Basketball Association (“NBA”): The world’s premier professional basketball league,
consisting of 30 member clubs. The NBA began play in 1946, has its headquarters in New York
City, and is led by Commissioner Adam Silver. The NBA’s 2016–17 revenues are projected to be
approximately $8 billion.
16
• National Hockey League (“NHL”): The world’s premier professional hockey league, consisting
of 30 member clubs. The NHL began play in 1917, has its headquarters in New York City, and is
led by Commissioner Gary Bettman. The NHL’s 2015–16 revenues were an estimated $4.1
billion.
17
• Canadian Football League (“CFL”): A professional football league consisting of 9 member
clubs, all of which are located in Canada. The CFL began play in 1958, has its headquarters in
Toronto, and is currently looking for a new Commissioner. The CFL’s revenues are an estimated
$200 million annually.
18
!
29!
Although both are professional football leagues, the NFL and CFL playing rules vary in several
important ways. Some of the key distinctions include: (1) in the NFL, a team has four downs to
advance the ball ten yards, while in the CFL a team only has three downs; (2) an NFL field is 120
yards long (including two ten-yard end zones) and 160 feet wide, while an CFL field is 130 yards
long (including two twenty-yard end zones) and 65 yards wide; (3) in the NFL, goalposts are at
the back of the end zone while in the CFL they are on the goal line; and, (4) in the NFL, players
in the backfield are not allowed to be moving forward when the ball is snapped, while in the CFL,
all offensive backfield players (except the quarterback) can be moving forward at the snap.
The NFL’s skill level is considered by most outside observers as superior to the CFL. Many CFL
players aspire to make the NFL while many players who were unable to make it in the NFL turn
to the CFL.
• Major League Soccer (“MLS”): A professional soccer league consisting of 20 clubs. As is
explained in further detail in Chapter 5, Section F: Compensation in MLS, MLS is uniquely
organized—rather than having each club owned and controlled by a different person or entity
(like in the other sports leagues), all of the clubs in MLS are owned and controlled by Major
League Soccer, LLC, a Delaware limited liability company.
19
The reasoning for this structure is
discussed in Chapter 5. MLS began play in 1996, has its headquarters in New York City, and is
led by Commissioner Don Garber. MLS’ 2016 revenues were an estimated $600 million.
20
Soccer, as a global game, has dozens of professional leagues around the world. Although MLS
has made strides and is an internationally respected league, it is not the world’s premier soccer
league. The European leagues, such as the English Premier League, Bundesliga in Germany, and
La Liga in Spain are generally considered the best in the world. Nevertheless, we chose to focus
our review on MLS for a few reasons: (1) the European leagues are organized and regulated in
materially different ways than MLS and American sports leagues; (2) the European leagues
generally are not governed by CBAs or a labor-management dynamic like in MLS and North
American sports leagues; and, (3) European laws on a variety of relevant issues are materially
different from American (and Canadian) laws. For these reasons, MLS was the best soccer league
from which to draw useful comparisons to the NFL.
We chose these leagues because of their similarity to the NFL, both structurally and legally. The NFL,
MLB, NBA, and NHL are particularly similar. Each of these leagues has been operating for nearly a
century (or more in the case of MLB) and is an entrenched part of the American sports and cultural
landscape. They share similar structures and operational practices, at least in part because they have
shared many executives, lawyers, stadiums, and fans over the years. Their revenue streams also dwarf
those of any other professional sports leagues, including the CFL and MLS. For these reasons, the NFL,
MLB, NBA, and NHL are commonly referred to collectively as the “Big Four” sports leagues.
21
Where
appropriate, we also adopt this moniker.
We nevertheless acknowledge that other sports and sports leagues can provide lessons for the NFL and
the other sports leagues concerning player health.
22
Sports of all kinds present health risks and rewards to
their athletes and thus how those sports manage those risks and rewards is relevant. We have not
undertaken this analysis here, focusing instead on the sports and leagues most similar to the NFL.
B. The Unions
!
30!
Each of the leagues discussed in this Report has an important counterpart. The leagues are the constructs
of the individual clubs (or operator-investors in MLS) and thus are principally interested in protecting and
advancing the rights of the clubs. To protect and advance their rights and interests, the players in each of
the leagues have formed a players association, a labor union empowered with certain rights and
responsibilities under federal labor laws.
23
The players associations are:
• National Football League Players Association (“NFLPA”): The NFLPA was formed in 1956,
24
has its headquarters in Washington, DC, and is led by Executive Director DeMaurice Smith.
• Major League Baseball Players Association (“MLBPA”): The MLBPA was formed in 1953,
25
has its headquarters in New York City, and is led by Executive Director Tony Clark, a 15-year
MLB veteran.
• National Basketball Players Association (“NBPA”): The NBPA was formed in 1954,
26
has its
headquarters in New York City, and is led by Executive Director Michelle Roberts.
• National Hockey League Players Association (“NHLPA”): The NHLPA was formed in 1957,
27
has its headquarters in Toronto, and is led by Executive Director Don Fehr, who served as
Executive Director of the MLBPA from 1985–2009.
• Canadian Football League Players Association (“CFLPA”): The CFLPA was formed in
1965,
28
has its headquarters in Stoney Creek, Ontario, and is led by President Scott Flory, a 15-
year CFL veteran.
• Major League Soccer Players Union (“MLSPU”): The MLSPU was formed in 2003,
29
has its
headquarters in Bethesda, Maryland, and is led by Executive Director Bob Foose.
The principal right and purpose of the unions is to negotiate with the leagues concerning many of the
policies examined in this Report, as is discussed in the next Section.
C. Collective Bargaining Agreements
Nearly all of the policies and practices that we discuss in this Report are contained in and governed by
collective bargaining agreements (“CBA”) agreed to by the league and its respective players association.
In this Section, we provide a brief explanation of CBAs to provide context for and assist in the
comprehension of the Report.
Pursuant to the National Labor Relations Act (“NLRA”), the unions are “the exclusive representative[] of
all the employees in [the bargaining] unit
30
for the purposes of collective bargaining in respect to rates of
pay, wages, hours of employment, or other conditions of employment.”
31
Also pursuant to the NLRA,
each league’s clubs, acting collectively as the league, are obligated to bargain collectively with the unions
concerning the “wages, hours, and other terms and conditions of employment” for the players.
We acknowledge that many commentators believe that MLBPA has historically been the strongest union,
and that the NFLPA has been regarded as having been less effective by comparison.
3233
However,
complexity and nuance belie any easy comparisons. For context, the NFLPA’s union membership is
roughly the same size of all of the other major unions combined and NFL players generally have shorter
careers than other athletes, creating challenges for building and maintaining solidarity among the players.
Ultimately, the CBAs speak for themselves as the result of the negotiations between the leagues and the
unions. Rather than speculate on the leagues’ and unions’ approaches to player health, we can objectively
!
31!
analyze the collectively bargained provisions and policies. Nevertheless, the ability to effectuate change,
including the areas in need of change highlighted in this Report, is a function of each union’s strength.
Since the 1960s, the Big Four leagues and their respective players associations have each negotiated
approximately ten to 15 CBAs.
34
The CBAs are hundreds of pages long and govern nearly every aspect
of the sports. Collective bargaining is inherently a give-and-take dynamic where the negotiating power
and leverage of each side plays an important role in the outcome. Both league and union leadership and
the dynamics between the leagues and unions have changed over time, resulting in varied CBA
negotiations and results. Nevertheless, generally speaking, most important changes in leagues’ policies
and practices are the result of the CBA process. Consequently, CBAs are of paramount importance to
understanding how the leagues function and making recommendations for improvement.
The CBA represents the key covenant between players and club owners, on all matters pertaining to
player health (alongside many other important issues that matter to these parties). The most
straightforward way to implement many of the changes we recommend to protect and promote player
health would be to include them in the next CBA. That said, whenever change is possible outside of the
CBA negotiating process, it should not wait. Moreover, although the CBA will often be the most
appropriate mechanism for implementing our recommendations, we do not want to be understood as
suggesting that player health should be treated like just another issue for collective bargaining subject to
usual labor-management dynamics. As an ethical matter, players should not be expected to make
concessions in other domains in order to achieve gains in the health domain. To the contrary: player
health should be a joint priority, and should not be up for negotiation.
Finally, it is important to clarify our writing process concerning the MLB-MLBPA CBA. MLB reviewed
a draft of this Report in the fall of 2016 and provided comments in September 2016. We made edits based
on those comments and asked MLB for additional information in October 2016. On November 30, 2016,
MLB and the MLBPA agreed to the terms of a new CBA.
35
On December 2, the league and union issued
a joint press release providing the terms of the new CBA,
36
and on December 14, the MLB owners and
the MLBPA Executive Board (consisting of player representatives) ratified the new CBA.
37
Nevertheless,
as of the date that our Report went to press on March 18, 2017, the full length CBA had not yet been
publicly released. Thus, while we were able to update the Report based on the information contained in
the joint press release, additional details, nuance or context may be contained in the full length CBA when
it is publicly released. On February 27, 2017, we provided MLB with the sections of this Report relevant
to MLB, including those which were edited based on the press release about the new CBA. In March
2017, MLB provided additional comments on the revised sections of the Report before it went to press.
D. Audience
This Report has several key audiences. There are those that we see as the major change agents: current
players; club owners; the NFL; the NFLPA; club medical staff; and, various player advisors (e.g., contract
advisors, financial advisors, and family members). If change is to occur, these are the key individuals and
entities that will need to effectuate it. But we live in an era where discussions about protecting and
promoting player health extend far beyond these change agents. Fans, the media, the NFL’s business
partners, and others all have a stake in—and more importantly, some power to shape—how the policies
and practices of NFL football will evolve to best protect and promote player health. Finally, while our
focus is on promoting the health of NFL players, much of what we have learned and discuss here is likely
useful to the other leagues as well.
Writing for such divergent audiences is a significant challenge. Ultimately, we decided to err in favor of
providing a more comprehensive analysis, with all the complexity and length that entails.
!
32!
E. Goals and Process
This Report has four functions. First, to identify the various policies that do or could influence the health
of players in the various leagues. Second, to describe the policies and their relation to protecting and
promoting player health. Third, to evaluate the capacity of these policies to protect and promote player
health, in particular, by comparing policies on similar issues. And fourth, to recommend changes to
policies that affect NFL players grounded in our evaluation of certain approaches taken by other leagues
that appear to be more favorable.
It is worth describing those functions in greater depth.
1. Identify
To arrive at the policy domains analyzed herein, we considered for potential analysis any policy or
practice that can, does, or should affect player health. Our prior Report, Protecting and Promoting the
Health of NFL Players: Legal and Ethical Analysis and Recommendations, offers a comprehensive
analysis of stakeholders and issues affecting NFL player health. That Report mapped a wide variety of
issues, and this Report more closely examines how the NFL and other leagues have handled some of
them. This Report includes six Chapters analyzing different policies concerning player health: (1) Club
Medical Personnel; (2) Injury Rates and Policies; (3) Health-Related Benefits; (4) Drug and Performance-
Enhancing Substance Policies; (5) Compensation; and, (6) Eligibility Rules.
One important limitation to the domains we include in this Report deserves explicit discussion. This
Report focuses primarily on written policies and rules. We have intentionally avoided analysis about
unwritten practices within the leagues, which is a practical limitation to our work. The policies we have
analyzed are generally codified in the CBAs and other documents and can easily be reviewed. To
accurately understand unwritten practices would require gathering substantial data from individuals
working in the leagues. For example, understanding the relationship among clubs, club medical
personnel, and players—and the ways in which these relationships might vary among the leagues—is
interesting and important. However, without collecting data from representative portions of both players
and club medical personnel in all of the leagues, we cannot fairly compare club medical personnel
practices across the leagues. Gathering such data is beyond the scope of the current project. Therefore, we
focus on the written policies that govern club medical personnel.
We similarly researched the role and practices of clubs, coaches, agents, and financial advisors
concerning player health across the different leagues. However, again, reliable data about the practices of
these groups across each of the leagues—as opposed to their policies—generally does not exist and is
challenging to gather. Such information would clearly be useful, and thus we encourage others to conduct
such research if sufficient funding and access to the relevant populations can be obtained. However, for
practical purposes, this Report focuses primarily on the relevant policies in each of the leagues. By
understanding these policies, we can understand the range of relationships and actions expressly permitted
and analyze whether existing policies could allow for or give rise to potentially problematic situations
could arise.
2. Describe
As discussed above, our analysis of the leagues’ policies stemmed largely from reviewing the CBAs and
other publicly available policies and documents, such as court filings, medical studies, law review
articles, and news articles. To supplement our review, in some cases we requested that the leagues and/or
unions provide us with information and documents that were not otherwise available. The leagues and
unions provided varying degrees of cooperation:
!
33!
• The NFL provided documents and information relevant to our prior report, Protecting and
Promoting the Health of NFL Players: Legal and Ethical Analysis and Recommendations, as well
as this Report. However, the NFL declined our invitation to review this Report.
• The NFLPA provided documents and information relevant to our prior report, Protecting and
Promoting the Health of NFL Players: Legal and Ethical Analysis and Recommendations, as well
as this Report. The NFLPA was also provided with a draft of this Report to review but did not
provide comments.
• MLB provided documents and information that we requested, reviewed the Report, and provided
comments.
• The MLBPA declined our invitation to review the Report.
• The NBA provided documents and information that we requested, reviewed the Report, and
provided comments.
• The NBPA was provided with a draft of this Report to review but did not provide comments.
• The NHL reviewed the Report but declined to provide specific comments. The NHL stated
“[w]ith respect to NHL-related information contained in the draft report, there are numerous
factual and data-related inaccuracies. By way of example, the report references and relies upon
certain outdated/superceded (sic) NHL/NHLPA policies and procedures. In addition, certain of
the cited analytical data appears to be inaccurate. As a result, analysis of and conclusions drawn
from such policies, procedures and data are flawed.”
38
In response to this statement, on multiple
occasions we requested additional information or specification about those items the NHL
believed were inaccurate. The NHL did not respond.
In addition, the NHL declined to provide copies of the following requested documents: (1) the
NHL/NHLPA Authorization Form for Health Care Providers to Release Health Information; (2)
the NHL/NHLPA Concussion Program Authorization Form; (3) the Authorization for
Management and Release of Neuropsychological Test Results; (4) the Substance Abuse and
Behavioral Health Program; (5) the Prohibited Substances List for the Performance Enhancing
Substances Program; and, (6) the NHL Concussion Protocol.
• The NHLPA reviewed the Report and provided comments and relevant documents. The NHLPA
requested that the following statement appear in the Report to explain its involvement:
The NHLPA is pleased to have been able to respond to the authors’ request for
comments regarding a late draft of the study, and to provide certain of the
information requested. The information and comments were provided to the
authors of the study on the strict understanding that they were not to be attributed
to the NHLPA in the text of the study, either directly or by implication. Nothing
in the study, including the study’s decision not to address a question or issue, is
to be construed as reflective of the position of the NHLPA.
• MLS declined our invitation to review the Report and declined to provide relevant documents,
including a Medical Policies and Procedures Manual and MLS’ injury reporting policy.
• The MLSPU provided documents and information that we requested, reviewed the Report, and
provided comments.
• The CFL provided some degree of cooperation by providing some information during a telephone
call. However, after that call, the CFL declined to provide additional information or documents
and declined our invitation to review the Report.
39
!
34!
• The CFLPA provided documents and information that we requested, and was provided a draft of
the Report to review but did not provide comments.
As a result of the varying degrees of cooperation from the leagues and unions, we were not able to
explore certain issues as deeply as we would have liked, in particular the relationships among clubs, club
medical staff, and players. We again highlight this and other practices as areas calling for further research,
provided the leagues provide the necessary access and information.
Importantly, while the leagues and unions had the opportunity to comment, and their comments in many
instances did inform the content of this Report, we retained control over the final content of the Report.
We carefully considered the comments from the leagues and unions and made changes we determined
were appropriate but no reviewer had the authority to demand that any change be included. Thus, review
should not be considered an individual endorsement of any part of the final Report.
3. Evaluate
Once we understood the leagues’ varying policies, we could compare and contrast them. In cases where
other leagues had policies that differed from the NFL we asked, “If the NFL adopted this policy, would it
improve player health?” In doing so, we were careful to take into account the leagues’ different
circumstances and motivations. Nevertheless, in certain situations, we were able to identify gaps and
opportunities for better protecting and promoting the health of NFL players. On the other hand, in some
instances, we discovered that the NFL has more protective policies in place than other leagues, indicating
that the learning from this Report can be multi-directional.
4. Recommend
The primary goal of this Report is to make recommendations that improve the overall health of NFL
players. Our analysis is thus principally focused on understanding other leagues’ policies and practices
and comparing them to the NFL’s. As will be shown in this Report, it would be reasonable to conclude
that overall the NFL’s policies and practices concerning player health are the most protective of player
health among the leagues. However, there are still some areas in which the NFL might learn lessons as
compared to one or more comparator leagues and we have made corresponding recommendations.
Additionally, even though our analysis likely reveals many areas in which other leagues can and should
improve concerning the health of their players, as described above, it is beyond the scope of this Report to
make those recommendations—we focus only on advancements for NFL players.
For every recommendation we describe both the reason for the change and, where applicable, potential
mechanisms by which it may be implemented. However, we avoided being overly specific or prescriptive
when multiple options for implementation may exist, and/or when we lacked sufficient information to
determine which mechanism might be best.
While we consider and discuss a wide range changes that could improve player health, we purposefully
chose to focus on actionable recommendations that could be realistically achieved between the
publication of this Report and execution of the next NFL-NFLPA CBA.
40
This pragmatic approach does
not mean that we are giving relevant stakeholders a pass to simply accept the many current barriers to
change that may exist, but it does recognize that change may be difficult in this complex web of
relationships and in a culture that has developed over the course of many decades and is deeply
entrenched. Furthermore, certain changes might require further information, research, or discussion than
we were able to achieve in this Report. When we concluded that was the case, we so indicated by
recommending only that a change be “considered” or that additional information be sought. Our
!
35!
recommendations may not be easy to achieve, but we have taken into account various realities in making
them.
Finally, it is important to recognize that we do not view our recommendations as the exclusive changes
that the various stakeholders should consider. We do, however, view these as minimum next steps
forward—a floor, not a ceiling.
Appendix A is a compendium of all of the recommendations made in this Report. As discussed above, the
NFL’s policies concerning player health on the whole appear superior to the other leagues. Consequently,
we include only nine recommendations in this Report. This is not to say there are not other areas in which
the NFL can improve player health. Indeed, in our Report Promoting the Health of NFL Players: Legal
and Ethical Analysis and Recommendations, we included 76 recommendations for improving player
health directed at a variety of stakeholders, including the NFL and NFLPA. This Report is focused only
on those Recommendations that are derived from an understanding of other leagues’ policies.
F. Scope
As already alluded to, the scope of this project is to generate legal and ethical recommendations that will
improve the overall health of NFL players, current, future, and former. To fully grasp what is to come, it
is essential to clarify these parameters.
As described at length in the Introduction to our Report Promoting the Health of NFL Players: Legal and
Ethical Analysis and Recommendations, we adopt a broad definition of health that extends beyond the
sort of clinical measurements that might immediately be evoked by the phrase. We maintain the
importance of considering the full range of non-medical inputs that can influence health, also known as
the “social determinants of health.” These social determinants extend beyond the sorts of things for which
one would seek out a doctor’s care, and include broadly “the conditions in which people are born, grow,
live, work, and age,” as affected by the “distribution of money, power, and resources at global, national
and local levels.”
41
Indeed, the NFL’s Player Engagement Department itself includes “physical strength,”
“emotional strength,” “personal strength,” and “financial strength” within its concept of “total
wellness.”
42
Ultimately, for the purposes of all of our work, we define health for purposes of this Report as “a state of
overall wellbeing in fundamental aspects of a person’s life, including physical, mental, emotional, social,
familial, and financial components.”
In making recommendations regarding NFL player health, we have taken as our threshold the moment
that a player has exhausted or foregone his remaining college eligibility and has taken steps to pursue an
NFL career—from that point on, what needs to happen to maximize his health, even after he leaves the
NFL? The reason we have selected this frame is not because the health of amateur players—those in
college, high school, and youth leagues—is secure or unimportant. Instead, the reason is largely
pragmatic: there is only so much any one report can cover. We recognize that what happens at the
professional level can have a trickle-down effect on the culture of football across the board, and also that
some amateur players may be taking health risks in hopes of eventually reaching the NFL, even when that
may be highly unlikely. Nonetheless, our goal with this Report, prompted by the limited scope of the
request for proposals for this project and in part by the fact that further analysis will be possible by others,
is only to address the already complicated set of factors influencing the health of NFL players, current,
future, and former.
That said, many of our recommendations will be most relevant to current and future players, simply
because former players may not continue to be engaged with or affected by many of the stakeholders that

!
36!
we are analyzing, or may be past the point at which implementation of particular recommendations could
help them. For example, no matter what improvements we recommend related to club doctors, these
simply could not affect players who are no longer affiliated with any club.
CHAPTER 1: CLUB MEDICAL PERSONNEL
This Chapter discusses the role of club medical staff, including both doctors and athletic trainers, in each
of the sports leagues as set forth in the leagues’ various controlling policies, most principally, the CBAs.
In particular, we focus on: (1) the types of medical personnel required, if any; (2) the medical personnel’s
obligations; (3) the obligations of the players concerning club medical personnel; (4) the relationship
between the medical personnel and the clubs; and, (5) the existence of sponsorship arrangements between
medical personnel and the clubs, if any.
Our focus here is on the structural issues that are generally governed by the CBA or other policies rather
than how each individual club hires and supervises its medical personnel and how individual medical
personnel interact with individual players, matters that are not the subject of extensive reporting or
publicly available research. By understanding what is required or permitted pursuant to the CBA or other
policies we can understand the scope of possible practices, including those that might be concerning as
they relate to player health.
To provide context for the policies we examine in this Chapter, it is important to provide background on
the subjects most relevant to player health. We discuss those below, and then provide background on two
additional issues relevant to club medical personnel and this Chapter, before reviewing the policies of
each league.
Subjects Relevant to Player Health
There are a wide variety of laws, statutes, regulations, and ethical codes that govern the actions of sports
medical professionals. For example, the American Medical Association (“AMA”)’s Code of Medical
Ethics (“AMA Code”)
43
governs the conduct of nearly all doctors, and contains multiple provisions
applicable to the duties and obligations of club doctors. Similarly, the leading sports medicine
organization, Fédération Internationale de Médecine du Sport (“FIMS”), publishes a Code of Ethics.
44
And, for athletic trainers, the National Athletic Trainers Association (“NATA”) has a fairly robust Code
of Ethics.
45
The full panoply of laws, statutes, regulations, and ethical codes and their application to professional
sports is complex and discussed at length in our prior Report: Protecting and Promoting the Health of
NFL Players: Legal and Ethical Analysis and Recommendations. Here, we identify some of the principles
discussed in that Report most relevant to understanding the different leagues’ efficacy in protecting and
promoting player health: (a) quality of medical care; (b) disclosure and player autonomy; (c)
confidentiality; and, (d) conflicts of interest. While we do not organize the Chapter by these issues, they
served as the framework for our analysis and we thus elaborate on them here.
a. Quality of Medical Care
Playing professional sports comes with a risk of injury that likely exceeds most traditional employment
situations. Moreover, a player’s health is essential to his performance and career longevity. Consequently,
it is important that players have access to high quality healthcare and healthcare that is suited to meet their
sport-specific needs. In this respect, we are interested in whether the leagues have policies that require
certain types of medical professionals and certain certifications that are likely to be most responsive to a
!
37!
professional athlete’s healthcare needs. Additionally, we are interested in whether the leagues clarify the
standard of care to be provided to players.
b. Disclosure and Player Autonomy
There is broad support in law and ethics for a patient’s right to autonomy—the right to make his or her
own choices concerning healthcare.
46
A key correlate of a patient’s right to make his or her own
decisions is the obligation of the healthcare provider to disclose relevant medical information. Players are
patients too and deserve the same protections we all seek in our medical decision-making.
47
As it
concerns professional sports leagues, we are interested in what types of information or records the clubs
are required to provide to players, what type of healthcare options are available to players outside of the
club, and what level of control the club retains over the player’s healthcare choices.
c. Confidentiality
One of the fundamental principles of the doctor-patient relationship is that a patient’s medical information
must be treated confidentially.
48
However, this principle is put under pressure in situations where an
employee’s health is relevant to the employee’s ability to perform his job, and his healthcare is provided
in the employment context, both of which are the case in professional sports. While we recognize club
interests and rights in accessing certain player health information, appropriate safeguards are needed in
dictating the degree to which player medical information can be disclosed and disseminated. We look
carefully to see which leagues have put such safeguards in place and to what extent. We also examine
confidentiality protections when a player obtains care from a healthcare professional outside of the club,
including whether the club has any rights to view that information.
d. Conflicts of Interest
Club medical staff—such as doctors and athletic trainers—are clearly fundamental to protecting and
promoting player health. However, they face an inherent structural conflict of interest. This is not a moral
judgment about them as competent professionals or devoted individuals, but rather a simple fact of the
current organizational structure of their positions, in which they simultaneously perform at least two roles
that are not necessarily compatible. On the one hand, they are hired by clubs to provide and supervise
player medical care. As a result, they have a legal and ethical responsibility to protect and promote the
health of their player-patients, in line with players’ interests as defined by the players themselves. This
means providing care and medical advice aligned with player goals, and also working with players to help
them make decisions about their own self-protection, including when they should play, rest, and
potentially retire.
On the other hand, clubs engage medical staff because medical information about and assessment of
players is necessary to clubs’ business decisions related to a player’s ability to perform at a sufficiently
high level in the short- and long-term. Additionally, clubs engage medical staff to advance the clubs’
interest in keeping their players healthy and helping them recover as fully and quickly as possible when
they are injured. These dual roles for club medical staff may sometimes conflict because players and
clubs often have conflicting interests, but club medical staff are called to serve both parties. We examine
what the leagues are doing (or are not doing) to protect players from these conflicts.
Similarly, many healthcare organizations are interested in being associated with professional sports clubs
to enhance their reputation and exposure. Consequently, these organizations seek to enter into a variety of
commercial arrangements with clubs, including some whereby a healthcare organization pays the club for
the right to provide medical care to the players. Such arrangements may raise concerns about how
medical professionals treating players are being selected (e.g., skill or payment) and whether these
!
38!
relationships have the potential to undermine the care provided to players or trust in the healthcare
professionals providing that care.
Additional Introductory Issues
a. Independent Contractors Versus Employees
Where possible, we have provided information concerning whether club doctors in a particular league are
independent contractors or employees of the club. The distinction has important ramifications from a
potential liability perspective vis-à-vis workers’ compensation laws.
Workers’ compensation statutes provide compensation for workers injured at work and thus generally
preclude lawsuits against co-workers based on the co-workers’ negligence.
49
Thus, in cases where the
club doctor is an employee of the club—as opposed to an independent contractor as is the case for most
club doctors—a player’s lawsuit against the doctor is likely to be barred by the relevant state’s workers’
compensation statute. This has been the result in multiple cases brought by athletes against clubs and club
doctors,
50
as well as in cases brought by athletes against athletic trainers,
51
who are almost always
employees of the club. Where the club doctors are independent contractors instead of employees, the
players can pursue medical malpractice cases against the doctor,
52
but the club is not likely to be held
legally responsible for any negligence by the doctor.
53
b. Healthcare in Canada
The second issue worth mentioning now concerns Canadian clubs. MLB (one club), the NBA (one), NHL
(seven), CFL (all nine), and MLS (three) have Canadian clubs. As Canadian and United States laws differ
concerning healthcare, an understanding of the Canadian healthcare system is necessary for any
discussion of the relationship between Canadian clubs and medical personnel.
The Canadian healthcare system is a social, welfare-based system, wherein “access to health care is
viewed as a right” and is financed through government funding.
54
The ten Canadian provinces and three
territories separately administer healthcare plans modeled off of the federal Canada Health Act of 1984.
55
The federal government ensures provincial compliance with the federal template through the threat of loss
of federal funding.
56
Compliant plans must cover “insured services”—a defined term in the Canada
Health Act that includes medically necessary hospital services, hospital facilities, drugs used in hospitals,
medically necessary services rendered by medical practitioners, and medically required surgical/dental
services performed in a hospital. In addition, plans must also meet the five principles of the Canada
Health Act: public administration; provincial portability; universality; comprehensiveness; and,
accessibility.
57
Given the gaps in coverage (for example, drugs outside of hospitals and vision/dental
services performed outside of hospitals are generally not covered), private spending still makes up 29% of
Canadian healthcare expenditures.
58
“As far as delivery of services is concerned, most physicians are independent contractors operating on a
fee-for-service basis.”
59
These physicians receive fees that are fixed through negotiations between medical
associations and provincial governments, and there is no additional billing.
60
To collect payment,
physicians directly bill the provincial medical services association.
61
Physicians providing non-covered
services, however, directly bill patients, who pay through private insurance or out-of-pocket.
62
Of course,
this is different from the United States. Outside of some specific populations, including but not limited to
those covered by Medicare, Medicaid, or the Veterans Affairs healthcare system, most Americans have
private health insurance either through their own insurance plan or one sponsored by their employer.
***

!
39!
With these introductory issues in mind to provide context, we turn now to analyzing club medical
personnel policies in each of the leagues. For each league, we analyze: (1) Types of Medical Personnel;
(2) Medical Personnel’s Obligations; (3) Players’ Obligations; (4) Relationship between Medical
Personnel and Clubs; and, (5) Sponsorship Arrangements.
A. Club Medical Personnel in the NFL
1. Types of Medical Personnel
a. Doctors
The CBA obligates NFL clubs to retain certain kinds of doctors:
• Club Physicians: Clubs must retain
63
a board-certified orthopedic
surgeon and at least one physician board-certified in internal medicine,
family medicine, or emergency medicine. All physicians must also have
a Certificate of Added Qualification in Sports Medicine. In addition,
clubs are required to retain consultants in the neurological,
cardiovascular, nutritional, and neuropsychological fields.
64
• Physicians at Games: “All home teams shall retain at least one [Rapid
Sequence Intubation] RSI physician who is board certified in emergency
medicine, anesthesia, pulmonary medicine, or thoracic surgery, and who
has documented competence in RSI intubations in the past twelve
months. This physician shall be the neutral physician dedicated to game-
day medical intervention for on-field or locker room catastrophic
emergencies.”
65
Of note, these two provisions do not require clubs to retain and have available neurological doctors at the
games. The absence of this requirement is offset by the Concussion Protocol’s
66
requirement that for
every game each club be assigned an Unaffiliated Neurotrauma Consultant to assist in the diagnosis of
concussions.
Most (if not all) of the doctors retained by NFL clubs are members of the National Football League
Physicians Society (“NFLPS”). The stated mission of the NFLPS, founded in 1966, “is to provide
excellence in the medical and surgical care of the athletes in the National Football League and to provide
direction and support for the athletic trainers in charge of the care for these athletes.”
67
Approximately
175 doctors work with NFL clubs,
68
an average of 5.5 per club. The NFLPS holds annual meetings at the
NFL Combine to discuss medical and scientific issues pertinent to its membership.
69
According to the NFLPS, 22 of the 32 clubs’ head orthopedists and 14 of the 32 clubs’ head “medicine”
doctors are board-certified in sports medicine.
70
In addition, although the 2011 CBA requires club
doctors to have a Certificate of Added Qualification in Sports Medicine, currently only 11 out of the 32
head club doctors have such a Certificate. The remaining club doctors were with clubs before the 2011
CBA and were grandfathered in under the new policy.
Notably, the NFLPS does not have a code of ethics for its members.
71
!
40!
b. Athletic Trainers
The CBA dictates the required presence, education, and certification of athletic trainers:
All athletic trainers employed or retained by Clubs to provide services to
players, including any part time athletic trainers, must be certified by the
National Athletic Trainers Association and must have a degree from an
accredited four-year college or university. Each Club must have at least
two full-time athletic trainers. All part-time athletic trainers must work
under the direct supervision of a certified athletic trainer.
72
Each NFL club employs approximately four athletic trainers, including a head athletic trainer and three
assistants. Head athletic trainers have an average of 21.9 years of experience in the NFL, while assistants
average approximately 8.4 years of experience in the NFL.
73
In the 2014 season, 26 athletic trainers had at
least 20 years of experience and eight had more than 30 years of experience.
74
Athletic trainers—unlike
most club doctors—are full-time employees of the club and not independent contractors.
The Professional Football Athletic Trainers Society (“PFATS”) is an organization that represents the
athletic trainers of NFL clubs.
75
“[M]embership in PFATS is limited to those professionally certified in
accordance with the most current NFL Collective Bargaining Agreement and who are employed full-time
as head or assistant athletic trainers by any of the 32 NFL franchises.”
76
PFATS’ mission statement is as
follows:
The Professional Football Athletic Trainers Society (PFATS) is a
Professional Association representing the athletic trainers of the National
Football League. We serve the players of the NFL, the member Clubs,
and other members of the community. Our purpose is to ensure the
highest quality of health care is provided to the National Football
League. We are dedicated to the welfare of our members and committed
to the promotion and advancement of athletic training through education
and research. The Society is founded on the professional integrity and the
ethical standards of our members and the fellowship that exists among
us.
77
PFATS does have a Code of Ethics for its members. However, as discussed in greater depth in our
Report, Protecting and Promoting the Health of NFL Players: Legal and Ethical Analysis and
Recommendations, the Code of Ethics is seriously flawed and requires substantial changes to be
protective of player health.
78
2. Medical Personnel’s Obligations
The CBA requires each NFL club to “use its best efforts to ensure that its players are provided with
medical care consistent with professional standards for the industry.”
79
The CBA expounds on this
provision by articulating its conception of the club doctor’s standard of care:
[E]ach Club physician’s primary duty in providing medical care shall be
not to the Club but instead to the player-patient. This duty shall include
traditional physician/patient confidentiality requirements. In addition, all
Club physicians and medical personnel shall comply with all federal,
state, and local requirements, including all ethical rules and standards
!
41!
established by any applicable government and/or other authority that
regulates or governs the medical profession in the Club’s city.
80
(Emphasis added.)
This CBA provision is susceptible to multiple interpretations. On a generous reading (i.e., one that does
not give the italicized language any special emphasis), club doctors’ primary duty is to the player at all
times. On a less generous reading, the CBA provision demands a primary duty to the player-patient only
in situations where the club doctor is “providing medical care,” and thus is inapplicable when the club
doctor is rendering services to the club. Importantly, however, the way club doctors are currently situated
within the club precludes the two roles from being truly separated, and thereby precludes club doctors
from having their exclusive duty be to the players. This is because at the same time that the club doctor is
providing care to the player, he is simultaneously performing duties for the club by judging the player’s
ability to play and help the club win.
Thus, the club doctor is required by the CBA to provide medical care that puts the player-patient’s
interests above the club’s (in the event these interests conflict), which is as it should be. However, in most
instances—and as seemingly recognized by the CBA—it is impossible under the current structure for the
club doctor to always have a primary duty to the player-patient over the club, because sometimes the club
doctor is not providing care, but rather is advising the club on business decisions, i.e., fitness-for-play
determinations. In other words, the club doctor cannot always hold the player’s interests as paramount
and at the same time abide by his or her obligations to the club. Indeed, a club doctor could provide
impeccable player-driven medical care (treating the player-patient as primary in accord with the CBA),
while simultaneously hurting a player’s interests by informing a club that the player’s injury and
treatment course will negatively impact his ability to play. Thus, under any reading of the CBA provision,
players lack a doctor who is concerned with their best interests at all times—an unacceptable situation.
Relatedly, the CBA provision also seems to require that the care relationship between players and club
doctors be afforded “traditional” confidentiality protections. However, clubs request or require players to
execute collectively-bargained waivers effectively waiving this requirement—and no player refuses to
sign the waiver.
81
Questions might be raised as to whether the players are providing meaningful and
voluntary informed consent in their execution. Players are being compelled to waive certain legal rights
concerning their health without meaningful options. There is no doubt that players execute the waivers
because they fear that if they do not, they will lose their job. Indeed, the waivers (which are collectively
bargained with the NFLPA)
82
permit the athletic trainer and club doctors to disclose the player’s medical
information to club employees, such as coaches and the general manager. Thus, it is unclear what work
this CBA language is doing. Of course, given this communication, it is inevitable that players will be less
than forthcoming about their medical needs, lest it negatively affect their career prospects.
In reviewing a draft of our Report, Protecting and Promoting the Health of NFL Players: Legal and
Ethical Analysis and Recommendations, the NFL rejected our claim that the CBA provision “requires the
traditional patient-physician confidentiality requirements of a private system,”
83
even though the
provision in question specifically says club doctors have a duty to provide “traditional physician/patient
confidentiality requirements.” The CBA provision does not qualify the club doctor’s duty in the context
of the employer-employee relationship. The NFL should abide by its obligations under the CBA.
The CBA also imposes disclosure requirements on club doctors:
All Club physicians are required to disclose to a player any and all
information about the player’s physical condition that the physician may
from time to time provide to a coach or other Club representative,
whether or not such information affects the player’s performance or
!
42!
health. If a Club physician advises a coach or other Club representative
of a player’s serious injury or career threatening physical condition
which significantly affects the player’s performance or health, the
physician will also advise the player in writing. The player, after being
advised of such serious injury or career-threatening physical condition,
may request a copy of the Club physician’s record from the examination
in which such physical condition was diagnosed and/or a written
explanation from the Club physician of the physical condition.
84
Additionally, club doctors are obligated to permit a player to examine his medical records once during the
pre-season and once after the regular season. Club doctors are also obligated to provide a copy of a
player’s medical records to the player upon request in the off-season.
85
Nevertheless, in reality, the NFL
now has an electronic medical record system that permits players to obtain access to their medical records
at any time.
Finally, there are no CBA provisions that address an athletic trainer’s obligations.
3. Players’ Obligations
The CBA and Standard NFL Player Contract impose certain obligations on players concerning their
relationship with club medical personnel.
First, players are required to “undergo the standardized minimum pre-season physical examination and
tests” that are agreed to as part of the CBA.
86
Second, players are obligated to “undergo a complete physical examination by the club physician upon
club request, during which physical examination Player agrees to make full and complete disclosure of
any physical or mental condition known to him which might impair his performance… and to respond
fully and in good faith when questioned by the Club physician about such condition.”
87
Third, players seemingly have an ongoing obligation to report injuries to the club. The CBA permits clubs
to fine players up to $1,770 if the player does not “promptly report” an injury to the club doctor or athletic
trainer.
88
We are not aware of any guidance on what constitutes “promptly report[ing].”
Fourth, whenever a player seeks a second medical opinion or exercises his right to have the surgeon of his
choice perform an operation, the player must first consult with the club doctor if he wishes to have the
club pay for the second medical opinion or surgery.
89
Additionally, if the player sees a second opinion
doctor and wants the club to pay for it, “the Club physician must be furnished promptly with a report
concerning the diagnosis, examination and course of treatment recommended by the other physician.”
90
4. Relationship between Medical Personnel and Clubs
As a preliminary matter, each member of an NFL club’s medical staff is typically chosen by the club’s
front office executives, e.g., the club president or general manager.
91
a. Doctors
Club doctors are affiliated with a wide variety of private practice groups, hospitals, academic institutions,
and other professional sports leagues. Some of these institutions have long-standing relationships with
clubs which often help lead to the doctor being retained by the club. The NFLPA plays no role in the
selection of club doctors other than ensuring they have the qualifications required by the CBA and are
!
43!
properly licensed in the relevant state(s), via Synernet, a third-party vendor jointly selected by the NFL
and NFLPA.
92
Additionally, of the NFL’s 32 head club doctors, two are employees and 30 are
independent contractors.
93
Also, while it is our understanding that club doctors’ contracts are generally reviewed and renewed on an
annual basis, there is very little turnover among club doctors.
Actual statistics and practices of club doctor compensation are difficult to ascertain. In the course of our
research, we were informed by some familiar with the industry that club doctors are generally paid in
relatively nominal amounts compared to what one might expect ($20,000–$30,000).
94
In reviewing a draft
of our Report, Protecting and Promoting the Health of NFL Players: Legal and Ethical Analysis and
Recommendations, the NFL stated that this estimate “grossly underestimates compensation to Head Team
Physicians, Head Team Orthopedists and Head Team Internists.”
95
Nevertheless, the NFL did not provide
alternative compensation statistics.
In addition, despite the relatively high scrutiny club doctors face, it is our understanding that their
contracts with the clubs do not include any type of indemnification whereby the club would pay for the
defense, settlement, or verdict of a medical malpractice claim.
Despite the various challenges, club doctors have a variety of reasons for being interested in the position.
Many of them are sports fans and thus the opportunity to work up close and personal with some of the
best athletes in the world is exciting. From a business perspective, a doctor’s association with an NFL
club could be powerful in terms of professional respect and name recognition, resulting in more patients.
b. Athletic Trainers
Athletic trainers—unlike most club doctors—are full-time employees of the club and not independent
contractors.
Athletic trainers are generally an NFL player’s first and primary source of medical care.
96
Club doctors
are only with the club sporadically during the week of practice and then attend the games, whereas the
athletic trainers are with the club at all times. Players will first meet with the athletic trainer concerning a
medical issue and the athletic trainer then typically determines whether the player should meet with the
club doctor. The athletic trainers and club doctors are in regular communication about players’ conditions
and treatment. The club doctors are responsible for directing and supervising the care of the players by the
athletic trainers.
Players execute waivers permitting the athletic trainer and club doctors to disclose the player’s medical
information to club employees, such as coaches and the general manager.
97
Athletic trainers—in
consultation with the club doctors—thus keep coaches and general managers apprised of players’ injury
statuses during regular meetings so the general manager can make a decision about whether or not to sign
another player in the event a player is unable to play.
98
These waivers effectively undermine the
confidentiality protections outlined in the CBA.
5. Sponsorship Arrangements
The NFL first instituted a Medical Sponsorship Policy in 2004.
99
At its core, the Policy, most recently
amended in 2014, permits clubs to enter into a Sponsorship Agreement
100
with a medical services provider
(“MSP”)
101
, but prohibits such agreements that also include the provision of medical services. Stated
another way, “[n]o Club may enter into a contract for the provision of medical services to its players that
is interdependent with, or in any way tied to a Sponsorship Agreement with a [MSP].” The Medical
!
44!
Sponsorship Policy does not define “interdependent” and instead the NFL reviews the arrangements to
ensure there is no interdependence.
102
The Policy also explicitly declares that clubs are permitted to enter into agreements with MSPs whereby
the MSP obtains the right to advertise itself as an “official” or “proud” “sponsor,” “partner,” or
“provider.”
103
A review of club websites and media guides shows that at least 25 clubs currently have
some type of “official” healthcare sponsor or partner.
Additionally, the Medical Sponsorship Policy does not prohibit MSPs from paying for the right to provide
medical services to players, although, according to the NFLPS, no MSP currently pays for the right to
provide medical services to players. The Policy also does not limit an MSP’s ability to bargain for the
right to provide healthcare to a club by offering discounted or free services.
Importantly, even in situations where an MSP enters into an agreement to provide medical services to a
club but has not entered into a sponsorship agreement of any kind, the MSP can benefit from the
association. The MSP could still identify itself as a healthcare provider for the club on its website and in
advertisements, within the bounds of relevant intellectual property, professional advertising, and
consumer protection laws and regulations. In other words, the MSP likely could not use the club’s logo
without permission or try to make it appear that the club was actively endorsing the MSP’s services. In
2004, the marketing director of Methodist Hospital explained the value of the hospital’s association with
the Houston Texans:
We track phone calls coming in from new patients…. The No. 1 driver of
our calls is the association with our local teams. People say they heard
that Methodist is where the players go, so it must be the best. It’s not a
coincidence that we are the best, but there isn’t a better way to convince
them. That’s a win-win situation.
104
Finally, it is worth noting that institutional MSPs can be a party to the doctor’s contract with the club to
the extent that such an arrangement is necessary for medical malpractice insurance or for practice
privileges.
When asked for its position on medical sponsorship in the NFL, the NFLPA stated only that it “insisted
upon changes that minimized conflicts of interest resulting in changes to the NFL’s Medical Sponsorship
Policy in 2014/15.” The NFLPA declined to provide further detail on the negotiations or what specific
changes it insisted upon, indicating that the discussions were confidential and that the Medical
Sponsorship Policy is unilaterally promulgated by the NFL. The NFLPA indicated that its “sole
objective” regarding the Medical Sponsorship Policy “is to reduce conflicts of interest and to ensure the
best care possible for its members.” Nevertheless, the NFLPA did not indicate that it is opposed to
medical sponsorship agreements. In addition, we recognize the medical sponsorship agreements provide
clubs—and thus the players—with a lucrative source of revenue.
Below are examples of relationships between MSPs, including doctors, and clubs with a discussion of
whether these relationships would be prohibited or permitted by the 2014 Medical Sponsorship Policy.
However, it is important to keep in mind that the 2014 Medical Sponsorship Policy is complex and, at
times, unclear. Additionally, the document is not collectively bargained and there is no generally
available guidance. Thus, what follows is our best interpretation of the Policy. A more detailed discussion
of the Medical Sponsorship Policy can be found in our Report, Protecting and Promoting the Health of
NFL Players: Legal and Ethical Analysis and Recommendations.
105
!
45!
Table 1-A: Arrangements Prohibited by Medical Sponsorship Policy
Description
Explanation
Agreement with MSP to provide medical services to
club on an exclusive basis.
Policy prohibits agreements with MSPs for the
exclusive provision of medical services, thus
enabling clubs and players to seek necessary
medical care elsewhere.
Agreement allowing institutional MSP to select the
doctors mandated by the CBA to provide care to the
club.
Policy prohibits agreements that permit MSP to
select CBA-mandated doctors; these doctors
must be selected by the club.
Agreement with MSP to provide medical services to
club on a non-exclusive basis alongside the right to
post advertisements in the club’s stadium using club
trademarks.
Each of these agreements would be permitted on
its own, but not jointly; policy prohibits medical
services agreements that are interdependent with
Sponsorship Agreements with MSPs.
Agreement with MSP to provide medical services to
club on a non-exclusive basis alongside naming
rights to the club’s practice facility.
Each of these agreements would be permitted on
its own, but not jointly; policy prohibits medical
services agreements that are interdependent with
Sponsorship Agreements with MSPs.
Agreement with doctor to provide medical services to
club on a non-exclusive basis alongside agreement
for his or her institutional MSP to post
advertisements in the club’s stadium using club
trademarks.
Each of these agreements would be permitted on
its own, but not jointly; policy prohibits medical
services agreements that are interdependent with
Sponsorship Agreements with MSPs.
Agreement with doctor to provide medical services to
club on a non-exclusive basis but doctor reports to
institutional MSP concerning care provided to
players
Policy requires doctors to report directly to the
club.
Table 1-B: Arrangements Permitted by Medical Sponsorship Policy
Description
Explanation
Potential Concerns
Agreement with MSP to pay the
club to provide medical services
to club on a non-exclusive basis.
Policy does not prohibit MSPs
from paying for the right to
provide medical services.
Club might choose MSP that is
willing to pay the most rather
than the best MSP.
Agreement with MSP to provide
medical services to club on a
non-exclusive basis, whereby
MSP has agreed to no
compensation or compensation at
rates below the MSP’s standard
rate and market rates.
Policy does not prohibit MSPs
from discounting the costs of
their services for the right to
provide medical services.
Club might choose MSP willing
to charge lowest rates rather than
the best MSP.
Agreement with MSP to provide
medical services to club on a
non-exclusive basis and MSP has
the right to call itself the
“official” doctor or healthcare
provider of the club.
Policy expressly permits
agreements that permit MSPs to
call themselves the “official”
doctor or healthcare provider.
MSP will attach monetary value
to “official designation,” and
alter payment structure as a
result—leading to clubs choosing
MSPs based on reduced rates
rather than skill.
Agreement with MSP to provide
Policy permits MSPs and clubs
Whether the two agreements are
!
46!
medical services to club on a
non-exclusive basis and a
separate agreement to post
advertisements in the club’s
stadium using club trademarks.
to enter into medical services and
Sponsorship Agreements so long
as they are not “interdependent.”
“interdependent” is difficult to
enforce. Implied agreements and
long-standing practices could
result in clubs choosing MSPs
based on Sponsorship
Agreements rather than skill.
Agreement with MSP to pay the
club for the right to call itself the
“official” healthcare provider of
the club and to post
advertisements in the club’s
stadium using club trademarks
but does not actually provide any
medical services to the club.
Policy expressly permits
Sponsorship Agreements with
MSPs “so long as these
agreements do not involve the
provision of medical service to
players.”
Does not directly affect player
health but raises concerns about
whether the general public will
falsely rely on the MSP’s
declaration that it is the “official”
healthcare provider.
In reviewing a draft of our Report, Protecting and Promoting the Health of NFL Players: Legal and
Ethical Analysis and Recommendations, the NFL stated that it “disagree[d] entirely with the conclusions
reached in Table [1]-B,”
106
without explaining why it reads the plain text of the Policy so differently than
we do. The fact that two sets of trained attorneys (those who authored this Report and those at the NFL)
interpret the Policy differently demonstrates that it should be clarified. Ideally, the NFL will make the
Policy public to allow for further discussion and review.
107
As these charts demonstrate, while the NFL has made progress in regulating the payment to and from club
doctors for sponsorship, on a plain reading of the Policy, there are still a number of ethically fraught
arrangements the current Policy appears to leave in place.
108
With this understanding of the NFL policies, we are now ready to begin the comparison to the other
leagues.
B. Club Medical Personnel in MLB
As explained in the Introduction, Section C: Collective Bargaining Agreements, in the fall of 2016, MLB
and the MLBPA agreed to and ratified the terms of a new CBA. However, as of the date this Report went
to press, the parties had not yet published the new CBA. Thus, this Section summarizes the information
contained in the 2012 CBA, with relevant changes revealed
in a joint press release issued by the parties summarizing the changes agreed to in 2016. Additional
details, nuance or context may be contained in the full length CBA when it is publicly released.
1. Types of Medical Personnel
a. Doctors
MLB policy requires “[t]he home Club [to] have a Club physician (medical or surgical) present for every
game.”
109
The home club doctor is also “expected to provide medical coverage for the visiting Club.”
110
In
addition, MLB policy requires each club to appoint a head doctor to be “responsible for all medical
decisions of the Club, and [to] serve as the primary liaison between the Club and the Office of the
Commissioner‘s Medical Director on all medical issues.”
111
A club’s head doctor must be “licensed to practice medicine in the club’s home state and be Board
Certified in his or her specialty.”
112
In addition, club doctors providing medical coverage at games must
!
47!
be “able to handle all common injuries and illnesses that would be expected during a professional baseball
game, including the evaluation and management of concussions.”
113
MLB’s policies concerning club doctors differ from the NFL’s in four important respects. First, while
there are several provisions referencing club doctors in the CBA,
114
there is no CBA provision that
explicitly requires clubs to retain doctors. Second, of the policies that do exist, none are in the CBA,
which permits MLB to change them without MLBPA input or approval. Third, neither MLB policy nor
the CBA requires clubs to retain certain kinds of doctors, whereas the NFL CBA requires clubs to retain a
board-certified orthopedic surgeon at least one physician board-certified in internal medicine, family
medicine, or emergency medicine, and consultants in the neurological, cardiovascular, nutritional, and
neuropsychological fields.
115
Fourth, unlike the NFL, MLB does not require that all club doctors have a
Certificate of Added Qualification in Sports Medicine.
The professional organization for MLB club doctors is the MLB Team Physicians Association
(“MLBTPA”). MLBTPA’s “mission is to maintain the earned trust of the athletes and teams of Major and
Minor League Baseball, as well as the public, by providing the highest quality medical care and services
aimed at securing and enhancing their safety, health and well-being.”
116
The MLBTPA website lists 117
members, an average of 3.9 per MLB club. Research did not reveal an MLBTPA code of ethics specific
to its members.
The 2012 CBA did not require clubs to retain doctors and the publicly released details of the 2016 CBA
do not indicate that anything has changed in that regard. However, the 2016 CBA did make two relevant
additions: (1) clubs are now required to provide access to a sports psychologist;
117
and, (2) MLB and the
MLBPA agreed to jointly retain a dietician to provide recommendations to players and clubs on nutrition
and supplements.
118
b. Athletic Trainers
Like the NFL CBA, the MLB CBA requires the employment of certified athletic trainers:
Each Club shall employ two Certified Athletic Trainers on a full-time
basis. Both trainers will travel with the Club on the road; provided, that
one trainer may remain in the Club’s home city if necessary for the Club
to fulfill its obligations to disabled players who do not travel with the
Club.
Individuals newly appointed as trainers shall be certified by the National
Athletic Trainers Association (NATA) or the Canadian Athletic
Therapists Association (CATA), or shall be physical therapists licensed
by an appropriate state authority.
119120
The professional organization for MLB club athletic trainers is the Professional Baseball Athletic Trainer
Society (“PBATS”). “PBATS mission is to serve as an educational resource for the Major League and
Minor League Baseball athletic trainers. PBATS serves its members by providing for the continued
education of the athletic trainer as it relates to the profession, helping to improve his understanding of
sports medicine so as to better promote the health of his constituency—professional baseball players.”
121
Research did not reveal a PBATS code of ethics specific to its members.
In reviewing a draft of this Report, MLB stated as follows:

!
48!
The insinuation in the report that MLB team physicians and certified
athletic trainers do not have a code of ethics is patently untrue. All MLB
physicians are board certified in their respective specialties and are
obligated to practice medicine under general ethical codes that govern all
licensed physicians, as well as the more specific codes of ethics of the
appropriate licensing bodies and other professional organizations by
which they are a member (e.g., AAOS, AMSSM, etc.). Since all MLB
athletic trainers are members of the National Athletic Trainers
Association and are also licensed by their respective state authorities,
these codes of ethics apply to and govern this group of medical
professionals. MLB takes the position that the duties and obligations of
Club medical representatives are not negotiable subjects of bargaining,
and are not an appropriate part of our CBA.
We understand MLB’s point and revised the report to clarify that there are not codes of ethics specific to
members of the MLBTPA and PBATS. Nevertheless, we disagree with MLB that medical personnel
working with professional sports clubs do not need their own codes of ethics. Club medical personnel
face a variety of complex situations that are not adequately contemplated or addressed by existing codes
of ethics, most notably balancing their obligations to provide care to the player while also advising the
club about players’ health. Codes of ethics adopted by professional organizations for club medical
personnel would supplement existing codes of ethics by providing guidance and tenets for the unique and
competitive environment in which they must operate.
122
2. Medical Personnel’s Obligations
a. Doctors
The CBA contains the following provisions concerning the club doctor’s duties or obligations.
123
First, club doctors are “prohibited from making any public disclosure of a Player’s medical information
absent a separate, specific written authorization from the Player authorizing such public disclosure.”
124
The NFL CBA does not contain a specific prohibition such as this, but the AMA’s Code of Ethics does.
125
Second, “[i]f a player on a visiting Club receives medical treatment from the home Club’s physician,
certified athletic trainer or other medical professional for a work-related injury, a copy of any written
medical evaluation prepared by the home Club’s medical professional shall be provided to the Player and
his Club’s physician.”
126
Third, if a player is a free agent and requests a copy of his medical records from his prior club, the “Club
shall provide such records within 10 days of such request.”
127
Fourth, the CBA requires club doctors to use a standardized medical history questionnaire when
conducting initial physical examinations of players.
128
Fifth, the CBA requires that for a player to be placed on the Disabled List, a standard form of diagnosis,
including an estimated time period for recovery, must be submitted by the club doctor, a copy of which
must be provided to the player.
129
Sixth, the CBA sets forth MLB’s policy concerning the assessment and management of concussions.
130
Club doctors are involved in determining whether a player has suffered a concussion, whether the player
should be placed on the Disabled List, and clearing the player to return to play.
131
!
49!
We turn now to the standard of care for MLB club doctors. When asked specifically about this issue,
MLB directed us to its minimum game day standards and the MLBTPA mission statement, both of which
were discussed above. However, neither the game day standards nor the mission statement sets forth a
standard of care for club doctors specific to MLB club doctors or that goes beyond what is already
required by codes of ethics and relevant law applicable to all doctors. By comparison, the NFL, NHL and
MLS CBAs all set forth standards of care for their club doctors which, in particular, attempt to address the
conflict of interest inherent in having doctors that treat players while also providing services to the club.
132
Also unlike the NFL, MLB policies do not: require club medical staff to inform players about
communications between the medical staff and the club; entitle players to the surgeon of their choice
(discussed further below); or, entitle players to their medical records as a general matter.
Concerning medical records, in reviewing a draft of this Report, MLB “dispute[d]… that players are not
entitled to their medical records as a general matter. The medical records maintained in MLB’s league-
wide electronic medical records system is a player’s legal medical file, and players are entitled to this
information upon request.” While it is useful that players can obtain their medical records upon request,
players would likely view their records more if they were able to access their records without having to
obtain the club’s assistance, as NFL players can.
b. Athletic Trainers
The CBA is also sparse concerning athletic trainers’ obligations. The only provision governing athletic
trainers is their involvement in MLB’s protocol for assessing and managing concussions. MLB’s
concussion protocol requires that players “involved in an incident during a game that is associated with a
high risk of concussion… will be evaluated on the field for a potential concussion by a Certified Athletic
Trainer (‘ATC’) following the National Athletic Trainers’ Association (‘NATA‘) guidelines for
management of sports-related concussions.”
133
As stated above, the player cannot return to play until he
has been cleared by the club doctor.
134
Additionally, MLB regulations require that “[a]ll ATCs comply with the NATA definition of an athletic
trainer, which states that ‘athletic trainers work under the direction of physicians, as prescribed by state
licensing statutes.’”
135
3. Players’ Obligations
Players are subjected to the following requirements concerning their relationships with club medical
personnel.
First, MLB’s Uniform Player Contract requires players, “when requested by the Club, [to] submit to a
complete physical examination at the expense of the Club, and if necessary to treatment by a physician,
dentist, certified athletic trainer or other medical professional in good standing.”
136
While the NFL CBA
requires players to submit to physical examinations, it does not directly require players to submit to
treatment. Nevertheless, in practice, if an NFL player failed to undergo treatment recommended by the
club medical staff, the club could argue that the player failed to fulfill his obligations under the contract.
Second, “[p]rior to undergoing a ‘second evaluation,’ a Player shall inform the Club in writing of his
decision to seek a second medical opinion, and the name of the physician who will be performing the
diagnosis and medical evaluation.”
137
In order for the club to pay for the cost of the second medical
opinion, the doctor providing the opinion must be on a list of doctors created by MLB’s Medical
Advisory Committee and a medical professional designated by the MLBPA.
138
The NFL CBA similarly
!
50!
requires players to consult with the club before seeking a second medical opinion but does not limit a
player’s options to a pre-approved list.
Third, if a player seeks medical treatment from a doctor unaffiliated with the club for a baseball-related
injury, the player must advise the club in advance and obtain the club’s authorization for the treatment.
139
The player does not have to notify the club of consulting with another doctor if the player does not
receive treatment for the injury, and is not invoking his right to have the club pay for a second medical
opinion.
140
Additionally, a player does not have to advise the club about treatment for a non-baseball-
related injury, provided the injury does not affect his ability to play.
141
4. Relationship between Medical Personnel and Clubs
MLB does not have any policies concerning how clubs select or monitor medical personnel.
142
Club-
doctor relationships, including compensation, duration of a contract, supervisory control, and hiring and
termination, are decisions made by each individual club.
143
Perhaps partially as a result, club doctors’
roles, employment situations, and compensation vary significantly around MLB.
144
In 2004, MLB
attorneys reportedly suggested that clubs consider classifying their doctors as employees in order to
reduce medical malpractice insurance premiums.
145
Despite this report, as in the NFL, most club doctors
are independent contractors and “only a few” club doctors are employees.
146
Clubs retain certain rights concerning a player’s healthcare. Specifically, “the Club has the right to
designate the doctors and hospitals when a Player is undergoing a surgery for an employment related
injury,” but are required to “take a Player’s reasonable preferences into account when designating doctors
to perform surgery[.]”
147
In contrast, NFL players have the right to a surgeon of their choice.
MLB and the MLBPA have collectively bargained a form that permits club medical personnel to disclose
any of the player’s health information to “the Owner, President, General Manager, Assistant General
Manager, Field Manager, Physicians and such medical personnel as they may designate, Certified
Athletic Trainer, Assistant Certified Athletic Trainer, Club Rehabilitation Coordinator, In-House Counsel,
Risk Manager and Workers’ Compensation Coordinator of the Club” “for any purpose relating to [the
player’s] employment as a player for the Club[.]”
148
The player has the right to revoke the authorization
(assuming he signed it).
149
However, any revocation appears to be effectively meaningless because, as
part of the Uniform Player Contract, the player agrees “that the Club’s physician and any other physician
or medical professional consulted by the Player… may furnish to the Club all relevant medical
information relating to the Player.”
150
The club also has the right to provide the player’s medical
information to clubs with which the player’s club is in trade negotiations.
151
MLB’s practices in this
regard are comparable to the NFL, where players generally sign broad waivers permitting clubs to obtain,
use, and disclose their medical information.
Turning to athletic trainers’ practices specifically, like in the NFL, MLB athletic trainers are the primary
caregivers for injuries suffered during the season.
152
Indeed, club doctors are not permitted by MLB
regulations to sit in the dugout.
153
Club doctors reportedly do not travel to regular season away games,
and, instead, the home club’s doctors are responsible for overseeing the healthcare of both the home and
visiting clubs, as well as all managers, coaches, and umpires.
154
MLB regulations also require that athletic
trainers “comply with the [National Athletic Trainers Association] definition of an athletic trainer, which
states that ‘athletic trainers work under the direction of physicians, as prescribed by state licensing
statutes.’”
155

!
51!
5. Sponsorship Arrangements
In 2004, MLB prohibited sponsorship arrangements between clubs and medical providers that included
“the right of the [sponsor] to be the medical service provider for the club’s players and employees.”
156
Under MLB’s policy, clubs must negotiate at arm’s length for medical services, and the Commissioner
must approve all sponsorship agreements with healthcare providers.
157
The Commissioner has approved
such sponsorship arrangements with medical providers where “the Club has had a pre-existing
relationship with the hospital or doctors prior to the sponsorship, and the terms of the health care
agreement were unaffected by the sponsorship.”
158
Additionally, MLB’s medical sponsorship policy is the
result of negotiations with the MLBPA.
159
Nevertheless, MLB’s policy does not prohibit clubs from “enter[ing] into traditional sponsorship
arrangements with [medical service providers] involving, for example, advertising, hospitality or the use
of trademark rights, provided that such agreements are otherwise consistent with Major League Baseball
policy and applicable law.”
160
Thus, it appears that MLB clubs are permitted to enter into sponsorship
agreements with medical service providers so long as those agreements do not involve the provision of
medical care to the players. Indeed, many MLB clubs have sponsorship relationships with regional
healthcare providers.
161
MLB’s medical sponsorship policy is substantially similar to the NFL’s. While there are gaps and room
for interpretation, the general purpose of both policies is to prevent healthcare providers from paying for
the right to provide medical care to the players. Additionally, MLB’s medical sponsorship policy is
slightly less concerning from a player perspective since it was negotiated with the MLBPA. In contrast,
the NFL’s Medical Sponsorship Policy is unilaterally imposed.
C. Club Medical Personnel in the NBA
1. Types of Medical Personnel
a. Doctors
Like the NFL CBA, the NBA CBA requires clubs to retain doctors with certain qualifications:
Each Team agrees to secure the services of at least two (2) physicians as
team physicians. Beginning with the 2017-18 Season, each individual
hired for the first time to perform services as a team physician must be a
duly licensed physician who as of the hiring date: (i) is board certified
and fellowship trained in his/her field of medical expertise; (ii) has at
least five (5) years of post-fellowship clinical experience; and (iii) has
successfully completed a fellowship in sports medicine, has a
Certification of Added Qualification (CAQ) in sports medicine, or has
other “sports medicine” qualifications as the parties may agree.
162
In addition, the CBA provides that:
Each Team has the sole and exclusive discretion to select any doctors,
hospitals, clinics, health consultants, or other health care providers
(“Health Care Providers”) to examine and/or treat players pursuant to the
terms of this Agreement and the Uniform Player Contract; provided,
however, no Team will engage any such Health Care Provider based
primarily on a sponsorship relationship (or lack thereof) with the Team,
!
52!
and without considering the Health Care Provider’s qualifications
(including, e.g., medical experience and credentials) and the goal of
providing high quality care to all of its players.
163
This provision’s application to potential sponsorships will be discussed below.
The professional organization for NBA club doctors is the NBA Physicians Association (“NBAPA”).
164
A
review of NBA club websites and media guides demonstrates that NBA clubs are typically affiliated with
two to three doctors. Research did not reveal an NBAPA code of ethics specific to its members.
However, according to the NBA, the NBAPA By-Laws provide that the first purpose of the organization
is “to achieve the best possible medical care for the professional basketball player.” Finally, NBPA
representatives are permitted to participate in meetings of the NBAPA “for the purpose of discussing
matters related to the medical care and treatment of players.”
165
b. Athletic Trainers
Like the NFL CBA, the NBA CBA dictates the required presence, education, and certification of athletic
trainers:
Each Team agrees to secure the services of at least one (1) athletic trainer
to serve as the Head Athletic Trainer and one (1) athletic trainer to serve
as an Assistant Athletic Trainer on a full-time basis. Beginning with the
2017-18 Regular Season: (i) each individual hired for the first time to
perform services as an athletic trainer for a Team must as of the hiring
date: (a) be certified by the National Athletic Trainers Association
(NATA)
166
or the Canadian Athletic Therapists Association (CATA) (or
a similar organization as the parties may agree), and (b) hold a current
certification in Basic Cardiac Life Support or Basic Trauma Life
Support; and (ii) each individual hired for the first time to perform
services as a Head Athletic Trainer for a Team must, as of the hiring
date, have at least three (3) years of experience as an athletic trainer since
he/she first received the foregoing NATA/CATA certification.
167
The professional organization for NBA club athletic trainers is the National Basketball Athletic Trainers
Association (“NBATA”). The NBATA describes itself as “a professional organization of highly skilled
certified athletic trainers who provide specialized health care and critical support services to the athletes
and organizations of the National Basketball Association.”
168
The NBATA further describes its purpose as
to: “[l]ead the management and practice of exceptional health care; [p]rovide continuing education to our
members; [p]rovide education and conduct basketball-related sports medicine research to benefit our
athletes, the National Basketball Association, and the National Basketball Athletic Trainers Association,
and our communities; [and,] [u]phold the athletic training profession’s highest moral and ethical
standards.”
169
According to the NBATA, there are 57 athletic trainers, approximately 1.9 per club.
Research did not reveal an NBATA code of ethics specific to its members, beyond its statement of
purpose.
The role of NBA athletic trainers is similar to that of athletic trainers in the other leagues. Athletic trainers
are typically with the club at all times, are the player’s first line of medical care and will liaise with
doctors and other medical professionals as necessary.
170
!
53!
2. Medical Personnel’s Obligations
The NBA CBA contains two notable provisions concerning club medical personnel’s obligations.
171
First, the CBA requires that “a player requiring the care and treatment of an orthopedic surgeon will, as
far as practicable, be referred to and treated by one (1) orthopedic surgeon (rather than several.)”
172
Second, the club must provide a player with his medical records within 48 business hours of the player’s
request.
173
In contrast, the NFL CBA only entitles players to their medical records once during the pre-
season, once after the regular season, and upon request in the off-season.
174
However, in practice, the
NFL’s electronic medical records system provides players with 24/7 access to their medical records.
Similarly, the NBA CBA says that one of the goals of its electronic medical records system is to “give
players the ability to easily access their own health information” but it is unclear whether there is a portal
through which players can access their medical records 24/7.
In addition to the above CBA provisions, according to the NBA, the NBA Operations Manual also
regulates medical personnel’s obligations including but not limited to their “timing of presence at games,
handling of situations involving blood, gloves, washing skin surfaces, cleaning procedures for skin, and
additional obligations under cardiac and concussion screenings, prescription drug policies, etc.”
Notably, unlike the NFL, no NBA policy sets forth the standard of care for club doctors. Also unlike the
NFL, NBA policies do not: require club medical staff to inform players about communications between
the medical staff and the club; or, entitle players to the surgeon of their choice. The NBA CBA—like the
NFL’s—does entitle players to their own medical records.
The 2017 NBA CBA did, however, introduce an interesting CBA provision that is worth discussing. In
the event the NBA, a club or the NBPA
has been advised by a physician that a player is medically unable and/or
medically unfit to perform his duties as a professional basketball player
as a result of a potentially life-threatening injury, illness or other health
condition and/or that performing such duties would create a materially
elevated risk of death for the player, then the NBA, a Team, or the
Players Association may refer the player to a Fitness-to-Play Panel….
Once so referred, the player will not be permitted to play or practice in
the NBA until he is cleared to do so by the Panel[.]
175
Beginning in 2017, the NBA and NBPA are creating Fitness-to-Play Panels with respect to: (i) cardiac
illnesses and conditions; and, (ii) blood clots and other blood conditions and disorders, and will consider
others as necessary.
176
The three-member Panels are to consist of expert doctors in these fields, with one
doctor appointed by the NBA, one doctor appointed by the NBPA, and the third doctor appointed by the
first two doctors.
177178
The determination to be made by the Panel is whether, in the panel’s
reasonable medical judgment and experience, and having considered
current medical knowledge and the best available objective evidence: (i)
the player is medically able and medically fit to perform his duties as a
professional basketball player; and (ii) performing such duties would not
create a materially elevated risk of death for the player.
179
!
54!
If a player’s condition is referred to a Fitness-to-Play Panel, prior to the Panel’s review of his condition,
he must “(on behalf of himself, his heirs and assigns)… sign a release and covenant not to sue agreement
in the form agreed upon” by the NBA and NBPA.
180
Similarly, if the player is cleared to play, the player
must sign an “informed consent and assumption of risk agreement” in a form agreed to by the NBA and
NBPA.
181
These forms are not publicly available, and thus we cannot opine on whether they comport
with applicable law and codes of ethics.
Nevertheless, even if the Panel clears the player to play, the club is not required to let him play or
practice.
182
Instead, if the club continues to believe that the player should not play, within 60 days the club
must trade the player, release him from the club or amend his contract in such a way that might enable
him to play.
183
The “Fitness-to-Play” provision is, as far as we know, unprecedented in professional sports and
seemingly arises out of a challenging situation in the NBA. In February 2015, Miami Heat star player
Chris Bosh was diagnosed with a blood clot in his calf muscle, that later spread to his lungs.
184
As a result,
Bosh missed a significant portion of the Heat’s games in the 2014-15 and 2015-16 seasons.
185
Then, in
September 2016, with the 2016-17 season approaching, Bosh failed his physical with the club when the
Heat’s doctor determined Bosh’s need for blood thinners made playing professional basketball too
risky.
186
Bosh’s desire to continue playing may have prompted the creation of the Fitness-to-Play Panels
though, as of February 2017, it is unclear whether Bosh intends to utilize the process.
187
The new Fitness-to-Play Panels are interesting and innovative but new. Thus, we recommend that the
NFL monitor their use and consider their potential application to the NFL. In its review of the Report, the
NBA indicated its belief that the Fitness-to-Play Panels are an important new right for players. However,
we note that NBA clubs retain considerable discretion in choosing whether to play players and thus it is
unclear how much value the Panels provide to players. Lastly, we note that the Fitness-to-Play provision
may implicate the Americans with Disabilities Act and/or the Genetic Information Nondiscrimination
Act. For more on the intersection of these statutes and professional sports, see our law review article,
Evaluating NFL Player Health and Performance: Legal and Ethical Issues, 165 U. Penn. L. Rev. 227
(2017).
3. Players’ Obligations
NBA players are entitled to a second medical opinion at the club’s expense provided the player’s injury or
illness meets one of the following criteria:
(i) has prevented the player from participating in a Regular Season or
playoff game for two (2) weeks or more; (ii) in the opinion of a Team
physician for the player’s Team, is more likely than not to prevent the
player from being able to participate in an NBA game for two (2) weeks
or more (or during the off-season, from participating in competitive
basketball without restriction for two weeks or more); (iii) in the opinion
of the Team physician will not be significantly aggravated by the player
continuing to participate in NBA games (or during the offseason
participating in basketball without restriction) when the player
reasonably believes that continued participation will significantly
aggravate his injury, illness or condition; (iv) results in direction from the
Team physician that the player should undergo surgery; or (v) results in
direction from the Team physician that the player should not undergo
surgery when the player reasonably believes that surgery is necessary for
the injury, illness or other health condition.
!
55!
Additionally, the club will only cover the cost of the second medical opinion if: (1) the doctor providing
the second medical opinion is from a list of doctors jointly maintained by the NBA and NBPA;
188
and, (2)
prior to obtaining the second medical opinion, the player provides the club with the “name of the
physician who will be performing the evaluation, and the date and location of the evaluation.”
189
The circumstances under which NBA players can obtain second opinions are limited as compared to
players’ options in the NFL. NBA players can only obtain second opinions in the above described
scenarios whereas NFL players can obtain a second opinion whenever they would like, provided that if
the club is to pay for the second opinion, the player first consults with the club doctor. Nevertheless, NBA
players’ rights to a second opinion was only added as part of the 2017 CBA. It thus remains to be seen
how the provision operates in practice. For example, NBA players may be able to obtain second opinions
as freely as NFL players.
Despite the player’s right to obtain a second medical opinion, the club is only required to “consider the
second opinion in connection with [the player’s] diagnosis or treatment” (emphasis added).
190
In other
words, the club doctor’s opinion as to the proper course of treatment controls even if it conflicts with the
second opinion doctor’s opinion. If the player fails to comply with the club doctor’s recommended
course of treatment, it is possible the player could be found to be in violation of his obligations under his
contract, including “to keep himself throughout each NBA Season in good physical condition.”
191
While
this provision potentially provides club doctors with the authority to determine the course of treatment
against a player’s wishes, we are not aware of any circumstance in which that has been the case.
Nevertheless, this arrangement contrasts with the situation in the NFL, where the CBA does not grant
club doctors the ultimate authority to determine the diagnosis and treatment for the player. In practice,
players are generally free to follow the course of treatment recommended by the second opinion doctor, a
clear positive for NFL players.
In addition to obligations in order to obtain a second medical opinion, the NBA Uniform Player Contract
imposes several requirements on players concerning their cooperation with the club’s medical personnel.
First, a player must “provide to the Team’s coach, trainer, or physician prompt notice of any injury,
illness, or medical condition suffered by him that is likely to affect adversely the Player’s ability to render
the services required under [his] Contract, including the time, place, cause, and nature of such injury,
illness, or condition.”
192
NFL players are similarly obligated to report their injuries.
Second, “[s]hould the Player suffer an injury, illness, or medical condition, he will submit himself to a
medical examination, appropriate medical treatment by a physician designated by the Team, and such
rehabilitation activities as such physician may specify.”
193
NFL players are also obligated to submit to a
medical examination but are not obligated to follow the treatment recommended by the club medical staff.
Instead, NFL players are entitled to a second medical opinion and the surgeon of their choice.
Third, a player must “submit to a physical examination at the commencement and conclusion of each
Contract year… and at such other times as reasonably determined by the Team to be medically
necessary.
194
Relatedly, players are required to “submit to reasonable screening and baseline testing (e.g.,
pursuant to NBA cardiac and concussion protocols) and, in connection with such screening and testing,
shall accurately and completely answer all reasonable health questions (including, upon request,
providing accurate and complete medical histories).”
195
Again, NFL players are also obligated to submit
to medical examinations and to provide an accurate medical history.
Fourth, a player must “at the commencement of [his] Contract, and upon the request of the Team…
provide a complete prior medical history.”
196
Similarly, the Standard NFL Player Contract and
!
56!
standardized minimum pre-season physical both require NFL players to provide a complete medical
history.
Fifth, a player must “supply complete and truthful information in connection with any medical
examinations or requests for medical information authorized by [his] Contract.”
197
“A player who knows
he has an injury, illness, or condition that renders, or he knows will likely render, him physically unable
to perform the playing services required under a Player Contract may not validly enter into such Contract
without prior written disclosure of such injury, illness, or condition to the Team.”
198
If a player does not
make the required disclosure, he risks having his contract voided. The Standard NFL Player Contract
imposes similar disclosure obligations on NFL players.
Sixth, if a player “consults or is treated by a physician (including a psychiatrist) or a professional
providing non-mental health related medical services (e.g., chiropractor, physical therapist) other than a
physician or other professional designated by the Team [the player] shall give notice of such consultation
or treatment to the Team and shall authorize and direct such other physician or professional to provide the
Team with all information it may request concerning any condition that in the judgment of the Team’s
physician may affect the Player’s ability to play skilled basketball.”
199
The NBA CBA imposes this
obligation on players regardless of whether the club is paying for the outside consultation or treatment. In
contrast, the NFL CBA does not require NFL players to make their clubs aware of treatment sought
outside of the club’s medical staff unless the player wishes to have that care paid for by the club.
Seventh, “[a] Player who engages in five (5) or more training or workout sessions with a trainer,
performance coach, strength and conditioning coach, or any other similar coach or trainer other than at the
direction of the Team (each a “Third-Party Trainer”), shall give notice of such training or workout to the
Team prior to the first such training or work out (sic) session, provided that if the player does not initially
plan to continue working with any such Third-Party Trainer for five (5) or more sessions, such notice
must be provided no later than prior to the fifth such session.
200201
The NFL does not contain any
requirement for players to give notice to their clubs of training with third-party trainers.
Eighth, a player is required to “execute such individual authorization(s) as may be requested by the
Team… or as may be required by health care providers who examine or treat the Player.”
202
Although the
NFL CBA does not require players to execute authorizations permitting disclosure of their medical
information, in practice all players execute such authorizations.
4. Relationship between Medical Personnel and Clubs
Our research was unable to determine how many NBA club doctors are employees versus independent
contractors. We also were unable to find reliable information about the typical compensation of NBA club
doctors. The NBA also did not provide non-public information concerning club doctors’ employment
relationships and structures.
203
Clubs are permitted broad access to player medical information. Club doctors are permitted to “disclose
all relevant medical information concerning a player to (i) the General Manager, coaches, and trainers of
the Team by which such player is employed, (ii) any entity from which any such Team seeks to procure,
or has procured, an insurance policy covering such player’s life or any disability, injury or illness such
player may suffer or sustain, and (iii)… the media or public on behalf of the Team.”
204205
Clubs
considering acquiring a player via trade are also entitled to a player’s medical records.
206
Additionally,
according to the NBA, “[e]ach player in the NBA signs a health information authorization form each
season that references disclosure to the media.” These policies are similar to the practices of NFL clubs,
whereby players execute waivers permitting broad disclosure and use of their medical information.
!
57!
5. Sponsorship Arrangements
As discussed above, the NBA CBA prohibits clubs from retaining medical personnel or entering into
agreements with healthcare providers to treat players if those agreements are “based primarily on a
sponsorship relationship.”
207
Thus, the NBA does not prohibit agreements whereby a healthcare provider
pays for the right to be the club doctor and to be a sponsor of the club, provided the sponsorship is not the
primary reason for the relationship. Consequently, it is not surprising that several clubs are engaged in
sponsorship relationships with healthcare providers that include the provision of care to the players.
208
In
this respect, the NBA policy falls short of the NFL and MLB’s general prohibitions on healthcare
providers paying for the right to provide care to players. However, in reviewing a draft of this Report, the
NBA noted the possible difference between policy and practice: stating that “[t]he practical differences of
the NBA and NFL/MLB policies may not be as pronounced as the statement in the report implies.” We
acknowledge this distinction between policy and practice. Without additional information concerning
medical sponsorship arrangements, which the leagues were generally unwilling to provide, we cannot
fully evaluate the effects of the leagues’ different medical sponsorship policies.
D. Club Medical Personnel in the NHL
1. Types of Medical Personnel
The NHL CBA, like the NFL CBA, contains robust requirements for club medical personnel.
a. Doctors
The CBA requires doctors to be present at all games:
Each Club shall have a minimum of two (2) team physicians in
attendance at all home games. At least one of the team physicians shall
have successfully completed hockey-specific trauma management
training or Advanced Trauma Life Support training during the previous
three (3) years. Each Club shall have consultant specialists at each home
game (the selection of whom shall be at the discretion of the head team
physician) to complement the skill set of the two (2) team physicians.
Each Club’s team physicians in attendance at home games shall include,
either as part of the two (2) main team physicians or as consultants, (i) an
orthopedist, and (ii) an internal medicine, emergency medicine or
primary care sports physician. At least one of the team physicians shall
have familiarity with the NHL Modified SCAT2 or other comprehensive
standardized acute concussion assessment tool as recommended by the
NHL/NHLPA Concussion Working Group.
209
Since the execution of the CBA, the above requirements have been amended. Clubs are now required to
have three doctors in attendance at each home game, including: (1) an orthopedic surgeon; (2) an internal
medicine or primary care physician; and, (3) a doctor certified and active in emergency medicine. In
addition, now the club’s two primary doctors, their athletic trainers, and any doctor that travels with the
club to away games must be proficient with the X2 SCAT3 App used for evaluating possible concussions.
The CBA also dictates club doctors’ required qualifications:
Each medical doctor hired or otherwise retained by the Club after the
Effective Date of [the CBA] to treat its Players as part of the Club’s
!
58!
primary medical team shall, in the United States be board certified in his
or her respective field(s) of medical expertise, and in Canada be board
certified by either the Royal College of Physicians and Surgeons (for
specialists) or the College of Family Practice of Canada (for family
physicians). Each Club medical doctor who is part of the primary
medical team hired or retained after the Effective Date of this
Agreement, and any head team physician hired or promoted to such
position after the Effective Date of this Agreement, shall have
successfully completed a fellowship in Sports Medicine or have other
“sports medicine” qualifications as the parties may agree.
210
Nevertheless, our research did not reveal a code of ethics specific to NHL club doctors, which was
confirmed to us by one NHL club athletic trainer that reached out to us concerning our work.
211
b. Athletic Trainers
The NHL CBA also requires the full-time employment and presence of athletic trainers:
Each Club shall employ at least two (2) ATs on a full-time basis. In the
event both ATs do not travel with the Club on the road, and to the extent
reasonably necessary in the Club’s reasonable discretion to provide
adequate services and treatment, the Club shall arrange for alternative
means to provide athletic training services by providing at least one AT,
and either an additional AT or other person of equal or greater medical
training, or a massage therapist. All ATs employed or retained by a Club
to provide services to Players must be certified by the National Athletic
Trainers Association (“NATA”) or the Canadian Athletic Therapists
Association (“CATA”), or shall be physical therapists licensed by an
appropriate state or provincial authority and/or certified as a specialist in
physical therapy, and shall hold current certification in Basic Cardiac
Life Support or Basic Trauma Life Support. At least one of the ATs shall
have familiarity with the NHL Modified SCAT2 or other comprehensive
standardized acute concussion assessment tool as recommended by the
NHL/NHLPA Concussion Working Group.
212
An AT shall be available on the bench at all times during games and
practices. If the AT must leave the bench for any reason, either (A)
another AT must be available to immediately replace such AT on the
bench, or (B) another person with equal or greater medical training must
be available to immediately replace the AT on the bench.
213
As with the CBA provision governing club doctors, the parties have also amended the policies governing
athletic trainers. The new policy requires that, when on the road, each club shall arrange to have at least
one athletic trainer and either an additional athletic trainer or a person of equal or greater medical training
available to the players. The revised policy eliminates discretion clubs previously enjoyed as to whether
to provide such services, and now makes this mandatory.
The professional organization for NHL club athletic trainers is the Professional Hockey Athletic Trainers
Society (“PHATS”). PHATS’ stated mission is to:
!
59!
1. Encourage and promote the consistent application of the most advanced
knowledge and techniques of the science of athletic training in the
prevention, treatment, and rehabilitation of sports injuries to professional
hockey players.
2. Function as a professional association for professional hockey athletic
trainers to promote the welfare of its members, the profession of athletic
training, and safe participation in the sport of hockey.
3. Provide for the exchange among its members of current ideas,
techniques, and scientific data relating to the prevention and care of
hockey injuries.
4. Support the continued advancement of the athletic training profession.
214
Nevertheless, research did not reveal a PHATS code of ethics specific to its members, which was
confirmed to us by an anonymous NHL club athletic trainer.
The role of NHL athletic trainers is similar to that of athletic trainers in the other leagues. Athletic trainers
are typically with the club at all times, are the player’s first line of medical care, and will liaise with
doctors and other medical professionals as necessary.
215
2. Medical Personnel’s Obligations
The NHL CBA directs that “[e]ach Club shall provide its Players with high quality health care appropriate
to their needs as elite professional hockey players, including access to health care professionals[.]”
216
Seemingly in accordance with this obligation, the CBA also outlines the required relationship between the
club medical personnel and the players:
The primary professional duty of all individual health care professionals,
such as team physicians, certified athletic trainers/therapists (“ATs”),
physical therapists, chiropractors, dentists and neuropsychologists, shall
be to the Player-patient regardless of the fact that he/she or his/her
hospital, clinic, or medical group is retained by such Club to diagnose
and treat Players. In addition, all team physicians who are examining and
evaluating a Player pursuant to the Pre-Participation Medical Evaluation
(either pre-season and/or in-season), the annual exit examination, or who
are making a determination regarding a Player’s fitness or unfitness to
play during the season or otherwise, shall be obligated to perform
complete and objective examinations and evaluations and shall do so on
behalf of the Club, subject to all professional and legal obligations vis-a-
vis the Player-patient.
217
Above, we discussed problems with a similar standard of care outlined in the NFL CBA. The NFL’s
provision requires that “each Club physician’s primary duty in providing medical care shall be not to the
Club but instead to the player-patient.” However, the NFL’s standard of care fails to account for the club
doctor’s obligations to the club—namely to perform fitness-for-play evaluations. The NHL’s provision
seemingly resolves this concern in part, by requiring—without limitation to the circumstances of
providing medical care—that the Club doctor be subject to his or her obligations to the player “regardless
of the fact that he/she… is retained by such Club[.]”
218
The CBA imposes other health-related requirements on clubs and club medical personnel.
!
60!
First, “If a Player on a visiting team receives medical and/or health diagnosis, treatment, or fitness to play
determination(s)” from the home club medical personnel, the home club must send the visiting club a
written medical report.
219
The NFL CBA has no such provision.
Second, “[e]ach Club shall identify one (1) individual who is responsible for monitoring on an ongoing
basis, or auditing on a regular basis, prescription drugs that have been given to each Player on the Club,
with a particular emphasis on monitoring controlled substances and sleeping pills, if any, that have been
prescribed.”
220
The NFL has no such provision, however, NFL clubs do not store controlled substances
and any prescription drugs are obtained from a retail pharmacy.
221
Third, the club is required to provide a doctor giving a second opinion all relevant medical information
regarding the player, as long as the second opinion doctor is on a “list of medical specialists mutually
agreed upon” by the Joint Health and Safety Committee,
222
a medical advisory committee consisting of
five NHL members and five NHLPA members.
223
The NFL does not explicitly require such cooperation
but, in practice, the second opinion doctor receives all relevant medical information.
224
Fourth, “[a]t the conclusion of each season, the Club shall provide each Player with a complete copy of
his medical records at the time of his annual exit physical (to the extent the Club maintains physical
possession of the Player’s medical records; otherwise the Club’s physician will provide the Player with a
complete copy of his medical records upon the Player’s direction to do so). The exit physical shall
document all injuries that may require future medical or dental treatment either in the near future or post-
career.”
225
This provision is outdated, as the NHL’s electronic medical record system now provides players with
access to their medical records. NFL players are also able to access their electronic medical records at any
time.
226
3. Players’ Obligations
Like the NFL CBA, the NHL CBA provides players the right to a second medical opinion concerning
diagnoses or courses of treatment
227
and the surgeon of their choice, but imposes obligations on players
related to that care.
When seeking a second medical opinion, the player must “advise the Club in writing of his decision to
seek a Second Medical Opinion and the name of the Second Medical Opinion Physician.”
228
The club is
only obligated to pay for the second medical opinion if the player consults with a doctor from the Joint
Health and Safety Committee’s list or otherwise obtains the approval of the club.
229
If the player uses a
doctor from the approved list or approved by the club, the player (or the second opinion doctor) must
provide the club doctor “with a report concerning the diagnosis, examination, and course of treatment
recommended by the Second Medical Opinion Physician[.]”
230
Players do not have to provide the club
with information from a second opinion doctor if the second opinion is obtained outside of the process
outlined in the CBA and if the player arranges and pays for the consultation himself.
If the club doctor and second opinion doctor disagree, the two doctors can agree to have the player
examined by a third doctor.
231
Nevertheless, in the NHL, the club doctor is ultimately entitled to
“determine the diagnosis and/or course of treatment,”
232
including whether “a surgical procedure is the
appropriate course of treatment for the Player.”
233
If the player fails to comply with the recommended
course of treatment, it is possible the player could be found to be in violation of his obligations under his
contract, including “to keep himself in good physical condition[.]”
234235
Nevertheless, we are not aware of
any circumstances in which surgery was performed or recommended against the player’s wishes. In
contrast, the NFL CBA does not set forth how to resolve a dispute between the club doctor and second
!
61!
opinion doctor. More importantly, the NFL CBA does not grant club doctors the ultimate authority to
determine the diagnosis and treatment for the player. In practice, players are generally free to follow the
course of treatment recommended by the second opinion doctor, a clear positive for NFL players.
An NHL player is entitled to the surgeon of his choice, but the club will only cover the cost of the surgery
if the doctor is on the Joint Health and Safety Committee‘s list or is otherwise approved by the club.
236
After any such surgery, the player (or his doctor) must provide the club doctor “with all relevant records
from the surgeon regarding the surgery[.]”
237
The NFL CBA imposes similar requirements.
Finally, if a player wishes to rehabilitate an injury during the off-season in a city of his choice, the player
must obtain permission from the club and send periodic status reports to the club.
238
If the club is not
satisfied with the player’s progress, the club can require the player to continue his rehabilitation in the
club’s city.
239
The NFL CBA does not address player’s off-season training locations.
4. Relationship between Medical Personnel and Clubs
The NHL declined to provide any information concerning the employment or financial relationships
between NHL clubs and their doctors, and our independent research did not uncover more information.
240
The only information we received on this issue was from the anonymous athletic trainer discussed above,
who explained that the club medical staff is typically hired by the club’s general manager.
Most of our information about the relationship between NHL clubs and their medical staff is based on the
CBA itself. The CBA permits clubs to disclose player medical information in a variety of situations. The
CBA requires players to execute three different health-related authorizations: (1) the NHL/NHLPA
Authorization Form for Health Care Providers to Release Health Information; (2) the NHL/NHLPA
Concussion Program Authorization; and, (3) the Authorization for Management and Release of
Neuropsychological Test Results.
241
The content of the authorization forms is unknown, but the CBA
does explicitly allow disclosure of player medical information “as reasonably required for professional
sports operations, between and among a Club’s Club Personnel
242
for purposes related to the Player’s
employment as an NHL hockey Player.”
243
Additionally, club personnel, the NHL and the NHLPA may disclose a player’s medical information: (1)
as required by the player’s Standard Player Contract or the CBA, e.g., determining a player’s fitness to
play; (2) when the information is relevant to a grievance; (3) when the information is relevant to an
investigation of whether the player or club violated the CBA or Standard Player Contract; (4) as permitted
by the authorization forms discussed above; (5) for purposes of the club seeking advice regarding its
rights and obligations; (6) for purposes of injury surveillance and as authorized by the electronic medical
record system; (7) to a club considering acquiring the player via trade; (8) to the player’s agent; (9) as part
of the player obtaining a second opinion; (10) to treat the player in an emergency; (11) to doctors and
individuals involved in managing the Performance Enhancing Substances Program or the Substance
Abuse and Behavioral Health Program; and, (12) to vendors and administrators as necessary.
244
These
disclosure policies are similar to the practices of NFL clubs.
5. Sponsorship Arrangements
Our research has not revealed whether the NHL has a medical sponsorship policy and the NHL declined
to provide any information on the matter. In 2012, the Canadian newspaper The Globe and Mail reported
that at least ten US-based NHL teams had an “official medical provider.”
245
According to the report, these
clubs had a variety of relationships with their healthcare providers, with some clubs paying their club
doctors a salary, others exchanging perks for pro bono services, and a minority of clubs accepting
payment from medical groups.
246
Additionally, some clubs entered into a sponsorship agreement with a
!
62!
medical service provider but independently retained club doctors from outside of that service provider’s
network.
247
The anonymous athletic trainer who contacted us confirmed that in his experience these sponsorship
arrangements exist. The athletic trainer expressed his belief that many NHL clubs enter into long-term
agreements whereby medical service providers such as local hospitals pay the club millions of dollars per
year for the right to provide medical services to the club’s players, including the right to select the club’s
doctors. Moreover, the athletic trainer indicated to us that under these agreements, medical specialists
needed by the players, such as neurologists and ophthalmologists, are chosen by the hospital. In sum, the
athletic trainer expressed his belief that players are “forced” to see doctors from a specific hospital, rather
than the best doctors for the players’ needs. The NHL did not respond to an email asking if the athletic
trainer’s assertions are accurate.
In contrast, as discussed above, the NFL has indicated that its medical sponsorship policy prohibits the
type of arrangement that might occur in the NHL, i.e., where medical service providers pay for the right
to provide care to players. Nevertheless, also as discussed above, the boundaries of the NFL’s medical
sponsorship policy are not clear. Additionally, the NFL’s medical sponsorship policy prohibits
agreements whereby medical service providers provide exclusive care to players, which might be a
problem in the NHL.
E. Club Medical Personnel in the CFL
1. Types of Medical Personnel
Unlike the NFL CBA, the CFL CBA does not require clubs to retain doctors. However, like the NFL
CBA, the CFL CBA does require clubs to retain certified athletic trainers, known in Canada as “Athletic
Therapists”:
Member Clubs shall employ or retain a minimum of one trainer who is
certified by the Canadian Physiotherapists Association and/or the
Canadian Athletic Therapists Association (CATA) or equivalent
qualifications. All head therapists in the C.F.L. must be certified athletic
therapists in good standing with CATA. The head therapists from each
Member Club will be required to submit their CATA certification
indicating that they are in good standing with CATA to the C.F.L. Office
on an annual basis.
248
Nevertheless, a review of CFL club websites reveals that CFL clubs are typically affiliated with five to
ten medical professionals.
249
These professionals typically include orthopedists, emergency physicians,
sports medicine physicians, chiropractors, and optometrists.
250
The clubs also generally employ 3–4
athletic trainers.
251
2. Medical Personnel’s Obligations
The CFL CBA’s only requirement of medical personnel is that they provide players with their medical
records upon request.
252
Unlike the NFL, the CFL lacks policies concerning: (1) the standard of care for club medical personnel;
(2) communications between medical personnel and the club; (3) a player’s right to a second opinion;
and, (4) a player’s right to a surgeon of his choice. The CFL CBA—like the NFL’s—does entitle players
to their own medical records.
!
63!
3. Players’ Obligations
The CFL’s Standard Player Contract imposes only one medical personnel-related obligation on players:
Prior to the start of each football season, the Player shall attend before
the Club’s Medical Committee for a complete physical and medical
examination, and, shall answer completely and truthfully all questions
asked of him with respect to his physical and medical condition[.]
253
The NFL CBA similarly requires players to submit to a pre-season physical and “to make full and
complete disclosure of any physical or mental condition known to him which might impair his
performance… and to respond fully and in good faith when questioned by the Club physician about such
condition.”
254
4. Relationship between Medical Personnel and Clubs
According to the CFL, all CFL club doctors are independent contractors.
255
The CFL’s characterization of
its relationship with club doctors accords with Canadian physicians’ general status as independent
contractors within its government-sponsored healthcare system; however, two 1980s Canadian cases that
considered whether NHL Canadian club doctors were independent contractors or employees for liability
purposes both looked beyond the parties’ understanding of their relationship.
256
Based on the differing
factual scenarios, the British Columbia Supreme Court—which heard both cases—concluded that club
doctors were employees in one case and independent contractors in another. In both cases, the perceived
level of control proved to be dispositive. Thus, a court considering the status of CFL club doctors for
vicarious liability purposes may look beyond the manner in which the club doctors receive compensation
or the title that the league ascribes to clubs’ relationships with doctors. In doing so, the court will likely
examine the degree of control clubs have over the doctors.
Concerning the duties of CFL club doctors, the CBA provides that a club has “the right to conduct a
medical examination at any time[.]”
257
However, the CBA also dictates that a pre-season physical “to
determine the status of any pre-existing condition” is to be performed by a neutral physician.
258
Although there is limited information available on CFL club doctors, in 2007, the Saskatchewan
Roughriders’ club doctor, Dr. Robert McDougall, acknowledged the complications in being a club doctor:
You have a responsibility to the organization for which you work... but in
addition you have a responsibility to the athlete and you can’t function
independently from that athlete. Because you administer care to the
athlete, he/she needs to be fully informed of the events. . . . So I feel like
there is a triad of duties: the organization you work with, the athlete, and
in the end, yourself as a physician. Above all, you have a responsibility
as a physician to make the right medical decision.
259
These concerns were echoed by CFL Hall of Fame player Chris Walby, who explained that there are
many situations “where the physician definitely supports the team before the player.”
260
According to
Walby, the club doctor’s “job is to get you back on the field in as short a time frame as possible.”
261
5. Sponsorship Arrangements
According to the CFL’s former President and Chief Operating Officer, Michael Copeland, no CFL clubs
!
64!
engage in sponsorship arrangements whereby a healthcare provider pays the club for the right to provide
healthcare to the club’s players.
262
The practice of leagues and their member clubs accepting payment
from medical groups is reportedly “frowned upon” in Canada.
263
F. Club Medical Personnel in MLS
MLS’ most recent CBA was agreed to in March 2015. In addition, MLS’ Medical Policies & Procedures
Manual (“MLS Medical Manual”), which is not collectively bargained, provides guidance on these
issues.
264
The MLS Medical Manual is a league-imposed manual with which MLS clubs and their doctors
and athletic trainers are required to comply.
265
1. Types of Medical Personnel
The MLS CBA declares that after its execution, MLS and the MLSPU would “meet to agree on a side
letter/provision to include in the CBA regarding the required number of medical/training personnel each
Team shall retain (e.g., Team physician, athletic trainers, therapists, and appropriate minimum
certification requirements for such personnel).”
266
As of the date of publication, it is unclear whether the
side letter has been executed. Nevertheless, the MLS Medical Manual suggests that MLS clubs “establish
a network” of the following medical professionals:
• Head club physician/chief medical officer;
• Orthopedic sub-specialists (special attention given to foot and ankle specialists);
• Primary care sports medicine;
• Internal medicine;
• Head athletic trainer;
• Assistant athletic trainer;
• Strength and conditioning coach;
• Cardiologist;
• Neuropsychologist;
• Neurosurgeon;
• Dentist;
• Oral and maxillofacial surgeon;
• Massage therapist;
• Physical therapist;
• Chiropractor;
• Nutritionist;
• Podiatrist;
• Dermatologist;
• Ophthalmologist; and,
• Imaging center.
267
The professional organization for MLS club doctors is the MLS Team Physicians Society (“MLSTPS”).
MLSTPS’ stated mission is “[t]o be a global leader and collaborator in the science of soccer medicine
focused on research, education and athlete care.”
268
Research did not reveal an MLSTPS code of ethics
specific to its members.
The corresponding organization for MLS club athletic trainers is the Professional Soccer Athletic
Trainers’ Society (“PSATS”). According to PSATS, the organization “serves to enhance the personal and
professional development of its membership. PSATS strives to provide educational opportunities for its
!
65!
members so they may better serve Major League Soccer, their organization, and the professional soccer
players under their care.”
269
Our research did not reveal a PSATS code of ethics specific to its members.
According to the MLS Medical Manual, MLS athletic trainers are required to be certified by the National
Athletic Trainers Association (“NATA”).
270
However, this is an error and a requirement with which
athletic trainers cannot comply. NATA is a voluntary professional association but does not certify athletic
trainers. Athletic trainers are certified by the BOC.
271
The BOC used to be part of NATA, but split from
the voluntary association in 1989.
272
As in all of the leagues, MLS athletic trainers are the players’ first line of medical care.
273
The athletic
trainers are with the club on a constant basis, preparing them for practices and games, treating conditions
as needed, and updating the club on players’ health statuses.
274
In addition, the athletic trainers liaise with
club doctors when the players need more extensive care.
275
2. Medical Personnel’s Obligations
The CBA directs that “[e]ach Team shall provide its Players with high quality health care that is
reasonably appropriate to their needs as elite professional soccer players, including access to health care
professionals[.]”
276
Seemingly in accordance with this obligation, the CBA also outlines the required
relationship between the club medical personnel and the players:
The primary professional duty of all individual health care professionals
(such as Team physicians, athletic trainers, physical therapists
chiropractors, dentists and neuropsychologists) providing health care to a
Player, shall be to the Player-patient regardless of the fact that the health
care professional or his/her hospital, clinic, or medical group is retained
by such Team to diagnose and treat Players. In addition, all individual
health care professionals, such as Team physicians who are examining
and evaluating a Player shall be obligated to perform complete and
objective examinations and evaluations and shall do so on behalf of the
Team and League, subject to all professional and legal obligations vis-a-
vis the Player-patient.
277
These provisions are almost verbatim replicas of the NHL CBA provisions. Above, we discussed
problems with a similar standard of care outlined in the NFL CBA as compared to the NHL CBA. The
same analysis applies here. The NFL’s provision requires that “each Club physician’s primary duty in
providing medical care shall be not to the Club but instead to the player-patient.” However, the NFL’s
standard of care fails to account for the club doctor’s obligations to the club—namely to perform fitness-
for-play evaluations. The NHL’s and MLS’ provision seemingly resolves this concern in part, by
requiring—without limitation to the circumstances of providing medical care—that the club doctor be
subject to his or her obligations to the player “regardless of the fact that he/she… is retained by such
Club[.]” Nevertheless, we still do not believe the NHL’s and MLS’ provisions sufficiently protect player
health as discussed in the Analysis Section.
In addition to the CBA provision, the MLS Medical Manual directs in multiple provisions some form of
the following: “Club physicians and Athletic Trainers are always expected to comply with the highest
standards of medical care and to use their best professional judgment.”
278
Finally, the MLS CBA also requires clubs to “cooperate with all requests by a Player or former player
and/or his representative(s) for copies of the Player’s or former player’s medical recording, including
!
66!
athletic trainers’ notes, and shall provide such records and notes within fourteen (14) days of any request
by a Player or former player.”
279
3. Players’ Obligations
The CBA imposes numerous health-related obligations on players.
First, as part of the Standard Player Agreement, the player represents that “he knows of no physical or
mental conditions that could impair his ability to play skilled professional soccer during the Term of th[e]
Agreement and he has not knowingly concealed any such conditions[.]”
280
The standard NFL Player
Contract also requires players to represent that they are in “excellent physical condition.”
281
Second, the Standard Player Agreement also obligates a player to “maintain a high level of physical and
mental conditioning and competitive skills, not engage in alcohol abuse, not use drugs or any other
substances in contravention of the MLS Player Substance Abuse and Behavioral Health Program and
Policy, and generally develop and maintain a physical and mental readiness necessary to play for the
Team.”
282
The NFL Player Contract also requires players to “maintain” themselves in “excellent physical
condition.”
283
Third, a player must “immediately… notify the Team’s coach, trainer or physician of any illness or injury
contracted or suffered by him which may impair or otherwise affect, either immediately or over time, his
ability to play skilled professional soccer.”
284
The CBA does not describe the punishment in the event a
player fails to disclose an injury. NFL players are similarly required to report their injuries.
Fourth, “[p]rior to the start (including, during the season, when a Player first joins his Team) and at the
conclusion of each League season, Players shall submit to complete medical examinations by a physician
designated by MLS, at times designated by MLS and at MLS’s expense. Such medical examinations may
include, without limitation, blood tests…. The Player shall answer completely and truthfully all questions
asked of him concerning his physical and mental condition.”
285
The NFL CBA imposes similar
requirements on its players.
Fifth, “[i]n addition to the Pre-season and end of League Season medical and physical examinations,
Players may also be required to submit, on reasonable dates and times at the expense of MLS, to such
reasonable additional medical examinations (including blood tests…) as may be requested by his Team or
MLS.”
286
NFL players are also required to submit to medical examinations.
Sixth, a “Player is required to execute any authorizations required to release all of his medical records to
MLS and/or Team physicians, relevant officials, and to the workers’ compensation insurance carrier of
MLS…. It is understood that medical information relating solely to the reasons why such Player has not
been, is not or may not be rendering services as a Player may be released to the public by MLS or a Team.
A medical information release… shall be executed by each Player during Pre-Season each year or upon
joining MLS during the League Season.”
287
Although the NFL CBA does not require players to execute
authorizations permitting disclosure of their medical information, in practice, all players execute such
authorizations.
Seventh, if a player seeks a second medical opinion and the second opinion doctor disagrees with the club
doctor, “[t]he physician for the player shall evidence his determination by completing [a form], which
shall be provided to the Player’s Team no later than forty-eight (48) hours after completion of the
examination.”
288
If the second opinion doctor and club doctor are unable to resolve the disagreement, the
“relevant medical issue(s)” are determined by a neutral doctor agreed upon by the club’s doctor and the
second opinion doctor.
289
The player is obligated to “promptly submit to treatment recommended by” the
!
67!
club doctor or the neutral doctor, as applicable.
290
If the player refuses to submit to the treatment
recommended by the club doctor, the player is considered in breach of his contract and thus subject to
suspension or termination.
291
In contrast, the NFL CBA does not set forth how to resolve a dispute between the club doctor and second
opinion doctor. More importantly, the NFL CBA does not grant club doctors the ultimate authority to
determine the diagnosis and treatment for the player, or require players to submit to any treatment. In
practice, players are generally free to follow the course of treatment recommended by the second opinion
doctor. However, it is important to remember that NFL players have an obligation to maintain themselves
in excellent physical condition.
292
If the player does not take certain steps to recover from an injury—
including perhaps the treatment recommended by one or more doctors—it is possible that the player could
be found to have breached his contract and thus subject to suspension or termination.
4. Relationship with Clubs
The MLS Medical Manual dictates that clubs are responsible for negotiating agreements with doctors and
athletic trainers for the treatment of players.
293
In addition, while the MLS Medical Manual requires that
athletic trainers be “year-round employees,”
294
there is no direction on whether club doctors should be
employees or independent contractors. Otherwise, we were unable to discover information about the
financial relationships between MLS clubs and their doctors. MLS declined to provide any information
related to these issues. Additionally, according to the MLSPU, there are no “collectively bargained
provisions regarding the relationships between team medical personnel and the clubs.”
295
Some information about the relationships between MLS clubs and their doctors can be gleaned from a
2012 lawsuit filed by former D.C. United player Bryan Namoff against the club, the club’s coach, Tom
Soehn, the club doctor, Christopher Annunziata, and the club athletic trainer, Brian Goodstein.
296
Namoff
alleged that the D.C. United medical staff had failed to properly treat his concussion, resulting in a variety
of physical and mental conditions.
297
In a May 8, 2014, order, a District of Columbia court determined that Namoff’s claims against D.C.
United, Soehn, and Goodstein were barred by workers’ compensation laws.
298
The court noted that
Goodstein was employed by D.C. United as an athletic trainer,
299
and found that MLS and D.C. United
were “concurrent employers” of Namoff.
300
Consequently, the workers’ compensation laws barred
Namoff’s lawsuit against his co-employee Goodstein.
In an August 12, 2014, order, the court found that Annunziata was an independent contractor.
301
The court
based its decision largely on Annunziata’s ethical requirements as a doctor to “make clinical decisions
and exercise his independent professional medical judgment when managing, caring for, and treating
patients.”
302
Additionally, the court found that the MLS Medical Policies and Procedures Manual “directs
team physicians to provide care based on their own ‘best professional judgment’ and recognizes that they
are ultimately responsible’ for treating players.”
303
Thus, because D.C. United could not direct his work,
Annunziata was not an employee of the club.
The court’s order also revealed some interesting details about the relationship between Annunziata and
D.C. United. There was no written contract between the parties and Annunziata was not paid for his
work.
304
Instead, D.C. United provided Annunziata “tickets to games, permissions to use his association
with D.C. United in his promotional and marketing materials, and paid travel expenses.”
305
The arrangement revealed by the Namoff lawsuit comports with the typical arrangements in the NFL,
where the club doctor is generally an independent contractor and the athletic trainer is an employee.
!
68!
As mentioned above, MLS players are required to sign an authorization permitting disclosure of their
medical information. The authorization form is broad.
306
The authorization form permits “all physicians,
hospitals, laboratories, pharmacies, clinics, and other health care providers (including, but not limited to,
all athletic trainers/therapists) (collectively, ‘Health Providers’)” to release the player’s medical
information to:
(a) the Health Providers, coaches, soccer operations staff, player
operations staff, legal staff, human resources staff, owners, executives,
general managers, assistant general managers, and other officials
(collectively “Soccer Personnel”) of Major League Soccer, L.L.C., MLS
Canada LP, and the Major League Soccer (“MLS”) Team or Teams (and
such MLS Team Operators) for which [the player] ha[s] agreed (or may
agree) to play while this authorization is in effect, (and, in the event of
any contemplated assignment of my playing services to another MLS
Team or Teams, the Soccer Personnel of such other MLS Team or
Teams (and such MLS Team Operators); (b) at the direction of MLS and
consistent with the collective bargaining agreement, to the Soccer
Personnel of the United States Soccer Federation, the Canadian Soccer
Association, and any other National Federation (and their respective
Teams) for which [the player] ha[s] agreed (or may agree) agree [sic] to
play while this authorization is in effect; and (c) at the direction of MLS,
any individual or entity from which MLS or an MLS Team may receive
services in furtherance of uses and disclosure of [the player’s] Health
Information permitted by this authorization, such as electronic medical
records vendors and worker’s [sic] compensation insurance carriers,
provided that such individual or entity shall be required to maintain the
confidentiality of my Health Information.
307
These disclosure policies are similar to the practices of NFL clubs.
5. Sponsorship Arrangements
Research has not revealed an MLS medical sponsorship policy. However, some MLS clubs have entered
into sponsorship arrangements with healthcare providers and hospitals while at the same time retaining a
doctor from that healthcare provider as the club doctor. For example, the Hospital for Special Surgery in
New York is the “Official Hospital of the New York Red Bulls,”
308
and a doctor affiliated with the
Hospital for Special Surgery is listed as one of the Red Bulls’ two club doctors.
309
Similarly, Orlando
Health is both the jersey sponsor and “official medical team” of the Orlando City Soccer Club,
310
and a
doctor from Orlando Health serves as Orlando City’s club doctor.
311
In addition, the MLS Medical Manual tangentially admits that medical sponsorship is permitted. In
outlining policies concerning whether certain healthcare costs are the responsibility of the league or the
club, the MLS Medical Manual states that clubs are responsible for healthcare costs where “[c]lubs have
created either written or verbal marketing agreements in which clubs funnel billable therapy to a
particular club sponsor group.”
312
This provision thus strongly suggests that MLS permits sponsorship
arrangements whereby healthcare providers pay for the right to provide care. In contrast, the NFL does
not permit such arrangements.
G. Analysis
!
69!
Table 1-C below summarizes the leagues’ handling of certain issues concerning the different principles
identified at the beginning of this Chapter.
Table 1-C: Summary of Club Medical Personnel Policies and Practices
Do the Leagues’ Policies:
NFL
MLB
NBA
NHL
CFL
MLS
Quality of Medical Care
Require retention of doctors?
Yes
Yes
Yes
Yes
No
No
Require retention of athletic trainers?
Yes
Yes
Yes
Yes
Yes
No
Require sports-specific certification for
doctors?
Yes
No
Yes
Yes
No
No
Set forth a standard of care?
Yes
No
313
No
Yes
No
Yes
Disclosure and Player Autonomy
Require medical staff to disclose
communications with club to player?
Yes
No
No
No
No
No
Require club to pay for second opinion?
Yes
Yes
Yes
Yes
No
Yes
Provide club doctor right to determine a
player’s course of treatment?
No
No
Yes
Yes
No
Yes
Entitle players to surgeon of their choice?
Yes
No
314
No
Yes
No
No
Entitle players to medical records?
Yes
Yes
Yes
Yes
Yes
Yes
Require players to submit to physicals
upon request?
Yes
Yes
Yes
No
Yes
Yes
Confidentiality
Permit non-medical club personnel to
obtain and disclose player health
information?
No
Yes
Yes
Yes
No
Yes
Require players to inform club of care by
other medical professionals, regardless of
payment source?
No
If
basebal
l-
related
Yes
No
No
No
Conflicts of Interest
Insulate club medical staff from influence
by coaches and other club personnel?
No
No
No
No
No
No
Prohibit healthcare providers from paying
for right to provide care?
Yes
Yes
Partiall
y
Unkno
wn
No
No
Before analyzing the results of the above Table, it is important to note that some of the leagues’ practices
concerning these issues might be positive towards player health but are not codified in the CBA or other
policy document. Therefore we cannot capture them in our analysis, especially since some leagues were
unwilling to provide us information we requested. With that caveat in mind, we turn to our analysis of the
leagues’ policies concerning medical personnel. In particular, our focus is on how the NFL compares to
the other leagues.
The above Table suggests that the NFL’s policies concerning club medical personnel are the most
protective of player health in almost all cases by providing players with superior control and information
about their healthcare. The NHL’s policies are similarly protective of player health, with one worrisome
provision that permits club doctors to “determine the diagnosis and/or course of treatment,”
315
including
whether “a surgical procedure is the appropriate course of treatment for the Player.”
316
The NHL’s policy
would seemingly permit players to be compelled to undergo a surgery even if they (or their own doctor)
believe it inappropriate, at risk of having their contract voided should they refuse. That the NFL and NHL
!
70!
lead on these issues is perhaps not surprising considering they are generally the two leagues with the
highest rates of serious injuries (See Chapter 2: Injury Rates and Policies) and the most controversies
concerning player health. The CFL is a football league too of course, but it does not compare in size to the
NFL or NHL and thus does not engage in the same level of collective bargaining, policy making, or
litigation.
While overall the NFL appears to offer the medical personnel policies most protective of player health,
there are, however, four areas in which the NFL might learn lessons as compared to one or more of the
other leagues. We explain these areas below, including those resulting in recommendations for the NFL.
First, it appears the NFL might learn lessons when it comes to players’ access to medical records. The
NBA requires club medical personnel to provide players with medical records within 48 hours of a
player’s request. In contrast, the NFL CBA only entitles players to their medical records once during the
pre-season, once after the regular season, and upon request in the off-season.
317
However, in practice, the
NFL’s recently implemented electronic medical records system provides players with 24/7 access to their
medical records. Consequently, the NFL’s deviation on this issue is no longer relevant.
Similarly, the NHL CBA requires club medical personnel to provide players with a complete copy of their
medical records during their end-of-season physical. In contrast, while NFL players have 24/7 access to
electronic versions of their records, there is no NFL CBA provision that obligates clubs to provide players
with their medical records as a matter of course. It is not clear whether providing players with paper
copies of their medical records versus electronic access is preferable. It is possible that one approach – or
the two approaches combined – could increase the possibility that a player will review his records and
seek appropriate or necessary care. However, without additional information, it is speculative to say the
NHL’s policy is superior.
Second, the NHL CBA requires clubs to identify an individual responsible for monitoring the club’s
prescription drug use. The NFL CBA has no such requirement. Nevertheless, the absence of any such
provision is mitigated by the NFL’s policies concerning medications. NFL clubs do not store controlled
substances at their facilities and any prescription medications are filled through a local pharmacy.
Third, while the CFL Standard Player Contract requires players to submit to a pre-season physical by the
club’s doctors, the CFL CBA also requires that pre-season physicals “to determine the status of any pre-
existing condition” be performed by a neutral physician.
318
The stated purpose of this requirement is to
help determine “in the future” whether there was “an aggravation of… [a] pre-existing condition.”
319
Furthermore, the provision is housed within the Injury Grievance article of the CBA,
320
and thus it appears
that the provision is designed to ensure that there is an accurate record of a player’s injury history. In
contrast, NFL club doctors perform all pre-season physicals and would be the ones to opine about a
player’s prior injury history. We believe the CFL’s approach is preferred, for reasons explained below.
Fourth, the NHL’s and MLS’ required standards of care appear preferable to that of the NFL, in that they
seemingly require club doctors to subjugate their duties to the club to their duties to the player at all times.
In contrast, the NFL CBA only explicitly requires that the doctor’s first priority be the player when the
doctor is “providing medical care.” Club doctors have important roles for the club beyond providing
medical care, specifically performing fitness-for-play evaluations, the outcomes of which might not be in
the player’s interests. Consequently, by its specific terms, the NFL CBA only requires club doctors to
consider players as their principal responsibility some of the time. But while the NHL’s and MLS’
provisions are preferable in their specificity and demands, they still fail to sufficiently protect player
health.
321
!
71!
Despite the possible protections provided by the NHL’s and MLS’ standards of care, they do not – nor do
any of the other leagues – address perhaps the most fundamental structural issue concerning player health:
the conflicts of interest faced by club medical personnel. In each of the leagues, the club’s medical staff
treats the players, but is selected by, reports to the club, including providing advice on the players’ short-
term and long-term usefulness to the club. While the Canadian healthcare system seemingly insulates the
Canadian club doctors from payment as a source of conflict, American clubs have financial or other
arrangements with their club doctors that can influence doctors’ decision-making and care (consciously or
unconsciously). While the various player health provisions discussed herein can improve a player’s
options and empower him to receive better care, there will be concerns about the quality and primacy of
player health, and trust in club medical personnel, so long as it is principally clubs that control the
medical staff.
For these reasons, in our report Protecting and Promoting the Health of NFL Players: Legal and Ethical
Analysis and Recommendations, we recommended that club doctors and medical staff be redefined as
“Players’ Doctors” and “Players’ Medical Staff,” to reflect their exclusive responsibility to advance the
health of players.
322
Moreover, we recommended that these medical professionals should be chosen and
subject to review and termination by a Committee of medical experts selected equally by the NFL and the
NFLPA and that their only interaction with clubs should be via the head Players’ Doctor’s written reports
on the status of players currently receiving medical treatment. Finally, we recommend that a Players’
Doctor’s determination of a player’s playing status should be controlling. The rationale for this proposed
structure is discussed at length in our report but, generally, this arrangement removes the structural
conflicts of interest that can and do impede player health. The NHL’s standard of care supports our
proposed approach, but does not go far enough. To ensure the best possible and most independent care, a
standard of care is insufficient—structural changes are needed.
H. Recommendations
Given the general superiority of NFL policies compared to other leagues, and uncertainty about possible
areas where the NFL can learn by comparison, we have only one recommendation related to medical care,
generated by comparison to the CFL.
Recommendation 1-A: Pre-season physicals for the purpose of evaluating a player’s prior injuries
should be performed by neutral doctors.
The CFL requires pre-season physicals for the purpose of evaluating a player’s prior injuries to be
performed by a neutral doctor. The NFL should adopt the same rule. The use of neutral doctors ensures
that players’ medical history is being recorded in an accurate manner, i.e., in a manner that correctly
details a player’s injury history and the ways in which those prior injuries are manifesting themselves
today. Clubs—and thus club doctors—have an incentive to minimize players’ injuries and declare them
fit to play in order to avoid further financial liability. For example, if an NFL player is injured during one
season, and fails the pre-season physical the next season, the player is entitled to an Injury Protection
benefit, an amount equal to 50% of his Paragraph 5 Salary (i.e., base) for the season following the season
of injury, up to a maximum payment of $1,150,000 (in 2016).
323
If the player is still injured during the
next pre-season, he can obtain Extended Injury Protection, a benefit that permits a player to earn 50% of
his salary up to $500,000 for the second season after suffering an injury that prevented the player from
continuing to play. Additionally, similar to the CFL, if the club doctor finds that a player is healthy
enough to play, a player’s potential Injury Grievance
324
is undermined. In these situations, the club doctor,
acting in the interests of the club, might be motivated to find that the player is healthy enough to play
during the pre-season physical, preventing the player from receiving benefits and compensation to which
he is entitled. While we do not know if such practices are common or widespread, in our Report
Protecting and Promoting the Health of NFL Players: Legal and Ethical Analysis and Recommendations,

!
72!
we provided examples from players attesting that such situations do occur.
325
Whatever the frequency, a
structural conflict still exists and needs to be addressed. A neutral doctor avoids the potential for bias, and
ensures players are receiving their just compensation and care.
As discussed in the Introduction, the NFL declined to review this Report. However, MLB did provide
comments on the Report which may provide insight into the viewpoints of the other professional leagues.
In reviewing a draft of this Report, MLB expressed its disagreement with this recommendation, stating:
The recommendation (1-A) that preseason physical examinations be
performed by a neutral doctor misses the point of the PPE
[preparticipation physical evaluation]. Continuity of care is an important
aspect of player health care and it is the view of our medical experts that
having a separate physician for the preseason exam would result in worse
care during the season. The recent Consensus Monograph on PPE, which
was prepared by several national physician groups and is viewed as the
governing document on these types of exams, does not include a
recommendation for independent physicians.
While we generally agree with MLB that continuity of care is important, we disagree with MLB’s
comment for several reasons.
First, it is important to understand we believe there is a structural conflict of interest whereby NFL club
doctors provide care to players while also providing services for the club.
326
As a result, players have
business reasons to be concerned about the outcome of the pre-season physical. As explained above, club
doctors may not accurately record a player’s condition, which can negatively affect his contract status and
benefits to which he is entitled.
Second, our recommendation would not affect continuity of care as MLB’s comment seems to suggest.
Assuming doctors working for the club continue to treat players (which is not what we recommend as
explained in the footnote below), the club doctor would have full access to the results of the pre-season
physical and is also permitted to re-examine the player at any time, including during the pre-season.
However, a physical performed by a neutral doctor should be used to establish the player’s pre-existing
conditions in order to better protect the player’s business interests.
Third, MLB’s reference to the consensus monograph
327
is misplaced. The monograph specifically states
that it “is intended to provide a state-of-the-art, practical, and effective screening tool for physicians who
perform PPEs for athletes in middle school, high school, and college.”
328
Thus, the monograph does not
apply to professional sports, and does not speak to the issues raised above.
CHAPTER 2: INJURY RATES AND POLICIES
329
An important measurement of player health is the incidence and type of injuries players may sustain in
the course of their work. Additionally, given the importance of player injuries, the manner in which
player injuries are handled administratively and reported can indicate a league’s approach to player health
issues more generally. In this Chapter, we examine the leagues’: (1) injury tracking systems; (2) injury
rates; (3) injury-related lists; and, (4) policies concerning public reporting of injuries. At the conclusion of
this Chapter, Table 3-E will summarize some of the key statistics and policies concerning injuries.
Before beginning our analysis, we provide some background information and qualifications on some of
the topics we will discuss.
!
73!
Injury Tracking Systems and Rates
As will be discussed below, all of the leagues (except the CFL) have an electronic medical record
(“EMR”) system into which the club’s medical staff enters player injuries and through which the club and
league are then able to track player injuries and conduct a variety of statistical analyses, all on a de-
identified basis.
330
While these data are valuable, they are not routinely made available to the public.
Consequently, obtaining data on injury incidence, specifically in the form of injury incidence rates,
requires release of the data either by the leagues themselves or through academic studies (many of which
have requested the data from the leagues).
There are additional limitations with the injury tracking systems.
As a general matter, injuries in sports are underreported.
331
Players routinely hide their medical conditions
from the club. Players principally do this to protect their status on the club and due to fear of being
viewed as less tough by the coaches.
332
Players know that their careers are tenuous and also know that if
the club starts perceiving a player to be injury-prone, it is often not long before the club no longer
employs that player.
333
Similarly, club medical staff might not enter player injuries into the system or might discourage players
from seeking help for a medical condition so that it appears players are healthier than they actually are.
Medical staff also might not input injuries in order to: (1) make it appear they are doing their job well and
keeping players healthy; or, (2) to help the club in a potential dispute with the player. For example, if an
NFL club terminates a player’s contract while he is injured, the club is responsible for the player’s salary
for so long as the player is injured. A club’s medical staff might not include the full extent of a player’s
injuries in the system in order to support the club’s potential argument that the player was not injured
when the club terminated the player’s contract. While we do not mean to imply such actions are common,
and we have no way of estimating the incidence, in our report Protecting and Promoting the Health of
NFL Players: Legal and Ethical Analysis and Recommendations, we discuss evidence from interviews
with players who attest that such actions do occur in the NFL.
334
It is not known whether there is any
prescribed punishment in any of the leagues if a club’s medical staff fails to fully and accurately report
player injuries. Beyond non-reporting by club medical staff, some injuries might not be documented
because the athlete does not report the injury to the medical staff.
In particular, as other scholars have noted, concussions are underreported.
335
Diagnosing concussions
requires review of various criteria, such as whether the player has balance problems, a blank or vacant
look, disorientation, or cognitive issues.
336
Additionally, a concussion diagnosis often requires a player to
self-report symptoms, such as headaches, dizziness, vision problems, and/or sensitivity to light or
sound.
337
As a result of the varied diagnostic criteria and the ability of players to hide symptoms,
concussion rates are likely higher than the reported statistics.
In light of the above, we emphasize that the injury statistics we provide in this Chapter reflect only those
that are reported and that actual injury rates are likely higher. Aside from underreporting, our analysis is
also limited by differences between the leagues, including scheduling, EMR systems, and injury
definitions.
Injury severity is a potentially interesting statistic to calculate and compare. Indeed, several of the studies
discussed below attempt to quantify injury severity by the amount of time players lost, i.e., the number of
practices or games a player missed. However, because the leagues’ practice and game schedules vary
considerably, a cross-league comparison of the severity data would not be useful. For example, NFL clubs
play a 16-game regular season and practice four to five times per week. In contrast, MLB clubs play a
162-game regular season and have almost no practices during the season. An injury that might cause an
!
74!
MLB player to miss four or five games might not cause an NFL player to miss any games. Consequently,
determining the severity of injuries by the number of games or practices missed does not provide for an
accurate comparison across the leagues.
338
Finally, in this Chapter, unless otherwise indicated, we are only comparing data from regular season
games, not pre-season or post-season games or practices. We generally limit our analysis in this way
because in many cases only regular season injury data are available. Additionally, several other domains
we discuss such as the number of games, players, and plays, have more readily available and consistent
data in the regular season, permitting better comparisons. Lastly, the number of practices per season in
each of the sports varies considerably, making comparisons that include practices problematic. While this
method results in reporting lower aggregate injury incidence, we believe statistics focused on injuries per
regular season game, and injuries per player-season
339
provide the best understanding of the incidence of
injury in each sport.
Injury Studies
In this Chapter, we utilize data from several studies concerning injury rates in the respective leagues.
Several of these studies retrieved data from the leagues’ injury tracking system. Consequently, those
studies (and our use of that data) are limited in the same way that the injury tracking systems are limited,
as discussed above. In addition, we identify other limitations of the studies that are relevant to our
analysis. Despite these limitations, the studies we have used are the best publicly-available sources for
injury data in the leagues and, we believe, provide useful data. Nevertheless, in light of these limitations
and the limited number of studies, we caution the reader about interpreting our findings too strongly.
Indeed, one important recommendation we make is that more research is needed on injury rates in the
NFL, as well as more sharing of league data on injuries. Similarly, while our focus is on the NFL, it is
likely desirable for the other leagues to engage in the same type of research.
Concussions
Given the above concerns about underreporting of injuries, specifically concussions, it is also important to
know what we mean by “concussion.” The leading definition of a concussion comes from the 4th
International Conference on Concussion in Sport held in Zurich, Switzerland, in November 2012, and
published in the British Journal of Sports Medicine. The publication (identified by lead author Paul
McCrory of the Florey Institute of Neuroscience and Mental Health in Australia) is a consensus statement
from 28 of the leading sports medicine and sports concussion professionals, including many with ties to
the leagues and unions.
340
The consensus statement (which improves on definitions from prior
conferences) defines a concussion “as a complex pathophysiological process affecting the brain, induced
by biomechanical forces.”
341342
In addition, the consensus statement lists symptoms and conditions
associated with concussions, including headaches, cognitive impairment, behavioral and emotional
changes, loss of consciousness, amnesia, and sleep disturbance.
343
The NFL, MLB, NBA, NHL, and MLS
concussion protocols specifically cite the consensus statement’s criteria for a concussion as the required
procedure.
344
Given the nature of this Report, some may wonder why we are not providing analysis of each of the
leagues’ concussion protocols, that is, the policies that dictate how the clubs treat players who have
suffered or are suspected of having suffered a concussion. We have chosen not to discuss these policies in
depth because they are substantially similar. The consensus statement sets forth the leading medical
opinion as to the appropriate process for evaluating a possible concussion, including the diagnostic tests
to be performed (both pre-season and post-concussion), and a recommended return-to-play process,
consisting of a graduated increase in activity, provided the player remains free of concussion-
symptoms.
345
In reviewing the leagues’ concussion protocols (or reports describing the protocols where
!
75!
the protocols themselves were not available), it is clear that all of the leagues’ protocols are in line with
the procedures recommended by the consensus statement.
346347
We acknowledge that at times questions have been raised as to whether certain leagues or clubs are
sufficiently following the protocols.
348
While these are important questions, we were unable to find any
objective data from which to analyze the leagues’ compliance. This is an issue that the leagues and unions
must investigate and enforce.
349
Injury-Related Lists
In this Chapter, we also discuss injury-related lists—a type of roster on which injured players are placed
for a certain number of days or games. All of the leagues have such lists. The lists vary in their meaning
and duration, potentially alleviating or creating pressure on the player to play through, or return from, an
injury. We will discuss each league’s approach to injury lists and analyze their effects in the Analysis
Section.
***
With this background in hand we now turn to an analysis of each of the leagues on the relevant issues
relating to player injuries.
A. Injuries in the NFL
1. Injury Tracking System
In 1980, the NFL created the NFL Injury Surveillance System (“NFLISS”) to document, track, and
analyze NFL injuries and provide data for medical research.
350
When an injury occurs, each club’s athletic
trainer is responsible for opening an NFLISS injury form and recording the medical diagnosis (including
location, severity, and mechanism of injury) and details about the circumstances (e.g., date, game or
practice, field surface) in which it occurred.
351
Prior to 2015, a reportable injury was defined as only those
injuries, football-related or not, associated with any time lost from practice or games or specific
conditions regardless of time lost, including but not limited to concussions, fractures, dental injuries
requiring treatment, health-related illness requiring IV fluid administration, and injuries or illness
requiring special equipment (e.g., a knee brace). Beginning with the 2015 season, all injuries, regardless
of whether or not they result in time lost from practice or games, are included in the NFLISS.
352
The
athletic trainer is required to update the injury form with details about all medical treatments and
procedures the player receives, including surgery.
353
Since 2011, the NFLISS has been managed by the
international biopharmaceutical services firm Quintiles.
354
Quintiles analyzes injury data and provides
reports to the NFL and NFLPA throughout the year.
355
The NFLISS provides the best available data concerning player injuries and we thus use it here. Although
the NFL’s past injury reporting and data analysis have been publicly criticized as incomplete, biased, or
otherwise problematic, those criticisms have been in response to studies separate from the NFLISS
356
and
we are not aware of any criticism of the NFLISS.
357
The next Section is a compilation of NFLISS data on
player injuries, which was reviewed and updated (where necessary) by the NFL. However, in considering
this data, it is important to recognize that the NFL’s injury reporting systems have undergone substantial
change in recent years. An electronic version of the NFLISS was launched as a pilot with five clubs in
2011;
358
the electronic NFLISS expanded to all 32 clubs in 2012;
359
then, in 2013, the NFL launched an
electronic medical record (“EMR”) system on a pilot basis with eight NFL clubs, which was expanded to
all clubs in 2014.
360
The EMR system integrates with the NFLISS and provides the most accurate injury
reporting data in NFL history. Consequently, the different reporting structures over time almost certainly
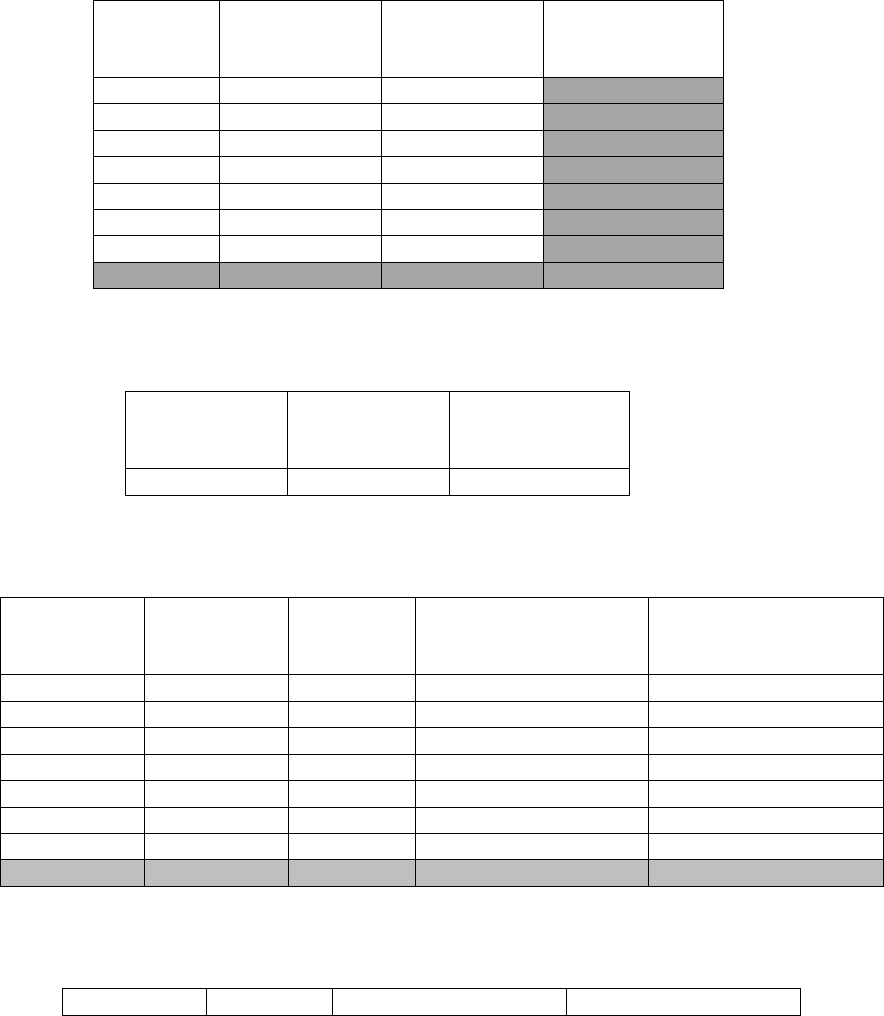
!
76!
contributed to fluctuations in the injury rates identified below. Therefore, it is not possible to be certain
whether injury rates have increased in recent years, or if, instead, the apparent increases are due to
improved injury reporting, or some combination of the two. Similarly, increased attention to player
injuries in recent years, concussions in particular, might also lead to higher reported injury totals.
2. Injury Statistics
The tables below summarize key injury statistics of NFL players.
Table 2-A: Number of Practice, Game, and Total Injuries in NFL Pre-season (2009–2015)
361
Year
Number of
Practice
Injuries
Number of
Game Injuries
Total Injuries
2009
551
360
911
2010
560
410
970
2011
641
399
1,040
2012
675
431
1,106
2013
688
416
1,104
2014
823
503
1,326
2015
780
498
1,278
Totals
3,138
2,016
7,735
Table 2-B: Mean Number of Practice, Game, and Total Injuries in NFL Pre-season per Year, over
6 Seasons (2009–2015)
362
Mean Number
of Practice
Injuries
Mean Number
of Game
Injuries
Mean Number
of Total Injuries
623.0
403.2
1026.8
Table 2-C: Number of Practice, Game, and Total Injuries, and Mean Number of Injuries per Game
in NFL Regular Season (2009–15)
363
Year
Number of
Practice
Injuries
Number of
Game
Injuries
Total Regular Season
Injuries
Mean Number of
Injuries per Regular
Season Game
2009
165
1,372
1,537
5.36
2010
176
1,346
1,522
5.25
2011
295
1,426
1,721
5.57
2012
262
1,380
1,642
5.39
2013
264
1,500
1,764
5.86
2014
401
1,823
2,224
7.12
2015
336
1,730
2,066
6.76
Totals
1,899
10,577
12,476
N/A
Table 2-D: Mean Number of Practice, Game, and Total Injuries per Year, and Mean Number of
Injuries per Game in NFL Regular season, over 6 seasons (2009–15)
Mean
Mean
Mean Number of
Mean Number of
!
77!
Number of
Practice
Injuries
Number of
Game
Injuries
Total Regular Season
Injuries
Injuries per Regular
Season Game
364
271.3
1,511.0
1,782.3
5.90
Table 2-E: Number of Practice, Game, and Total Concussions, and Mean Number of Concussions
per Game in NFL Regular Season (2009–16)
365
Year
Number of
Practice
Concussions
(Pre- and
Regular Season)
Number of
Pre-season
Game
Concussions
Number of
Regular
Season Game
Concussions
Total
Concussions
Mean Number
of Concussions
per Regular
Season Game
2009
25
40
159
224
0.62
2010
45
50
168
263
0.66
2011
37
48
167
252
0.65
2012
45
43
173
261
0.68
2013
43
38
148
229
0.58
2014
50
41
115
206
0.45
2015
38
54
183
272
0.71
2016
32
45
167
244
0.65
Totals
315
359
1,280
1,951
NA
Table 2-F: Mean Number of Practice, Game, and Total Concussions, and Mean Number of
Concussions per Game in NFL Regular Season, over 8 Seasons (2009–16)
366
Mean Number of
Practice
Concussions (Pre-
and Regular
Season)
Mean
Number of
Pre-season
Game
Concussions
Mean
Number of
Regular
Season Game
Concussions
Mean
Number of
Total
Concussions
Mean
Number of
Concussions
per Regular
Season Game
39.4
44.9
160.0
243.9
0.625
Table 2-G: Number of Regular Season Game Concussions per Player, and Mean Number of
Regular Season Game Concussions per Player per Season (2009–16)
367
Year
Number of Regular
Season Game
Concussions
Number of Regular
Season Players
Rate of Concussions
per Player-Season
2009
159
2,123
0.075
2010
168
2,187
0.077
2011
167
2,144
0.078
2012
173
2,183
0.079
2013
148
2,188
0.067
2014
115
2,202
0.052
2015
183
2,251
0.081
2016
167
2,274
0.073
Totals
1,280
17,552
0.073
!
78!
In considering the mean number of concussions per player-season, it is important to point out that the
number of players who played in a regular season NFL game includes both players who played all 16
games in a season and those who played only 1 game in a season. Thus, while there is a mean of 0.073
concussions per player per regular season, the mean is likely different for different subsets of players, i.e.,
depending on how many games a player played in that season.
Table 2-H: Concussion Incidence by Player Position in the Regular Season (2013)
Position
2013
Offensive Line
19
Running Back
15
Tight End
16
Quarterback
6
Wide Receiver
17
Offense Total
73 (49.3%)
Defensive Secondary
25
Defensive Line
12
Linebacker
11
Defense Total
48 (32.4%)
Special Teams Total
27 (18.2%)
Table 2-I: Mean Number of Injuries per Play, NFL Regular Season Games (2013)
Total Number
of Injuries
Total Number
of Plays
368
Mean Number of Injuries Per
Play
369
1,500
43,090
0.035 injuries/play
As shown in Table 2-I, the mean number of injuries per play in 2013 was 0.035, indicating that there was
an injury on 3.5% of all plays. Additionally, from the available information regarding the total number of
injuries, total number of players per game, games per year, and years of data, we can calculate the overall
rate of injury as 0.064 per player-game.
370
In other words for every particular game there is a mean of 5.90
injuries (0.064 injuries per player-game x 92 players per game). That equates to one injury for every 15.6
players in that game.
We can also determine the mean rate of how often concussions occur in a game. Between 2009 and 2016
there were a total of 1,280 regular season concussions. Using the available information regarding the total
number of concussions, total number of players per game, games per year, and years of data, we can
calculate the overall rate of concussion per player-game as 0.0068 concussions per player-game.
371
We can also determine the rate of injuries per player-season. During the 2009–15 seasons, there were a
total of 15,278 player-seasons played.
372
During this same time period there were a total of 10,577 game
injuries. This equates to an overall rate of 0.69 injuries per player-season (10,577/15,278). Some
readers—particularly players—may be surprised that this statistic is not higher. It is important to
remember that this statistic is the mean of all players who played in the NFL during these seasons,
including players who might have only played in one game. Additionally, the statistic does not include
injuries that occurred during pre-season practices or games or regular season practices. Thus, while
helpful, this statistic is an incomplete picture of the injuries suffered by NFL players during the course of
a season.
!
79!
Readers might be interested in the mean number of games a player plays before suffering an injury. We
calculated above that the rate of injuries per player-game was 0.064. Thus, we can calculate that players
play a mean of 15.6 games before suffering one injury (1/0.064). We can also calculate the mean number
of games a player plays before suffering a concussion. We calculated above that the rate of concussion
per player-game was 0.0068. Thus, we can calculate that players play a mean of 147.10 games before
suffering one concussion (1/0.0068). With 16 regular season games, players theoretically play a mean of
9.2 seasons before suffering a concussion. For context, although there is a debate about career lengths
generally, the mean career length for a drafted player is about 5 years.
373
Nevertheless, it is important to
remember that these are mean statistics and thus include players who play very little in the game or
players who play positions less likely to suffer injuries or concussions. Players with more game time and
players at certain positions are likely to suffer injuries and/or concussions at rates higher than those
provided here.
Finally, we can calculate what percentage of player injuries are concussions. Between 2009 and 2015,
there were a total of 10,577 regular season injuries (Table 2-C). During this same time period, there were
1,113 regular season concussions (Table 2-E). Thus, concussions represented 10.5 percent of all regular
season injuries (1,113/10,577).
Finally, below is some additional information from the NFLISS:
374
• The most common types of injuries during regular season practices in 2013 were hamstring
strains (46), groin adductor strains (10), high ankle sprains (6), and shoulder sprains (6).
• The five most common types of injuries during regular season games in 2013 were concussions
(147), hamstring strains (approximately 128
375
), medical collateral ligament (MCL) sprains
(approximately 76), high ankle sprains (approximately 58), and groin adductor strains
(approximately 47).
• The most common mechanisms of concussions during regular season games in 2013 were contact
with other helmets (49.0%), contact with the playing surface (16.3%), contact with another
player’s knee (10.2%), and contact with another player’s shoulder (7.5%).
3. Injury-Related Lists
Injured NFL players are placed on different lists depending on the expected duration of the injury and the
timing of the injury.
If a player fails the pre-season physical, i.e., the club doctor determines the player is not physically ready
to play football, and is unable to participate in training camp but is expected to be able to play later in the
season, the player can be placed on the Physically Unable to Perform (“PUP”) List. A player on the PUP
List cannot practice or play until after the sixth game of the regular season and does not count towards the
club’s 53-man Active/Inactive List during that time.
376
Players who are injured during the pre-season or regular season and are unable to return that season are
placed on Injured Reserve, which typically precludes them from practicing or playing further that season.
Players on Injured Reserve do not count towards the club’s 53-man Active/Inactive List. In 2012, the
NFL and NFLPA amended the rules to permit clubs to allow one player in any season to return from
Injured Reserve after a minimum of six weeks.
377
Finally, players who suffer short-term injuries are only given a different status on the day of the game.
NFL clubs have a 53-man Active/Inactive List.
378
This is the roster of players clubs have to choose from
each week. On the day of the game, the number of players who are permitted to play, i.e., the Active List,
is reduced to 46 players.
379
Thus, seven players are declared Inactive and cannot play on each game day.
!
80!
Generally, at least some of the seven players declared Inactive have been so declared due to injury (the
rest would be for skill reasons). A player is Inactive for that particular game, but can be Active for the
next game. In this way, the Inactive List serves as a short-term, non-durational injured list.
4. Injury Reporting Policies
The NFL’s “Personnel (Injury) Report Policy” (“Injury Reporting Policy”) requires each club to report
information on injured players to both the NFL and the media each game week (“Injury Report”).
380
The
stated purpose of this reporting is “to provide a full and complete rendering of player availability”
to all
parties involved, including the opposing team, the media, and the general public.
381
According to the NFL,
the policy is of “paramount importance in maintaining the integrity of the game,”
382
i.e., preventing
gambling on inside information concerning player injuries.
383
The Injury Report is a list of injured players, each injured player’s type or location of injury, and the
injured player’s status for the upcoming game. Each injury must be described “with a reasonable degree
of specificity,” e.g., ankle, ribs, hand. For a quarterback’s arm injury or a kicker’s or punter’s leg injury,
the description must designate left or right. No other injuries require the side of the injury to be disclosed.
Historically, the player’s status for the upcoming game was classified into four categories: “Out
(definitely will not play)”; “Doubtful (at least 75 percent chance will not play)”; “Questionable (50-50
chance will not play)”; and, “Probable (virtual certainty player will be available for normal duty)”.
384
In
2016, the NFL changed the classifications for player injuries by: (1) eliminating the “probable”
designation; (2) changing the definition of “questionable” to “uncertain as to whether the player will play
in the game”; (3) changing the definition of “doubtful” to “unlikely the player will participate”; and, (4)
only using the “out” designation two days before a game.
385
The Injury Report also indicates whether a
player had full, limited, or no participation in practice, whether due to injury or any other cause (e.g.,
team discipline, family matter, etc.).
For a typical Sunday game, clubs must issue an Injury Report after practice each Wednesday, Thursday,
and Friday of game week. If there are any additional injuries after the Friday deadline, the club must
report these injuries to the NFL, the club’s opponent, the televising network, and the local media on
Saturday and Sunday.
The Injury Reporting Policy dictates that all injury reports be “credible, accurate, and specific within the
guidelines of the policy.” In “unusual situations,” clubs are requested to contact the League’s public
relations office and, when in doubt, clubs should include a player in the Injury Report. Clubs and coaches
that violate the policy are subject to disciplinary action. If a question arises as to why a player did not
participate in a game, the club can be required to provide a written explanation to the NFL within 48
hours.
Despite the enforcement system and disciplinary action for abuse (typically fines of $5,000 to $25,000
386
),
many in the media along with coaches and players have questioned the Injury Report’s accuracy and
value. A 2007 USA Today analysis of two-and-a-half seasons of Injury Reports found a high variance in
the number of injuries reported by teams, with 527 reported by the Indianapolis Colts versus just 103 by
the Dallas Cowboys.
387
Interviews with coaches in that article as well as others suggested that the
different philosophies of coaches to report even minor injuries versus only major injuries accounted for
this variance.
388
In the same article, former Pittsburgh Steelers coach Bill Cowher was quoted as saying
that he deliberately changed the location of injuries (e.g., reporting hip instead of knee) to protect his
players from having their injuries targeted by opponents.
389
Baltimore Ravens head coach Jim Harbaugh,
after being fined for not listing an injured player in 2012, told the media that “[t]here’s no credence on the
injury report now…. It doesn’t mean anything. It has no value.”
390
In March 2014, two former players on
the New England Patriots stated that head coach Bill Belichick filed inaccurate and false injury reports.
391

!
81!
Many in the media have referred to the Injury Report as a “game” or “joke.”
392
Nevertheless, some
believed that the 2016 changes to the injury reporting policy allowed for even more gamesmanship.
393
Many clubs have policies prohibiting players from speaking to the media about injuries.
394
Finally, to facilitate the Injury Reporting Policy, clubs, request or require players to execute waivers
permitting broad disclosure and use of their medical information.
395
With this understanding of the NFL’s policies, we can now begin our comparison to the other leagues.
B. Injuries in MLB
1. Injury Tracking System
In 2010, MLB—with agreement and assistance from the MLBPA—launched a web-based electronic
medical record (“EMR”) system “designed to allow trainers to have more and better information at their
fingertips.”
396
The EMR system is linked to MLB’s electronic Baseball Information System (“eBIS”),
397
that clubs use to complete the Standard Form of Diagnosis for Disabled List applications,
398
which will be
discussed in more detail below. With the EMR system, clubs’ athletic trainers enter data on “all injuries,
illnesses, and preventative events”
399
—whether baseball-related or not.
400
In addition, the EMR system
provides MLB with robust data, which—once de-identified and centralized in MLB’s Health and Injury
Tracking System (“HITS”)—MLB can use to monitor, study, and analyze injuries in baseball.
401
“HITS
includes any injury or physical complaint sustained by a player that affects or limits participation in any
aspect of baseball-related activity (e.g., playing in a game, practice, warm up, conditioning, weight
training).”
402
2. Injury Statistics
MLB’s efforts to study injury data should serve as a model for other leagues. Since the creation of MLB’s
EMR and HITS systems, MLB has undertaken, in partnership with the Johns Hopkins University
Bloomberg School of Public Health, to conduct and publish comprehensive studies of injuries by major
and minor league baseball players for the purpose of amending policies and practices to better protect
player health.
403
As of the fall of 2016, doctors affiliated with MLB and their research partners have
published studies on overall injury trends,
404
hamstring injuries,
405
knee injuries,
406
hip and groin
injuries,
407
and traumatic brain injuries,
408
in major and minor league players. Moreover, additional studies
are forthcoming.
409
In 2016, the researchers discussed above published a study describing the implementation of the EMR
and HITS systems, which included aggregate MLB injury data, shown below in Table 2-J.
410
Importantly,
“[f]or research studies, injuries are operationally defined as those that are work-related, did not occur in
the off-season (i.e., occurred only [in] spring training, the regular season, or the postseason), were a
primary diagnosis, and resulted in at least 1 day out of play.”
411
In the Analysis Section at the end of this
Chapter, we explain how this definition varies slightly from injury data we provide from other leagues.
Table 2-J: Number of Injuries during Spring Training, the Regular Season, or Postseason over Five
Seasons (2010-14)
Year
2010
2011
2012
2013
2014
Total
Injuries
2,076
1,641
1,347
1,270
1,249
7,583

!
82!
Importantly, the number of injuries recorded in HITS is considerably more than the number of players
placed on the Disabled List (“DL”), as shown in Table 2-K.
Table 2-K: Number of Disabled List Designations over Five Seasons (2010–14)
412
Year
2010
2011
2012
2013
2014
Total
Designations
459
515
504
519
488
2,485
The DL is a roster designation for players “unable to render services because of a specific injury or
ailment.”
413
During the time players are on the DL, clubs are permitted to replace the player on the club’s
active roster. However, not all injured players are placed on the DL. DL designations only include injuries
that result in time loss.
414
Thus, DL data underrepresents the actual total number of injuries and for that
reason we do not use it here.
Between 2010 and 2014, there were 4,614 spring training games,
415
12,150 regular season games,
416
and
32 postseason games,
417
for a total of 16,941 games. We can thus estimate that there are 0.45 injuries per
game (7,583/16,941). It is important to note that injuries that would occur during practice are included in
the total number of injuries and thus the actual mean number of injuries per game is probably lower.
However, we think the number of injuries that occur during practice are minimal—players play 162
games in 183 days
418
and there are very limited practices during the season.
419
We can also calculate a rate of injuries per player-game. A 2015 study conducted by MLB’s Medical
Director Dr. Gary Green (“Green Study”)
420421
revealed that during the 2011 and 2012 seasons, players
played a total of 138,085 regular season games.
422
During this same time period, there were 2,988
injuries.
423
However, these statistics include spring training and postseason injuries. From the data above,
we know that 71.7% of all MLB games between 2010 and 2014 were regular season games
(12,150/16,941). If we assume that the rate of injuries is constant among spring training, regular season,
and postseason games,
424
we can estimate that between 2011 and 2012, there were 2,142 injuries in
regular season games (2,988 x 71.7%). We can thus estimate that the rate of injuries per player-game
during this time period is 0.016 (2,142/138,085) assuming players only suffer one injury per game.
Finally, we can calculate the rate of injuries per player-season. Approximately 1,337 players played in an
MLB regular season game in 2014.
425
During 2014, there were 1,249 injuries. Thus, the rate of injuries
per player during the 2014 regular season was 0.93 per player-season (1,249/1,337). There are two
important points concerning this statistic: (1) this statistic represents a per player per season statistic,
regardless of whether they played one game or all 162 games; and, (2) there is likely variation in injury
rates among the different positions on the field.
Between 2011 and 2014, the five most commonly injured body parts were upper leg (thigh) (724
injuries), shoulder/clavicle (672), hand/finger/thumb (501), elbow (430), and knee (410).
426
We turn now to the incidence of concussions in MLB. The Green Study focused on exactly this issue.
The Green Study reported that there were 41 concussions in MLB during the 2011 and 2012 seasons, but
only 36 occurred during games.
427
It is important to note that the Green Study acknowledged that the
possible underreporting of concussions was a limitation of its study.
428
Nevertheless, the Green Study
offers the most reliable data on MLB concussions and we thus use it here.
With 4,860 regular season MLB games occurring during these two seasons,
429
there is a mean of 0.007
concussions per game (36/4,860). From the available information regarding the total number of
!
83!
concussions, total number of players per game, games per year, and years of data, we can calculate the
overall rate of concussion as 0.00026 per player-game.
430
Finally, we can estimate the rate of concussions per player-season. As stated above, in 2014, 1,337
players played in an MLB regular season game. In the same year, players were placed on the DL due to a
concussion or concussion-like symptoms 21 times.
431
Thus, in 2014, the rate of concussion per player-
season was 0.016 (21/1,337).
The Green Study also examined the number of concussions by “athlete exposures,” or “AE.” The Green
Study based the number of AEs on the actual number of games played by players.
432
This methodology
resulted in 138,085 AEs over the two seasons. With 36 concussions occurring in the two seasons, that is
the equivalent of 0.26 concussions per every 1,000 AEs, or, put another way, players experienced 0.26
concussions for every 1,000 games played. The Green Study also found that catchers experience more
concussions than fielders,
433
and “struck by batted ball” is the most likely mechanism by which a player
sustains a concussion.
434
Readers might be interested in the mean number of games a player plays before suffering an injury. We
calculated above that the rate of injuries per player-game was 0.016. Thus, we can calculate that players
play a mean of 62.5 games before suffering one injury (1/0.016). We can also calculate the mean number
of games a player plays before suffering a concussion. We calculated above that the rate of concussion
per player-game was 0.00026. Thus, we can calculate that players play a mean of 3,846.15 games before
suffering one concussion (1/0.00026). With 162 regular season games, players theoretically play a mean
of 23.74 seasons before suffering a concussion. For context, the mean career length for a drafted player is
about 5.6 years.
435
Nevertheless, it is important to remember that these are mean statistics and thus
includes players who play very little in the game or players who play positions less likely to suffer
injuries or concussions. Players with a lot of play time and players at certain positions are likely to suffer
injuries and/or concussions at rates higher than those provided here.
Finally, we can calculate what percentage of player injuries are concussions. In 2014, there were 1,249
injuries and 22 instances in which players were placed on the DL due to a concussion or concussion-like
symptoms. Concussions thus represented 1.8% of all injuries (22/1,249).
3. Injury-Related Lists
MLB has three DLs: a 7-day DL, which is exclusively for players who have suffered “acute”
concussions;
436
a 10-day DL; and, a 60-day DL.
437
To place a player on one of the DLs, a club must
submit an application to MLB that includes the Standard Form of Diagnosis (appended to the MLB CBA)
and a separate document indicating the estimated time period of recovery.
438
The club doctor-prepared
Standard Form of Diagnosis provides MLB with information about the nature of the player’s injury
(including “Body Side,” “Part of Body Injured,” and “Body Part Detail”), the date of the injury, and the
club doctor’s diagnosis.
439
MLB may request “that a Club provide additional information in support of a
Disabled List placement before the application is approved[.]”
440
Once MLB has accepted a DL
application, the player covered by the application must remain inactive for at least the number of days
enumerated in the title of the DL to which he has been assigned.
441
4. Injury Reporting Policies
Unlike the NFL, MLB does not obligate clubs to report player injuries publicly. However, the CBA
permits clubs to disclose the following “about employment-related injuries: (a) the nature of a Player’s
injury, (b) the prognosis and the anticipated length of recovery from the injury, and (c) the treatment and
surgical procedures undertaken or anticipated in regard to the injury.”
442
Despite this permission, club
!
84!
doctors are “prohibited from making any public disclosure of a Player’s medical information absent a
separate, specific written authorization from the Player authorizing such public disclosure.”
443
Thus, club
officials, such as coaches or the general manager (and not the doctor), are most likely the ones to update
the media on player injuries.
As a matter of course, clubs effectively report injuries through roster transactions. An MLB club’s active
roster is limited to 25 players (except during September).
444
If a player is injured and placed on the DL,
his spot on the active roster will be filled by another player. Clubs publicly update their active rosters and
DL as needed. Thus, when a player is moved from the active roster to the DL, the club is indicating that
the player is injured.
C. Injuries in the NBA
1. Injury Tracking System
Since 2012, the NBA has employed an EMR system, called HealtheAthlete. Cerner Corporation, the
creator of HealtheAthlete, describes the “secure electronic platform” as “enhanc[ing] the standard of
medical record keeping for all NBA athletes.”
445
The system allows each player to have an integrated
record of their care, gives medical personnel easy access to these records, and improves the NBA’s ability
to track trends in player health and healthcare.
446
The EMR system also “allow[s] for authorized academic
researchers to access the data (on a de-identified basis) and conduct studies designed to improve player
health and broaden medical knowledge” (with the NBPA’s approval, which cannot be unreasonably
withheld).
447
The CBA specifically permits disclosures of player health information to be made via
“secure systems” with EMRs to the extent that medical disclosures are otherwise allowed by the CBA.
448
Prior to the EMR system, the National Basketball Athletic Trainers Association (“NBATA”), comprised
of all athletic trainers working for an NBA club, maintained a record of “all injuries and illnesses
sustained by NBA players.”
449
An injury or illness was considered reportable if it: (1) required physician
referral, prescription medication, or both; (2) resulted in a missed game or practice; or, (3) necessitated
emergency care.
450
Entries into the NBATA system were “completed by the team’s athletic trainer and
cosigned by the team physician.”
451
The reported data included pathology, time and place of injury or
onset of illness, activity, and the mechanism of injury.
452
The HealtheAthlete system collects the same
data formerly recorded by the athletic trainers.
453
In reviewing a draft of this Report, the NBA stated that
the HealtheAthlete system also provides additional unspecified information. Additionally, since 2014, the
NBA has worked with the international biopharmaceutical services firm Quintiles to analyze injury data
and provide reports to the NBA and NBPA.
454
2. Injury Statistics
The most recent comprehensive study on NBA injury rates was led by Dr. Mark C. Drakos and published
in Sports Health in 2010.
455
The study looked at injury data from the NBATA injury database for 17
seasons (1988–89 through 2004–05).
456
The Drakos study stated that it did not examine injury rates “for
practices and pre-season games” due to “unreliable reporting methods and lack of a standardized
protocol.”
457
Given the source of the data, “injuries” as defined in the study included those: (1) requiring
physician referral, prescription medication, or both; (2) resulting in missed games or practices; and, (3)
those requiring emergency care.
458
Additionally, the study only included injury data for injuries that
occurred during the NBA regular season.
459
The Drakos study acknowledged that it was limited by the fact that the injury data may be underreported
for a variety of reasons.
460
Additionally, the length of study complicates the analysis, as it seems likely
that over the 17 seasons knowledge about injuries and attitudes towards reporting injuries changed,
!
85!
resulting in changes in the data over time. Nevertheless, the Drakos study provides the most reliable
publicly-available data on NBA player injuries and we thus use it here.
Like the Green Study discussed above in MLB, the Drakos study examined injury rates through AEs,
defined as “1 athlete appearing in 1 game.”
461
During the time period studied, there were 6,287 injuries in
regular season games.
462
The study determined there was an injury rate of 19.1 per 1,000 AEs.
463
Using the data from the Drakos study, we can also calculate several other statistics. Over the 17 seasons,
there was a mean of 369.8 injuries per season (6,287/17). Also, during the time period studied, there were
38,268 regular season NBA games.
464
Thus, there were 0.16 injures per regular season NBA game
(6,287/38,268).
To determine additional statistics, we used data from basketball-reference.com for the 17 seasons covered
by the Drakos study. During these seasons, players made a total of 387,673 game appearances. Thus, the
injury rate per player-game was 0.016 (6,287/387,673). Additionally, during the seasons of the study,
there were a total of 7,115 player-seasons.
465
Using the Drakos study’s calculation of 6,287 injuries, we
can calculate that the injury rate per player-season was 0.88 (6,287/7,115). Again, there are two important
limitations to this statistic: (1) this statistic represents a per player-season statistic, regardless of whether
he played one game or all 82 games; and, (2) there is likely variation in injury rates among the different
positions on the court.
According to data in the Drakos study, the most commonly injured body parts during regular season
games were ankles (66.1 injuries per season), knee (29.5), femur (28.4), lumbar spine (28.3), and tibia
(25.4).
466
Ankle sprains (distinct from all ankle injuries) were the most common injury (62.7 per
season).
467
Concussions were among the least-reported injuries in the study. During the 17-year period, there were
only 53 reported concussions that occurred during games, which accounted for only 0.8% of total injuries
reported during games and contributed to only 0.4% of games missed.
468
With 38,268 games played
during the period, a diagnosed concussion occurred only once every 722.0 games, or a mean of 0.0014
per game. Over the length of the Drakos study, the rate of concussion was 0.00014 per player-game
(53/387,673). During the 2013–14 season, there were only nine reported concussions,
469
a mean of one
every 136.7 games, or 0.007 per game. Players made 25,618 game appearances during the 2013–14
season,
470
and therefore suffered a per player-game concussion rate of 0.00035 (9/25,618). Additionally,
during the 2013–14 season, 483 players played in the NBA. Thus, there were 0.019 concussions reported
per player-season (9/483).
Readers might be interested in the mean number of games a player plays before suffering an injury. We
calculated above that the rate of injuries per player-game was 0.016. Thus, we can calculate that players
play a mean of 62.50 games before suffering one injury (1/0.016). We can also calculate the mean number
of games a player plays before suffering a concussion. We calculated above that the rate of concussion
per player-game was 0.00035. Thus, we can calculate that players play a mean of 2,857.14 games before
suffering one concussion (1/0.00035). With 82 regular season games, players theoretically play a mean of
34.8 seasons before suffering a concussion. For context, the mean career length for a player is about 4.8
years.
471
Nevertheless, it is important to remember that this is a mean statistic and thus includes players
who play very little in the game. Players with more game time are likely to suffer concussions at rates
higher than those provided here.
Finally, as stated above, during the time period of the Drakos Study (1988–2005), concussions
represented only 0.8% of game injuries. Based on increased attention to concussions since 2005, it seems
likely that this proportion has increased. However, we do not have more recent injury data against which
!
86!
to compare recent concussion data.
472
For this reason, we also do not provide a Figure showing
concussions as a percentage of injuries, as we do for the NFL, MLB, and NHL.
3. Injury-Related Lists
NBA rosters are generally limited to 15 players, divided between an Active List and an Inactive List.
473
A
club typically has 12 or 13 players on its Active List, who are eligible to play in games, and then has 2 to
3 players on the Inactive List who cannot play.
474
While NBA clubs generally place their injured players
on the Inactive List, healthy players can also be on the Inactive List.
475
Thus, the NBA has no list specific
to injured players. Moreover, players are not required to be on the Inactive List for any specific period of
time. Consequently, like in the NFL, NBA clubs can declare players inactive for as little as one game at a
time.
4. Injury Reporting Policies
Like the NFL, the NBA obligates clubs to report player injuries publicly, including the nature of the
player’s injury.
476
The CBA authorizes each club to make public injury information relating to its players,
so long as the information relates solely to the reasons that a player is not rendering his services as a
player.
477
Further, a player or his immediate family (where appropriate) “shall have the right to approve
the terms and timing of any public release of medical information relating to any injuries or illnesses
suffered by that player that are potentially life- or career-threatening, or that do not arise from the player’s
participation in NBA games or practices.”
478
In practice, NBA clubs release injury reports prior to every game, describing a player’s status (out,
doubtful, questionable, probable) and the nature of the player’s injury, including the injured body part.
D. Injuries in the NHL
1. Injury Tracking System
The NHL’s injury tracking system is part of the Athlete Health Management System (“AHMS”). The
AHMS is the NHL’s “electronic health records system focusing on the diagnosis, treatment and
rehabilitation of injuries suffered by athletes in the course of athletic competition and training.”
479
The
AHMS “has an injury surveillance component,” which requires “NHL Athletic Team Trainers/Therapists
and Team Physicians [to] document[] all injuries using a standardised ‘injury/illness event’ (IIE) form for
each event causing a player to miss one or more games.”
480
“Medical staff [are] also instructed to create
an IIE for each event needing medical assessment and treatment, regardless of time loss.”
481
2. Injury Statistics
The most comprehensive study on NHL injury rates was led by Carly McKay and published in the British
Journal of Sports Medicine in 2014.
482
The study looked at injury data from the AHMS for six seasons
(2006–07 through 2011–12).
483
The McKay study acknowledged that it was limited by the potential underreporting of injuries,
484
as is a
common and complex occurrence in injury surveillance. Additionally, it acknowledged the possibility that
athletic trainers’ practices in reporting injuries vary among the clubs.
485
Nevertheless, the McKay study
provides the best available data on NHL player injuries and we thus use it here.
Like the MLB and NBA studies discussed above, the McKay study examined injury rates through AEs.
This study defined 1 AE as 1 player participating in 1 game.
486
During the time period studied, there were
!
87!
4,368 injuries during regular season games.
487
Thus, using this methodology, there was an injury rate of
15.58 injuries per 1,000 AEs.
However, the study also presented injury rates per hours of ice time, where exposure was measured in
terms of the number of hours on the ice. Using this methodology, the study determined that there were
49.4 injuries per 1,000 hours on the ice.
488
The study explained that the approximately threefold increase
in injury rate is due to the fact that no player (other than the goaltender) plays the entire 60-minute
game.
489
Using the data from the McKay study, we can also calculate several other statistics. During the time
period studied, there were 7,380 NHL regular season games.
490
Thus, there were 0.59 injuries per game
(4,368/7,380).
From the available information regarding the total number of injuries, total number of players per game,
games per year, and years of data, we can calculate the overall rate of injury per player-game as 0.015.
491
Additionally, during the seasons of the study, there were a total of 5,145 player-seasons.
492
With 4,386
injuries during this span, there was thus a mean of 0.85 injuries per player-season (4,386/5,145). Again,
there are two important limitations to this statistic: (1) this statistic represents a per player-season rate,
regardless of whether they played one game or all 82 games; and, (2) there is likely variation in injury
rates among the different positions on the ice.
The study found that the most common injuries were to the head (16.8%), thigh (14.0%), and knee
(13.0%).
493
Additionally, body checks were the most frequent cause of injury at 28.6%.
494
Turning to concussions in the NHL, there are two principal studies.
495
In an independent study led by Dr.
Richard A. Wennberg and published in the Canadian Journal of Neurological Sciences in 2008 examined
concussion as reported in the media for ten NHL seasons (1997–98 through 2007–08).
496
While media
reported concussion data is not the ideal data set, the NHL and NHLPA declined our requests for data on
the number of concussions suffered over the last ten years. The Wennberg study concluded that the
concussion incident rate during these seasons was 1.45 per 1,000 AEs, with an AE defined as one player
playing in one NHL game.
497
The Wennberg study reported that there was a total of 688 concussions over
the ten years studied,
498
which we can calculate equals a mean of 68.8 reported concussions per season, or
.058 per regular season game.
499
From data provided by the Wennberg study, we can calculate that player
exposures (i.e., games played) was a total of 477,240 games during the seasons studied.
500
Thus, the rate
of concussions per player-game is 0.0014 (0.688/477,240).
In 2011, the doctors in charge of the NHL/NHLPA Concussion Program
501
published their own study
concerning NHL concussion rates.
502
The NHL/NHLPA study examined concussions reported by club
doctors on standardized injury reporting forms for the seasons of 1997–98 through 2003–04.
503
The
NHL/NHLPA study reported a total of 559 concussions during the time period studied,
504
equaling a mean
of 79.9 concussions per season, or 0.068 per regular season game.
505
If we estimate that 38 players play
per game,
506
we can estimate that during the seasons analyzed by the NHL/NHLPA study, players played
a total of 313,158 games.
507
Thus, according to the data from the NHL/NHLPA study, the rate of
concussions per player-game is 0.0018 (559/313,158). The NHL/NHLPA study also calculated those
statistics as the equivalent of 1.8 concussions per 1,000 player-hours on the ice.
508
As awareness of concussions has grown, and reporting of concussions has likely improved, more recent
data concerning concussions are more useful. The NHL does not make its concussion data publicly
available like the NFL, but, nevertheless, it was reported that there were 78 concussions during the 2012–
13 regular season and 53 concussions during the 2013–14 regular season.
509
However, because of a work
stoppage, there were only 48 games during the 2012–13 regular season, rather than the normal 82. We can
!
88!
extrapolate that 78 concussions during 48 regular season games is the equivalent of 133 concussions
during a normal 82 game regular season.
510
53 concussions reportedly suffered during a full-length 2013–
14 regular season is considerably less (60.2%) than the 133 concussions during a hypothetical full-length
2012–13 regular season, which necessarily calls the data into question. Nevertheless, as stated earlier, the
NHL and NHLPA declined to provide more recent or reliable data on concussions and thus we rely on the
best available data.
There were a total of 1,950 regular season games in the 2012–13 and 2013–14 regular seasons.
511
With
131 concussions having occurred during these season, we can calculate that a concussion occurred once
every 14.9 regular season games,
512
equivalent to a rate of 0.067 per regular season game.
513
Again,
estimating that 38 players play per game, we can estimate that players played a total of 74,100 games
during the 2012–13 and 2013–14 seasons.
514
We can thus calculate that the rate of concussions per player-
game during those seasons was 0.0018 (131/93,480). This rate is slightly more than that from the
Wennberg study and matches the rate calculated using data from the NHL/NHLPA study.
We can also try to calculate the number of concussions per player-season. Using the extrapolated
concussion data for the 2012–13 season, we can estimate a hypothetical total of 186 concussions during
the 2012–13 and 2013–14 seasons. Using data from the McKay study, we can calculate that there during
the time period studied (2006–12), a mean of 857.3 players played each season.
515
If we assume that the
mean number of players played for the 2012–13 and 2013–14 seasons was the same as during the time
period of the McKay study, we can estimate that there are 0.108 concussions per player-season
(186/1,714.6).
516
Readers might be interested in the mean number of games a player plays before suffering an injury. We
calculated above that the rate of injuries per player-game was 0.016. Thus, we can calculate that players
play a mean of 62.5 games before suffering one injury (1/0.016). We can also calculate the mean number
of games a player plays before suffering a concussion. We calculated above that the rate of concussion
per player-game was 0.0018. Thus, we can calculate that players play a mean of 555.56 games before
suffering one concussion (1/0.0018). With 82 regular season games, players theoretically play a mean of
6.8 seasons before suffering a concussion. For context, the mean career length for a player is about 5.6
years.
517
Nevertheless, it is important to remember that this is a mean statistic and thus includes players
who play very little in the game. Players with more game time are likely to suffer concussions at rates
higher than those provided here.
Finally, by combining data from the different studies, we can estimate what percentage of player injuries
are concussions. The McKay study found that there was a mean of 728 injuries per season during the
2006–07 through 2011–12 regular seasons. Again in an effort to use the most recent data, there was an
estimated mean of 93.0 concussions per season during the 2012–13 and 2013–14 regular seasons,
assuming the 2012–13 season was normal length (186/2). Based on these statistics, we can estimate that
12.8% of regular season injuries are concussions (93/728).
518
3. Injury-Related Lists
Like the NFL, injured NHL players are placed on different lists depending on the expected duration of the
injury and the timing of the injury.
First, the Injured Reserve List (“IR”) is for a player “reasonably expected to be injured, ill or disabled and
unable to perform his duties as a hockey Player for a minimum of seven (7) days from the onset of such
injury, illness or disability.”
519
NHL club rosters are limited to 23 players.
520
During the time a player is
on IR, the club can replace him on the roster.
521
!
89!
Second, players who fail the pre-season physical are placed on the Injured Non-Roster list.
522
A player on
the Injured Non-Roster list does not count against the club’s 23-man roster.
523
NHL clubs are permitted to
have up to 50 players under contract,
524
thus, the purpose of the Injured Non-Roster list is unclear.
Third, like the NFL, players injured for only a short period of time are only temporarily declared inactive.
NHL clubs have 23-man rosters. But clubs are only permitted to have 20 players play in each game. Thus,
clubs declare three players inactive for each game. As in the NFL, the players declared inactive are
frequently players with an injury that is expected to keep them out of only for a game or two.
4. Injury Reporting Policies
Like the NFL, the NHL requires clubs to report publicly information about player injuries. Specifically,
clubs are “required to disclose that a player is expected to miss a game due to injury, or will not return to
a game following an injury.”
525
Additionally, “Clubs are prohibited from providing untruthful information
about the nature of a player injury or otherwise misrepresenting a player’s condition.”
526
The CBA authorizes clubs to publicly disclose the nature of a player’s injury, the prognosis and
anticipated recovery time, and the treatment and surgical procedures that have been or will be
undertaken.
527528
Nevertheless, unlike in the NFL, clubs are not required “to disclose the specific nature of
player injuries.”
529
Accordingly, individual clubs may disclose information as they see fit, and
designations such as “upper-body injury” and “lower-body injury” are both common and acceptable.
530
The NHL may fine clubs for failing to abide by the policy, but the NHL does not publicly disclose those
fines.
531
E. Injuries in the CFL
1. Injury Tracking System
Research has not revealed any injury tracking system in use by the CFL.
2. Injury Statistics
There has not been a comprehensive study of general injury rates in the CFL, perhaps because CFL clubs
are not required to publicly report injuries, as will be discussed below.
532
In 2010, the CFL implemented a concussion protocol, requiring the standardization of concussion
reporting and allowing the League to more accurately track concussions.
533
In the first year of the new
protocol, there were 50 reported concussions in 85 CFL games for a mean of 0.59 per game.
534
It is
unclear whether this data includes pre-season or postseason games.
535
The CFL does not publicize its concussion data in the same manner as the NFL. Thus, it is challenging to
find more recent statistics concerning the number of concussions in the CFL. However, in a 2015 news
article, Dr. Dhiren Naidu, the club doctor for the CFL’s Edmonton club, stated that in 2014, there was a
mean of slightly more than eight concussions per club.
536
With nine CFL clubs, that means there were
slightly more than 72 concussions in the CFL in 2014. In the same article, it was reported that
concussions in the CFL “dropped by 25 percent in 2015.”
537
Thus, if we assume that the number of
concussions in 2014 was 76 (which is closer to eight per club than nine per club), a 25% reduction would
mean that there were 57 concussions in 2015. Thus, in 2015, there was an estimated mean of 0.704
concussions per game.
538
!
90!
Using this estimated number of concussions in 2015, total number of players per game, and games per
year, we can calculate a rate of 0.0080 concussions per player-game.
539
With this statistic we can also
calculate that the mean number of games a player plays before suffering one concussion is 125.0
(1/0.0080). With 18 regular season games, players theoretically play a mean of 6.9 seasons before
suffering a concussion. Nevertheless, it is important to remember that this is a mean statistic and thus
includes players who play very little in the game or players who play positions less likely to suffer
concussions. Players who play a lot and players at certain positions are likely to suffer concussions at
rates higher than those provided here.
3. Injury-Related Lists
CFL clubs maintain a 44-player active roster, a two-player reserve list,
540
and a 10-player practice-squad
roster.
541
In the event that a player is injured, his club may place him on either a six-game or one-game
Injured List, depending on the severity of the injury.
542
Players on either Injured List do not count toward
the club’s roster limits.
543
4. Injury Reporting Policies
The CFL does not require public disclosure of injuries, but clubs report injuries to the CFL through the
process of placing a player on the Injured List, and clubs must report concussions to the League.
544
F. Injuries in MLS
1. Injury Tracking System
Like the NBA, MLS uses the “HealtheAthlete” EMR system for recording player medical information
and tracking injuries.
545
Cerner Corporation, the creator of HealtheAthlete, describes the “secure
electronic platform” as providing the ability to “improve the standard of medical record keeping for
injured athletes, as well as ease communication between the athlete’s key care providers.”
546
Additionally,
according to Cerner, the platform “allows MLS athletic trainers to increase the accuracy of injury
documentation by accessing the platform from any location and integrating care-related media, like notes,
X-rays, and MRIs, directly into the athlete’s injury report.”
547
Athletic trainers are required to “document
soccer related Player complaints, injuries, treatments, [and] medications, including over-the-counter
medications[.]”
548
2. Injury Statistics
The only study ever done of MLS injury rates was performed by San Jose Earthquakes athletic trainer
Bruce E. Morgan following MLS’ inaugural 1996 season.
549
The study determined that MLS players
suffered injuries at a rate of 35.3 per 1,000 hours of game play.
550
Data from the MLS’ HealtheAthlete system are not publicly available and thus it is difficult to provide
current MLS injury data. More helpful data can be derived from studies or reports concerning injury rates
in the Union of European Football Associations (“UEFA”), a European soccer organization whose
members generally include the best soccer clubs in the world and who play in some of the best soccer
leagues in the world (such as the English Premier League and Spain’s La Liga). While UEFA and MLS
are different soccer organizations, we nonetheless believe that data from UEFA, an elite soccer
organization like MLS, can be instructive of the injury rates in MLS. Indeed unless and until MLS makes
its own data public, we think the UEFA data provides the best proxy estimate of the underlying injury rate
in that league.
!
91!
In 2014, UEFA released a report on injuries suffered by players playing for a selection of 29 (out of 54)
UEFA member clubs (“UEFA Report”).
551
The UEFA Report does not provide a definition for a
reportable injury. Nevertheless, the UEFA Report stated that the mean match injury incidence for all
clubs was 23.2 injuries per 1,000 hours of match play during the 2013–14 season.
552
Additionally, a study
done of UEFA injuries from 2001 to 2008 determined that players suffered injuries at a rate of 27.5 per
1,000 hours of game play.
553
The UEFA Report acknowledges two relevant limitations. First, it acknowledged that the Report only
includes injuries from one season.
554
Second, the UEFA Report acknowledged that there is variation
among the clubs in injury incidence,
555
which might be explained by different practices in the reporting of
injuries. For example, the UEFA Report does not discuss a standardized injury reporting system or
process among the clubs. Nevertheless, the UEFA Report provides the most reliable data on UEFA player
injuries and we thus use it here.
The UEFA Report determined that the body parts most commonly injured during games are thigh
(27.0%), knee (17.5%), ankle (14.6%), hip/groin (13.8%), and lower leg/Achilles tendon (7.6%).
556
Using the data from the UEFA Report, we can also calculate several other statistics. The UEFA Report
included data from 29 clubs.
557
Additionally, the UEFA Report found there to be a total of 739 injuries
from games,
558
for a mean of 25.5 injuries per club for the 2013–14 season (739/29).
The UEFA report also reported that the clubs participating in the study played a mean of 59 games,
559
for
a total of 1,711 games played by the clubs (59 x 29). To provide an accurate analysis of the injuries per
game, we can only count games in which the clubs played against one another as one game, i.e., we only
count the unique games. We thus reviewed the 2013–14 seasons of the 29 clubs (which participate in 12
different leagues) and determined that the clubs played 327 games against one another. Thus, the clubs
played in a total of 1,384 unique games (1,711 less 327). With this number of games, we can calculate
that there were 0.53 injuries per UEFA game (739/1,384).
We can also calculate injury rates per player. Data on player participation during the 2013–14 season was
not readily available. Thus, we make our best estimates. There are generally 11 players per club in a
soccer game at a time. FIFA’s
560
rules limit clubs to three substitutions in official games.
561
Thus, we can
estimate that 14 players play in each game per club, assuming clubs use all of their substitutions. As a
result, we can estimate that were 19,376 player appearances during 2013–14 games (14 x 1,384). We can
then estimate a rate of 0.038 injuries per player-game (739/19,376). We again remind the reader there is
likely variation among the different positions on the field.
The UEFA Report found that the most common injuries were to the thigh (27.1%), knee (18.5%), and
hip/groin (14.5%).
562
The UEFA Report reported 14 concussions during games.
563
Using the above statistic of 1,384 unique
games, we can calculate a mean of 0.010 concussions per game (14/1,384). With an estimated 19,376
player appearances, we can thus also estimate that the rate of concussion per player-game was 0.00072
(14/19,376).
Readers might be interested in the mean number of games a player plays before suffering an injury. We
calculated above that the rate of injuries per player-game was 0.038. Thus, we can calculate that players
play a mean of 26.32 games before suffering one injury (1/0.038). We can also calculate the mean number
of games a player plays before suffering a concussion. We calculated above that the rate of concussion
per player-game was 0.00072. Thus, we can calculate that players play a mean of 1,388.89 games before
suffering one concussion (1/0.00072). Nevertheless, it is important to remember that this is a mean
!
92!
statistic and thus includes players who play very little in the game. Players who play a lot are likely to
suffer concussions at rates higher than those provided here.
Finally, we can calculate what percentage of injuries were concussions. The UEFA report found that 14 of
739 injuries were concussions, equal to 1.9%.
MLS, without explanation, has refused to publicly release data on the number of concussions suffered by
its players.
564
3. Injury-Related Lists
MLS club rosters are limited to 28 players.
565
Injured players can be placed on two different lists,
depending on the severity of the injury.
First, players with “short-term” injuries are placed on the Disabled List (“DL”) and replaced on the roster
with another player.
566
The player must remain on the DL for a minimum of six matches.
567
Second, players who have suffered season-ending injuries are placed on the Season Ending Injury List.
568
These players are then replaced on the club’s roster.
569
4. Injury Reporting Policies
Like NFL clubs, MLS clubs are required to submit injury reports about players’ statuses.
570
MLS requires
clubs to include in their “Match Notes” information about player injuries.
571
Match Notes are programs of
pre-game information including rosters, statistics, and other information about the game that are publicly
available. In the Match Notes, the clubs must designate a player either as “out” or “questionable,” indicate
the affected part of the body, and provide an injury diagnosis.
572
According to the MLS Medical Manual,
the “injury reports should be as accurate as possible.”
573
Policies concerning the public reporting of injuries can seem somewhat contradictory. The CBA dictates
that public reporting of player injuries be limited to medical information relating to why the player “ha[s]
not been, [is] not, or may not be rendering playing services as an MLS player.”
574
However, the MLS
Medical Manual directs that “[i]n circumstances where a player injury or illness requires a complex
medical examination (e.g., to review a surgical procedure),” the club doctor or athletic trainer can
publicly describe “the nature of the injury or illness, the prescribed treatment or rehabilitation, and the
excepted timing of the player’s return to action.”
575
While the MLS Manual does say the club doctor or
athletic trainer should first consult with the player,
576
there is no indication the player can prevent the club
doctor or athletic trainer from discussing his medical condition.
G. Analysis
Tables 2-L and 2-M summarize some of the key injury-related statistics and policies. Nevertheless, it is
important to understand the limitations of the injury statistics. At the beginning of this Chapter, we
identified various limitations with analyzing injury statistics, including that injuries in sports are likely
underreported and that there are important differences between the leagues including practice and game
scheduling, EMR systems, and injury definitions. Moreover, for each of the leagues, we described various
limitations or statistical assumptions we made to calculate the statistics discussed in these tables.
Additionally, for the reasons discussed above, the injury statistics for MLS include MLS-specific data as
well as the data provided by the UEFA Report.
Table 2-L: Comparison of Leagues’ Regular Season Injury Statistics
577
!
93!
NFL
MLB
NBA
NHL
CFL
578
UEFA
MLS
579
Electronic
Tracking
System
Yes
Yes
Yes
Yes
No
N/A
580
Yes
Mean Injuries
Per Season
581
1,511.0
1,516.6
369.8
728.0
N/A
N/A
N/A
Rate of
Injuries Per
Player-Season
0.69
0.93
0.88
0.85
N/A
N/A
582
N/A
Mean
Concussions
Per Season
583
160.0
18.0
9.0
93.0
57.0
584
N/A
585
N/A
586
Rate of
Concussions
Per Player-
Season
0.073
0.016
0.019
0.108
N/A
587
N/A
588
N/A
Concussions
As Percentage
of Injuries
589
10.5%
1.8%
2.4%
12.8%
N/A
1.9%
N/A
Mean Injuries
Per Game
5.90
0.45
0.16
0.59
N/A
0.53
N/A
Rate of Injury
Per Player-
Game
0.064
0.016
0.016
0.016
N/A
0.038
N/A
Regular
Season Games
Per Player-
Injury
15.60
62.50
62.50
62.50
N/A
N/A
N/A
Most Common
Injury/Injured
Body Part
590
Concussio
n
Upper leg
(thigh)
Ankle
Sprain
Head
N/A
Thigh
N/A
Concussions
Per Game
0.625
0.007
0.007
0.067
0.704
0.010
N/A
Rate of
Concussion
Per Player-
Game
591
0.00679
0.00026
0.00035
0.00180
0.00800
0.00072
N/A
Games Per
Concussion
Per Player
147.10
3,846.15
2,857.14
555.56
125.00
1,388.89
N/A
Table 2-M: Comparison of Leagues’ Injury Reporting Policies
NFL
MLB
NBA
NHL
CFL
UEFA
MLS
Authorized to
Disclose
Injuries
(Existence
and Nature)
By waiver
Yes
Yes
Yes
No
N/A
Yes
!
94!
Required to
Disclose
Existence of
Injuries
Yes
No
Yes
Yes
No
N/A
Yes
Required to
Disclose
Nature of
Injuries
Yes
No
Yes
592
No
No
N/A
Yes
Before proceeding with our analysis, there are some important limitations to our comparison of injury
statistics across the leagues that should be noted.
First, in describing the leagues’ injury statistics, we are limited by the injury definitions used by the
leagues and studies. These definitions vary slightly among the leagues. Generally speaking, the NFL,
NBA, and NHL report all player injuries that result in treatment, regardless of whether the injury causes
the player to miss a practice or game. In contrast, MLB’s publicly available injury data (through the
research studies conducted by its partners and affiliates), only includes injuries that cause a player to miss
“at least 1 day… of play.” Thus, MLB’s injury data is low as compared to the other leagues.
Second, the data comes from different time periods. Generally speaking, the injury data for the NFL is
from 2009–16, for MLB from 2010–14, for the NBA from 1988–2005, and the NHL from 2006–12. It is
possible that injury rates and injury reporting practices have changed over time. Nevertheless, we believe
that this is still sufficiently reliable and transferrable to the present and thus provides useful information
for examining the injury rates across the different sports leagues.
With these limitations in mind, we turn now to an analysis of the data.
The NFL’s injury rates appear to be much higher than those of the other leagues. Indeed, if one combines
the estimated mean number of injuries suffered per game in MLB, the NBA, and the NHL, the estimated
mean number of injuries suffered per game in the NFL is approximately 4.9 times higher than the sum of
those other leagues. Additionally, if one combines the per-game concussion rates of all of the non-football
leagues (including UEFA), the NFL’s concussion rate is approximately 6.9 times higher than the sum of
those other leagues.
Nevertheless, it is important to point out one area in which the NFL may not be more injurious. The
NFL’s rate of concussions per player-season is 0.073; the NHL’s is 0.108. Thus, if one were to imagine a
comparison of one NFL player and one NHL player, the NHL player would be more likely to suffer a
concussion in his next regular season than the NFL player during his next season. However, this
discrepancy is due to the fact that the NHL plays substantially more regular season games than the NFL
(82 versus 16). When comparing concussion statistics on a per game basis, an NFL player is
approximately 3.8 times more likely to suffer a concussion in a regular season game as compared to an
NHL player (0.00679/0.00180).
In addition, limiting our analysis to the leagues’ regular season games (a function of available data)
underestimates injury rates. As shown in Section II.A on NFL injury rates, there are a significant number
of injuries and concussions sustained during NFL practices and during the pre-season (90 concussions in
2015 practices and pre-season games). In particular, pre-season NFL training camps can often be
extremely physical as players fight to prove themselves and make the club.
593
With that increased level of
intensity and physicality comes injuries and concussions. The reader should bear this limitation in mind.
!
95!
It is beyond our expertise to recommend specific on-the-field rule changes for professional football, but
we acknowledge that the rules of play can have an important impact on minimizing player injury. Rule
changes have historically been implemented to increase the safety of the game, and that trend continues
today.
594
However, the effects of these changes are not always clear at the outset: some injury-reducing
rule changes may inadvertently induce other types of risk-taking behavior, or reduce certain injuries while
exacerbating others. As in any contact sport, a certain number of injuries in football are unavoidable.
Which on-the-field changes would be desirable depends on a multi-factorial analysis of the benefits and
drawbacks of the current version of the game (in regards to health and otherwise), the benefits and
drawbacks of moving to a radically different game, and a method of weighing those benefits and
drawbacks against the welfare consequences of injuries to players and players’ own desires and goals as
they define them. Thus, while we welcome recommendations for rule changes to improve player safety
made by appropriate experts, evaluated in light of what players themselves want, we are not in a position
to make these determinations as a definitive matter. Ultimately, we conclude that we are likely to be far
more effective in protecting and promoting player health via off-the-field intervention than by suggesting
that the game itself fundamentally change.
In our efforts to improve and promote player health, we instead focus our analysis on three of the issues
discussed above: (1) injury tracking systems; (2) injury-related lists; and, (3) policies concerning public
reporting of injuries.
Injury Tracking Systems
Each of the Big Four leagues and MLS has an injury tracking system of some kind. Discussions with
experts on this issue indicated that the injury tracking systems are generally comparable; each of them is a
sophisticated and modern system that should enable accurate reporting and provide interesting and useful
data. The differences may come in how the leagues use the data that is available to them.
The NFL and NBA employ Quintiles, a health information technology firm, to perform sophisticated data
analysis concerning player injuries. While the studies discussed above demonstrate that the other leagues
have occasionally made injury data available for analysis, our research has not revealed whether the other
leagues perform an ongoing annual analysis like Quintiles does for the NFL and NBA. The academic
studies discussed above demonstrate that such analyses are possible. We will discuss this issue and others
in the Recommendations Section below.
Injury-Related Lists
The NFL, NBA, and NHL all permit their clubs to declare players inactive one game at a time,
595
which is
generally advantageous to players. We use the NFL as an example. In the NFL, clubs have a 53-man
Active/Inactive List, only 46 of whom can be active for the game each week. The remaining seven
players are placed on the Inactive List for the game, i.e., benched, either for injury or skill purposes, but
are available to play in the next week’s game. This arrangement permits players the opportunity to remain
on the roster but to rest and treat an injury without immediately rushing back to play. At the same time,
because clubs are constantly struggling with having the best players available as well as likely having
multiple injured players, players will still likely feel pressure to return as soon as possible so that the club
can deactivate other injured players and avoid seeking a replacement.
The Active/Inactive List is also interrelated with the Injured Reserve list, designated for players with
longer-term injuries. Generally, once a player is on Injured Reserve, he is no longer eligible to play that
season. However, by placing the player on Injured Reserve, the club can replace the player on the 53-man
Active/Inactive List. Thus, there are important implications in determining whether the player’s injury is
short-term and the club only has to declare him inactive for a game or two, or whether the player’s injury
!
96!
is more severe and requires the player to be placed on Injured Reserve (which also allows the club to
obtain a replacement player to join the 53-man roster).
The interplay between the short-term Inactive List and the longer term Injured Reserve list is particularly
important concerning concussions. As discussed in the full Report, concussions present uncertain
recovery times, are challenging to diagnose and treat, and present particularly acute long-term concerns.
MLB is the only sport with a concussion-specific injured list. We discuss this in more detail in the
Recommendations Section.
Injury Reporting Policies
There are three variations in the leagues’ injury reporting policies.
First, the NFL, NBA, NHL, and MLS require clubs to disclose publicly players’ injury statuses.
Second, the NFL, NBA and MLS require clubs to disclose publicly the nature of player injuries. While
the NHL requires clubs to disclose whether a player will miss a game or not return to a game due to
injury, the NFL and NBA (in practice) require that the club identify the player’s body part that is injured.
Below, we make a recommendation concerning this issue.
Third, in MLB, the NBA, the NHL, and MLS, the CBAs specifically describe what type of information
the clubs are permitted to disclose publicly. The NFL CBA is silent on this issue. Instead, NFL clubs
seemingly rely on players’ individually executed waivers to obtain permission to disclose publicly player
health information.
In considering whether the NFL should make changes to its Injury Reporting Policy, it is important to
understand what the concerns might be with the current Policy. We discuss two possibilities.
First, there is a general concern about an individual’s medical information being made publicly available.
Codes of ethics
596
and laws
597
relevant to the medical profession generally prohibit the disclosure of an
individual’s medical information to a third party without permission. These codes and laws are grounded
in the historical notion that an individual’s health information is “sacred.”
598
However, the relevant codes
of ethics and laws also permit an individual’s medical information to be disclosed to a third party without
permission in certain contexts, including where the employer is providing healthcare to an employee,
599
as
is the case in the NFL. These laws recognize that in certain situations employers have a legitimate interest
in an employee’s medical information, such as where the employee’s medical information pertains to the
employee’s ability to perform the job or for workers’ compensation purposes.
600
Nevertheless, disclosure to employers is different from disclosure to the general public. The question is
then whether the public or the NFL has sufficient interest in a player’s medical information to override a
player’s right to keep his medical information confidential. The reasons the NFL favors disclosure are
also relevant to our second concern with the NFL’s Injury Reporting Policy.
The second concern with publicly disclosing player health information relates to the potential for
targeting injuries. The NFL’s Injury Reporting Policy requires clubs to disclose the location of a player’s
injury. This disclosure creates the possibility that opposing players will target the location of a player’s
injury in an attempt to knock the player out of the game. For example, prior to the 2015 Super Bowl, New
England Patriots cornerback Brandon Browner said he would encourage his teammates to target and try to
hit the injured shoulder of Seattle Seahawks safety Earl Thomas and the injured elbow of Seahawks
cornerback Richard Sherman.
601
Similarly, in the 2012 NFC Championship game, New York Giants
special teams players Jacquian Williams and Devin Thomas discussed targeting San Francisco 49ers kick
!
97!
returner Kyle Williams due to his history of concussions.
602
We discuss this concern further in the
Recommendation Section.
The purpose for the NFL’s Injury Reporting Policy, including the requirement that the nature of a player’s
injury be disclosed, largely relates to gambling. The NFL’s Injury Reporting Policy was created
specifically for the purpose of preventing gamblers from having inside information about player
injuries.
603
More specifically, the NFL is concerned with how the importance of inside information might
affect the integrity of its games. Gamblers will seek inside information, including player injury
information, and there is no better source for player injury information than the players themselves. Inside
information about player injuries can lead to closer relationships between gamblers and players, leading
to concern that gamblers might cause players (through pay or intimidation) to alter their play, diminish
their effort, or intentionally try to lose to benefit the gamblers.
604
If that is the case, the legitimacy of the
games is undermined and, if exposed, public confidence and interest in the games would likely erode.
605
Consequently, the NFL prohibits players from having any association with gamblers or gambling
institutions.
606
The NFL’s stance on gambling was established in the 1960s when gambling was closely associated with
organized crime.
607
And the NFL’s concerns were well-founded. Among other incidents, in 1963, two of
the leagues’ best players, Alex Karras of the Detroit Lions and Paul Hornung of the Green Bay Packers
were suspended one year for betting on NFL games and associating with known criminals.
608
All that said, it is debatable whether the NFL’s gambling-related concerns are sufficiently substantial
today to justify overriding a player’s right to have his health information treated confidentially. These
questions are beyond the scope of this report. In particular, it would be important to consider federal law
enforcement’s opinions on the state of organized crime and the role of gambling within organized crime’s
activities. Without this information, we cannot recommend that the NFL no longer obligate clubs to report
information on the status of players.
609
An additional purpose of the NFL’s Injury Reporting Policy also concerns the integrity of the game.
Certain types of injuries on certain players are more important than other types of injuries. For example,
an injury to the starting quarterback’s throwing shoulder has the potential to impact the game more than a
leg injury. Similarly, an injury to a defensive back’s ankle is generally more important than whether he
has a hand injury. Nevertheless, disclosure of the nature of a player’s injury presupposes that it is
somehow unfair if the other club does not know the nature of the opposing club’s player injuries. That is
not necessarily the case. If neither club knows the nature of the other club’s injuries, both clubs have an
equal (and fair) level of uncertainty.
Having identified areas of concern, we now turn to Recommendations for change.
H. Recommendations
Recommendation 2-A: The NFL, and to the extent possible, the NFLPA, should: (a) continue to
improve its robust collection of aggregate injury data; (b) continue to have the injury data analyzed by
qualified professionals; and, (c) make the data publicly available for re-analysis.
As explained above, each of the Big Four leagues and MLS seems to have a quality injury tracking
system, allowing for the accumulation of current information about the nature, duration, and cause of
player injuries. As stated above, we rely on this data in this Report because it provides the best available
data concerning player injuries, although we cannot independently verify the data’s accuracy.
Nevertheless, if accurately collected, this data has the potential to improve player health through analysis
by qualified experts so long as it is made available to them. In particular, analysis potentially could be
!
98!
performed to determine, among other things, the effects of rule changes, practice habits, scheduling, new
equipment, and certain treatments, while also identifying promising or discouraging trends and injury
types in need of additional focus.
610
Notably, the NFL already conducts this type of analysis through
Quintiles.
However, the NFL does not publicly release its aggregate injury data (nor does any other league).
611
The
NFL does release some data at its annual Health & Safety Press Conference at the Super Bowl. However,
the data released at the Press Conference is minimal compared to the data available and the analyses
performed by Quintiles. For the data to have the potential meaningful applications mentioned above, it
must be made available in a form as close to its entirety as possible. Such disclosure would permit
academics, journalists, fans, and others to analyze the data in any number of ways, likely elucidating
statistical events, trends, and statistics that have the opportunity to improve player health. To be clear we
are recommending the release of more aggregate data, not data that could lead to identification of the
injuries of any particular player or cause problems concerning gambling.
Publicly releasing injury data, nevertheless, comes with complications that we must acknowledge. While
more transparency in injury reporting is necessary, the nuances of such data can easily be lost on those
without proper training. Sports injury prevention priorities in public health can be swayed by public
opinion and heavily influenced by those with the most media coverage. Making injury data publicly
available may allow those with the media access to dictate the agenda regardless of the actual
implications of the data. As a result, it may be harder for injury trends that may be more hazardous, but
less visible in the media, to get the attention they need, even when the data clearly shows the importance
of these issues. Thoughtful, balanced, peer-reviewed results may have difficulty competing against those
statistics which garner the most media attention. For this and other reasons, in our report Protecting and
Promoting the Health of NFL Players: Legal and Ethical Analysis and Recommendations, we
recommended that “[t]he media… engage appropriate experts, including doctors, scientists, and lawyers,
to ensure that its reporting on player health matters is accurate, balanced, and comprehensive.”
612
The
medical, scientific, and legal issues concerning player health are extremely complicated, which demands
that the media take care to avoid making assertions that are not supported or that do not account for the
intricacies and nuance of medicine, science, and the law.
In light of these concerns, one possible intermediate solution is to create a committee of experts that can
review requests for data and determine whether or not the usage of the data is appropriate and will
advance player health. Indeed, the Datalys Center for Sports Injury Research and Prevention performs this
role concerning access to NCAA student-athlete injury data.
613
Moreover, such committees have also been
formed in the clinical research setting.
614
Recommendation 2-B: Players diagnosed with a concussion should be placed on a short-term injured
reserve list whereby the player does not count against the Active/Inactive 53 man roster until he is
cleared to play by the NFL’s Protocols Regarding Diagnosis and Management of Concussions.
615
According to the leading experts, 80–90% of concussions are resolved within seven to ten days.
616
Thus,
concussion symptoms persist for longer than ten days for approximately 10–20% of athletes. In addition,
there are a variety of factors that can modify the concussion recovery period, such as the loss of
consciousness, past concussion history, medications, and the player’s style of play.
617
Consequently, a
player’s recovery time from a concussion can easily range from no games to several games. The uncertain
recovery times create pressure on the player, club, and club doctor. Each roster spot is valuable and clubs
constantly add and drop players to ensure they have the roster that gives them the greatest chance to win
each game day. As a result of the uncertain recovery times for a concussion, clubs might debate whether
they need to replace the player for that week or longer. The club doctor and player might also then feel
pressure for the player to return to play as soon as possible. By exempting a concussed player from the 53

!
99!
man roster, the club has the opportunity to sign a short-term replacement player in the event the
concussed player is unable to play. At the same time, the player and club doctor would have some of the
return-to-play pressure removed.
In fact, MLB already has such a policy. MLB has a seven-day Disabled List (as compared to its normal
10- and 60-day Disabled Lists) “solely for the placement of players who suffer a concussion.”
618
Why treat concussions differently than other injuries in this respect? This is a fair question to which there
are a few plausible responses. First, in terms of the perception of the game by fans, concussions have
clearly received more attention than any of the other injuries NFL players might experience and thus the
future of the game depends more critically on adequately protecting players who suffer from them.
Second, concussions are much harder to diagnose than other injuries, such that there may be a period of
uncertainty in which it would be appropriate to err on the side of caution.
619
Third, both players and
medical professionals have more difficulty anticipating the long-term effects of concussions as compared
to other injuries, given current scientific uncertainties concerning brain injury.
620
Fourth, and perhaps
most importantly, it is much harder to determine the appropriate recovery times for concussions as
compared to other injuries.
621
These reasons all support a recommendation to exclude concussed players
from a club’s Active/Inactive roster, but we recognize that the key feature of players potentially feeling or
facing pressure to return before full recovery may be shared across any injury a player may experience.
Thus, it may also be reasonable to consider extending this recommendation to injuries beyond
concussions.
622
In reviewing a draft of our Report, Protecting and Promoting the Health of NFL Players: Legal and
Ethical Analysis and Recommendations, the NFL argued that “[t]he current NFL roster rules actually
provide greater flexibility” than is recommended here.
623
The NFL explained that because “[t]here is no
limitation on how long a player may be carried on the 53-man roster throughout the season without being
‘activated,’… a player who is concussed routinely is carried on his club’s 53-man roster without being
activated until he is cleared.”
624
However, for the reasons explained above, we believe concussions should
be treated differently. All 53 spots on the roster are precious to both the club and the players. The
uncertainty surrounding recovery from a concussion presents unique pressures that can be lessened with
the approach recommended here.
Indeed, the NFL’s practice has been to treat concussions differently from other injuries. As part of its
Concussion Protocol, players suspected of having suffered a concussion during a game are examined by
doctors unaffiliated with the club, and to be cleared to play in the next game they must be cleared by
doctors unaffiliated with the club. For all other injuries, club doctors are the only ones to examine and
clear players to play. Additionally, in 2016, the NFL sent a memo to all clubs directing them not to
comment on a player’s progress in returning from a concussion.
625
Instead, the NFL directed clubs to state
only “that the player is in the concussion protocol under the supervision of the medical team, and the club
will monitor his status.”
626
This is in contrast to the clubs’ open discussion of players’ other injuries.
The Washington football club essentially proposed our recommendation at the 2016 owners' meetings.
Washington proposed amending the NFL bylaws to provide that a player who has suffered a concussion,
and who has not been cleared to play, be placed on the club’s Exempt List, and be replaced by a player on
the club’s Practice Squad on a game-by-game basis until the players is cleared to play. Unfortunately, the
proposal was not adopted.
Recommendation 2-C: The NFL should consider removing the requirement that clubs disclose the
location on the body of a player’s injury from the Injury Reporting Policy.

!
100!
In our Report Protecting and Promoting the Health of NFL Players: Legal and Ethical Analysis and
Recommendations, we recommend the NFL consider fining and/or suspending players if they discuss or
encourage targeting another player’s injury.
627
However, the need for this Recommendation would be
reduced if the NFL’s Injury Reporting Policy did not openly disclose the location on the body of players’
injuries, a requirement imposed only by the NFL, NBA and MLS.
The gambling-related interests of full disclosure likely do not outweigh the risks of targeting by other
players created by the Injury Reporting Policy.
628
While additional data—including from federal law
enforcement authorities—could inform this analysis—it seems unlikely that the risks of injury
information being sold on a black market are so high to justify a known risk of players intentionally
aiming to hit a player in an area known to be injured because of the Injury Reporting Policy. Similarly,
we see no inequity in clubs not knowing the full extent of an opposing club’s player injuries.
Consequently, we recommend that the NFL consider removing the requirement that clubs disclose the
location of a player’s injury from the Injury Reporting Policy.
CHAPTER 3: HEALTH-RELATED BENEFITS
In this Chapter, we summarize the various health-related benefits available to the players in each of the
leagues. Specifically, for each league, we examine: (1) retirement benefits; (2) insurance benefits; (3)
disability benefits; (4) workers’ compensation benefits; (5) education-related benefits;
629
and, (6) the
existence of health-specific committees jointly run by the league and players association. Each of these
domains is relevant to protecting players should they experience negative health effects during and after
their playing years, and also to promoting their ability to maintain their health and well-being over the
longer term. Given that a decision to play or continue to play professional sports, like many other
decisions, is a matter of weighing risks and benefits, those decisions must be made against a backdrop of
available benefits. It is for this reason that we spend considerable space describing and evaluating the
available benefits in each league.
Before we begin our analysis of the leagues’ health-related benefits, there are a few prefatory notes that
should frame our analysis.
Financial Health
Our goal is to examine all the inputs that may influence players’ health, including the so-called “social
determinants of health.” Financial health is a major contributor to physical and mental health, and also, in
turn, affected by physical and mental health.
630
Indeed, many studies have shown a correlation between
financial debt and poor physical health.
631
While the actual career earnings of NFL players are difficult to
ascertain,
632
there have been multiple studies about NFL player financial health with a variety of results.
According to a 2009 Sports Illustrated article, by the time NFL players have been retired for two years,
78% of them are bankrupt or in financial distress.
633
But other studies have somewhat different findings.
According to a 2009 NFL-funded study of former NFL players by the University of Michigan, the median
income of a former player between the ages of 30 and 49 is $85,000, compared to $55,000 for the general
population. The study also found that 8.4% of former players between 30 and 49 were below the poverty
level, as compared to 9.5% of the general population.
634
A 2015 academic study also found different
results than those arrive at in the Sports Illustrated article, finding that within two years of the end of their
career, only 1.9% of players were bankrupt—while also finding that one in six players was bankrupt
within 12 years of leaving the NFL.
635
Moreover, in 2012, ESPN released the documentary Broke
detailing the financial problems of professional athletes, and exploring how they had gotten there.
636
And
in a 2014–15 survey of 763 former players by Newsday, 50.59% of former players interviewed said they
had struggled financially since their playing career ended.
637
!
101!
There are, however, important limitations to the above-mentioned studies.
First, to support its claims Sports Illustrated cited “reports from… athletes, players’ associations, agents
and financial advisers”
638
but no additional details and no information that can be independently verified.
Second, there are two potential limitations to the Michigan Study. First, the study population only
included players who had vested rights under the NFL’s Retirement Plan; meaning, the players generally
had been on an NFL roster for at least three games in at least three seasons. However, there is likely a
significant but unknown percentage of NFL players that never become vested under the Retirement Plan.
Second, responders to the survey were 36.8% African-American and 61.4% White—almost a complete
reversal of the NFL’s population of current players. While the racial demographics of former players is
likely closer to the population of the Michigan Study, i.e., there were formerly more white players than in
the current NFL, the Michigan Study did not provide such data on the former player population and did
not adjust or account for the racial demographics of the former player population. We discussed the
Michigan Study in a telephone call with Dr. David Weir, the Study’s lead author. Dr. Weir explained that:
(1) due to limited resources, the population of players to be studied and contacted was limited to the data
and contact information available to and provided by the NFL; and, (2) the NFL did not provide racial
demographics of former players and thus the study could not adjust for that factor. Weir also believes that
the racial demographics of former players is substantially similar to the racial demographics of the
Michigan Study’s participants. Finally, Weir explained that, during the internal review process with the
NFL, the study was leaked to the media, preventing the study from being amended and submitted to a
peer-reviewed publication.
Finally, there are also limitations to the Newsday survey: (1) the survey was sent via email and text
message by the NFLPA to more than 7,000 former NFL players, thus eliminating former players who
were less technologically savvy and also possibly skewing the sample towards those former players closer
to the NFLPA; (2) the response rate for the survey was low (approximately 11%); and, (3) the study does
not discuss the demographics of respondents, making it difficult to ascertain whether those who
responded are a representative sample of all former players.
Despite these limitations, we provide the reader with the best existing data. Moreover, while there are
limitations to the data collected to date as well as differences in the figures presented, it is clear that there
are serious concerns about former players’ financial difficulties.
639
The relationship between physical and financial health goes in both directions. Without adequate savings
and benefits during and after NFL play, players may find themselves insufficiently prepared to meet their
physical and mental health needs, especially in the event of crisis. Furthermore, crises in physical and
mental health are closely tied to bankruptcy, home foreclosure, and other serious financial setbacks.
640
At
its worst, these circumstances can lead to a vicious cycle—poor health outcomes lead to financial losses,
which worsen the ability to combat physical and mental health impairments, which in turn further deplete
financial resources.
Financial health is also in and of itself an important component of a person’s health. Financial difficulties
can cause stress that contributes to or exacerbates psychological and physical ailments.
For all of the above reasons, it is thus critical that we examine the financial benefits available to players,
including but not limited to retirement and investment plans.
Workers’ Compensation
!
102!
Most of the benefits discussed herein are fairly straight-forward, but it is helpful to explain workers’
compensation benefits more fully. “Workers’ compensation laws provide protections and benefits for
employees who are injured in the course of their employment. In the typical case, the workers’
compensation regime grants tort immunity to employers in exchange for the regime’s protections and
benefits to the employee,”
641
without the employee having to prove the employer was at fault, as they
would have to in a typical tort lawsuit. While workers’ compensation laws, systems and benefits vary
widely among the states, workers’ compensation generally provides two important benefits to workers:
(1) monetary compensation; and, (2) coverage for medical care. We discuss each of these benefits in turn.
Workers’ compensation payments typically depend on the employee’s level of injury or disability and the
extent to which the injury or disability affects the employee’s ability to continue working. Generally,
workers receive “around one-half to two-thirds of the employee’s average weekly wage.”
642
In addition,
the amount of benefits is subject to maximums which are usually tied to the state’s average weekly
wage,
643
and are generally between $500 and $1,000.
644
The benefits continue so long as the employee is
disabled or unable to work. Additionally, the amount a player receives in workers’ compensation often
reduces the amount a club is obligated to pay the player for certain other CBA-provided benefits.
645
Again, it is important to bear in mind that these benefits and schemes can vary widely among the states.
Medical care coverage is an important benefit available to players through workers’ compensation. Often,
if a player is injured during the season, he is entitled to medical care from the club during the season of
injury only.
646
Consequently, if a player suffers an injury that causes him to have ongoing or recurring
healthcare needs (such as surgeries) well beyond the season of injury (and for perhaps the rest of his life),
the club will have no obligation to pay for such care. Workers’ compensation fills that gap. Workers’
compensation statutes generally require the employer (in practice, usually the employer’s insurance
carrier) to pay for reasonable and necessary medical expenses that are the result of an injury suffered in
the workplace in perpetuity. More importantly, the worker does not have to pay for any part of the care.
Availability of Plan Documents
Although we analyze the leagues’ various benefit programs, many of the actual plan documents—to the
extent they exist—are not publicly available.
647
Typical plan documents for these kinds of benefits are
dozens or hundreds of pages long, detailing a variety of intricacies and nuances in the plans. Without the
ability to review those plans in detail, we rely on the summaries provided in the CBAs (which vary in
detail) and other publicly available information. Consequently, readers should not consider these
summaries as definitive statements concerning the leagues’ various benefit programs, but instead as
informed general explanations.
Comparing the Plans
In Tables 3-J and 3-K below, we provide our best estimates of the Big Four Leagues’ retirement/pension
plans. While we do our best to summarize the amounts potentially available to players under all of the
various plans, we stress caution in extrapolating data from our analyses and summaries. The benefit plans
contain intricate legal, financial, and actuarial components that determine a player’s ultimate entitlement.
For example, many of the plans contain offsets concerning other benefits, such that if a player is receiving
payments under a retirement plan, any amounts he could receive for disability benefits are likely to be
decreased. The eligibility criteria for the various benefits also vary within and across the leagues.
Consequently, it is difficult to determine in generalities the amounts to which a former player might be
entitled.
!
103!
Other Benefits
In considering the scope of health-related benefits available to players, it is important also know that the
degree to which players are able to collect the full balance of their contracts varies depending on the
league and the player’s individual contract. In Chapter 5: Compensation, we examine the degree to which
player compensation is guaranteed. For our purposes here, we are focused on those benefits available to
protect and promote player health other than the compensation available as part of a player’s contract.
In addition, while this Chapter focuses on those benefits that are agreed to as part of the CBA, many if not
all of the leagues—and the corresponding unions—have other programs and benefits available to players
that are not a part of the CBA. For example, the NFL’s Player Engagement Department operates many
programs designed to help future, current, and former NFL players, with particular focus on transitioning
to a life after football.
648
Similarly, the NFLPA offers a variety of internships and educational programs
for players.
649650
Other leagues and unions likely have similar programs, but they are not well-publicized
and publicly-available details can be sparse. Consequently, while we focus on the benefits for which more
information is available, readers should understand that the leagues likely offer additional benefits to the
players.
***
With those prefatory and explanatory notes in mind, we turn to our analysis of the leagues’ various
benefit plans.
A. NFL Health-Related Benefits
As a preliminary matter, NFL player eligibility for many of the collectively-bargained benefits discussed
below depends on the number of “Credited Seasons” a player has earned. Generally, a player earns a
Credited Season when he is entitled to be paid for at least three regular season games.
651
Additionally, it is important to understand the relationship between player benefits and player salaries. In
the NFL, the players’ share of revenues is referred to as the Player Cost Amount.
652
The Player Cost
Amount is one of two essential components for calculating the Salary Cap, which is the “absolute
maximum amount of Salary that each club may pay or be obligated to pay or provide to players… at any
time during a particular League Year.”
653
The other essential component of the Salary Cap calculation is
Player Benefit Costs. Player Benefit Costs are the total amounts the NFL and its clubs spend on all the
programs and benefits described herein, in addition to the costs of providing medical care to NFL
players.
654
The Salary Cap is determined by subtracting Player Benefit Costs from the Player Cost
Amount and dividing by the number of clubs in the NFL.
655
In other words, the Salary Cap equals Player
Cost Amount minus Player Benefit Costs divided by 32. Thus, the more that is paid to NFL players—
including retired players—in the form of benefits and medical care, i.e., Player Benefits Cost, the less
they are able to receive in the form of salary. Indeed, in 2015, when the Salary Cap was $143,280,000 per
club, each club was charged $37,550,000 in Player Benefit Costs. Thus, out of a possible $180,830,000
that could have been spent on player salaries by each club, 26.2% was allocated to player benefits.
It is important to clarify these numbers. As Figure 3-A shows below, about 50% of a club’s revenue is
allocated toward the players. The club keeps the other 50%. Of the 50% allocated for the players (the
Player Cost Amount), in 2015, 26.2% of that was used on player benefits. Thus, in 2015, we can estimate
that each club had approximately $361,660,000 in revenue, $180,830,000 of which would be available for
players. $37,550,000 was spent on player benefits. The $37,550,000 is 26.2% of the Player Cost Amount
and 10.4% of the club’s revenue.
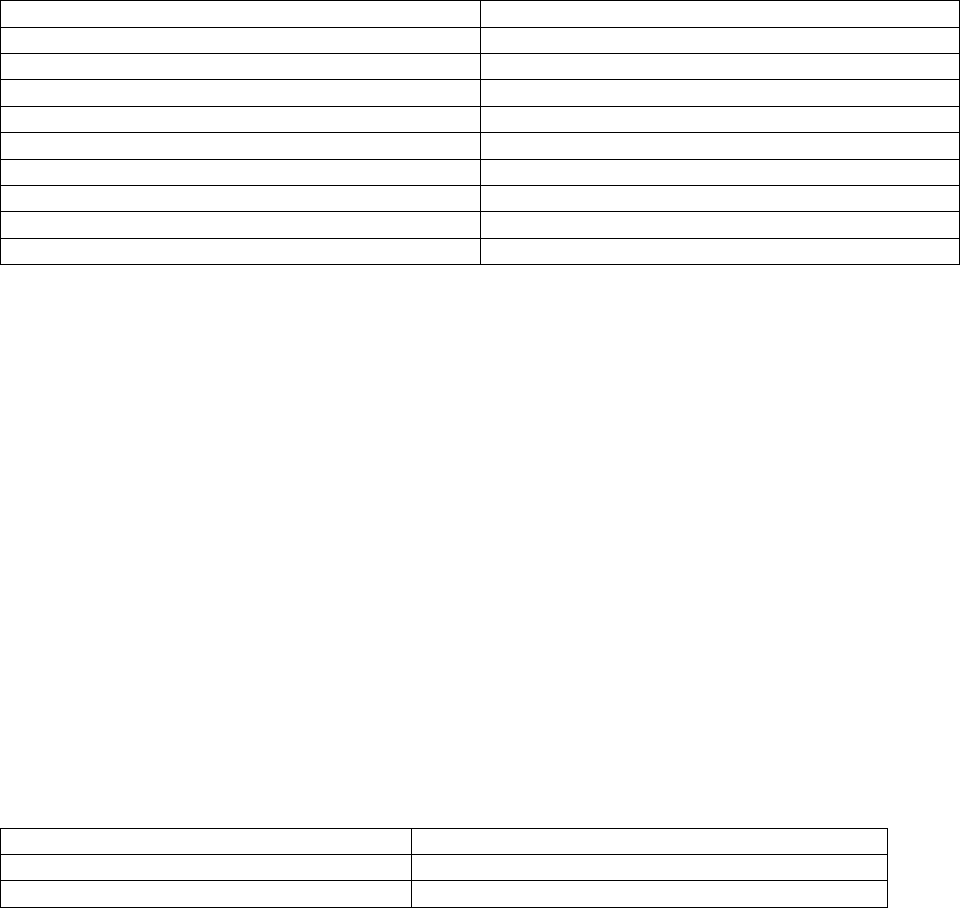
!
104!
1. Retirement Benefits
The NFL provides four retirement-focused benefits: (a) the Severance Pay Plan; (b) the Bert Bell/Pete
Rozelle NFL Player Retirement Plan (“Retirement Plan”); (c) the Player Annuity Plan; and, (d) the
Second Career Savings Plan.
a. Severance Pay Plan
656
The Severance Pay Plan, first created in 1982, entitles eligible players to severance pay for each Credited
Season. To be eligible, a player must have at least two Credited Seasons, at least one of which was in
1993 or later. A player becomes eligible for the lump sum severance payment 12 months after his last
contract expired or was terminated. Table 3-A below summarizes the amount of benefits available to
players under the Severance Pay Plan.
Table 3-A: NFL Severance Pay Plan Benefits
657
Seasons
Amount for Each Credited Season
1989–92
$5,000
1993–99
$10,000
2000–08
$12,500
2009
$15,000
2010
0
2011
$15,000
2012–13
$17,500
2014–16
$20,000
2017–20
$22,500
For example, a player who played from 1998 through 2009 would be entitled to a severance payment of
$147,500: $10,000 for each of his two seasons between 1998 and 1999 ($20,000); $12,500 for each of his
nine seasons between 2000 and 2008 ($112,500); and, $15,000 for 2009.
b. Retirement Plan
658
The NFL’s Retirement Plan, first created in 1968, provides eligible players with retirement benefits, and
offers survivor benefits for players’ wives and family. Generally, only “Vested Players” are eligible for
retirement benefits. A Vested Player is a player who fits one of the following criteria: (1) has three or
more Credited Seasons, including at least one Credited Season after 1992; (2) has four or more Credited
Seasons, including at least one Credited Season after 1973; or, (3) has five or more Credited Seasons.
Vested Players can receive monthly retirement benefits for life beginning at age 55. Players with a
Credited Season before 1993 can receive reduced monthly benefits as early as age 45. A player can elect
to receive retirement benefits until his death or defer some of the benefits to his family upon death. In
order to begin receiving his retirement benefits at age 55, a player must file for them. If a player has not
filed for them, he will automatically begin receiving the benefits at age 65. Table 3-B shows the monthly
benefits per credit season of the Retirement Plan. These benefits are additive, meaning the player’s
monthly benefits are the sum of the monthly benefits to which he is entitled for each Credited Season.
Table 3-B: NFL Retirement Plan Benefits (If Taken after Age 55):
Credited Season
Monthly Benefit Credit per Credited Season
Before 1982
$250
1982–1992
$255
!
105!
1993–1994
$265
1995–1996
$315
1997
$365
1998–2011
$470
2012–2014
$560
2015–2017
$660
2018–2020
$760
In addition, the Retirement Plan includes $620 million in Legacy Benefits created as part of the 2011
CBA for players who played before 1993. The Legacy Benefits listed in Table 3-C below are in addition
to the Retirement Benefits listed above.
Table 3-C: NFL Retirement Plan Legacy Benefits
Credited Season
Monthly Legacy Benefit per Credited Season
Before 1975
$124
1975–1992
$108
According to the NFL, as of 2015, 3,641 former players receive an average monthly retirement benefit of
$1,656,
659
for a total of approximately $72,353,952 annually. In addition, about 90% of those former
players also received Legacy Benefit payments, with an average monthly payment of $723.85,
660
for a
total of approximately $28,464,677 in Legacy Benefit payments. Thus, in 2015, the NFL Retirement Plan
paid a little over $100 million to former NFL players.
The Retirement Plan—which until 2011 also covered disability benefits—historically has been viewed
negatively by former players. The filing process has been considered complex and lengthy,
661
resulting in
many former players suing the Retirement Plan concerning their benefits.
662
During a 2007 hearing before
the United States Senate Committee on Commerce, Science, and Transportation, it was revealed that only
317 former players were receiving disability benefits, out of the thousands that were eligible.
663
Of additional concern, in recent years the NFLPA has been warning players that the Retirement Plan is
underfunded.
664
Currently, the Plan only takes in enough money to cover about 54.5% of what it pays
out,
665
jeopardizing its ability to pay retirement benefits in the future.
Tables 3-J and 3-K at the conclusion of this Chapter put these numbers in context, comparing monthly
payments under the leagues’ various retirement/pension plans.
c. Player Annuity Plan
666
The Player Annuity Plan, first created in 1998, provides deferred compensation to players.
667
Players
automatically contribute to the Annuity Plan through payroll deductions, which are then invested. The
Annuity Plan is divided between a Qualified Account and a Nonqualified Account. The Qualified
Account includes the maximum amount of compensation that can be deferred on a pre-tax basis pursuant
to IRS rules. The maximum amount that could be deferred on a pre-tax basis in 2016 was $53,000.
668
The
amount contributed to the Annuity Plan above this amount is the Nonqualified Account portion and must
be taxed before being invested as part of the Annuity Plan.
To be eligible for the Annuity Plan, a current or former player must have at least one Credited Season. So
long as the player is active, compensation will be deducted from his pay to fund his Annuity Plan

!
106!
account. A player does not vest
669
in his Qualified Account until he has earned at least three Credited
Seasons, but a player is always vested in his Nonqualified Account.
A player can elect to receive a distribution at any time after he is done playing, provided the player is at
least 45, or is at least 35 and five years have elapsed since the player last earned a Credited Season.
Distributions must begin no later than the first day of the month after the player turns 65. Players can also
elect different forms of distribution for each of their accounts and different dates for payments to begin.
Payment forms include: (1) annual installments until the player reaches 45; (2) an annuity for life; (3) a
reduced annuity for life, with a survivor annuity beginning after the player’s death; (4) a lump sum, if the
former player is at least 45 when the lump sum is to be paid; and, (5) a partial lump sum, if the player is at
least 45 when the partial lump sum is paid, with the remainder paid in one of the other payment forms.
Table 3-D provides details on this program.
Table 3-D: NFL Player Annuity Plan Deferred Compensation Amounts (2016 Season)
Credited Seasons
Total Amount Allocated to Annuity Plan for That Season
1
$0
2
$5,000
3
$5,000
4
$70,000
5 or more
$80,000
The reason for the large increase in allocation from the third to fourth Credited Season is likely due to the
vesting requirements. As stated earlier, a player is not vested in his Qualified Account—which represents
the bulk of the Annuity Plan contribution—until after his third Credited Season. If he does not vest in the
Qualified Account, it is forfeited. Thus, by minimizing the amounts allocated before players vest in the
Annuity Plan, the Annuity Plan minimizes the amount of deferred compensation that might be forfeited.
d. Second Career Savings Plan
670
The Second Career Savings Plan, first created in 1993, is a 401(k)
671
plan that helps players save for
retirement in a tax-favored manner. All NFL players are eligible for the Plan, regardless of the number of
Credited Seasons.
To fund the Plan, the player’s club is required to contribute a minimum of: $1,000 if the player has
exactly one Credited Season; $7,200 if the player has exactly two Credited Seasons; and, $3,600 if the
player has three or more Credited Seasons. In addition, the club will contribute $2 for every $1
contributed by a player during a year in which the player earned a Credited Season, provided the player
already has at least one Credited Season, up to a maximum of $26,000 between 2015 and 2018, and
$28,000 between 2019 and 2020. Players are automatically enrolled in the plan, with 10% of their pre-tax
salary going towards the plan. Players can change the amount of their contributions or opt out of the plan
at any time.
A player can receive benefits after he is 45 provided the player is not employed by a club,
672
or after the
player is 59½. The player can receive the benefits in a variety of forms: (1) a single lump sum payment;
(2) installments over ten years; (3) an annuity for the player’s life; or, (4) an annuity for the player’s life
and surviving spouse’s life.
According to the NFLPA, 99% of NFL players are enrolled in the Second Career Savings Plan.
673

!
107!
2. Insurance Benefits
The NFL provides four insurance-related benefits: (a) the Player Insurance Plan; (b) the Health
Reimbursement Account Plan; (c) the Long Term Care Insurance Plan; and, (d) the Former Player Life
Improvement Plan.
a. Player Insurance Plan
674
The NFL Player Insurance Plan, first created in 1968, provides players and their immediate family with
life insurance, accidental death and dismemberment insurance, medical coverage, dental coverage, and
wellness benefits. The wellness benefits include access to clinicians for mental health, alcoholism, and
substance abuse, child and parenting support services, elder care support services, pet care services, legal
services, and identity theft services.
Any player in the NFL, including a practice squad player, is eligible for the Player Insurance Plan. Players
who are vested under the Retirement Plan continue to receive coverage for five years after their career
ends. Players who are not vested are only covered through the end of the plan year in which they play
their last game.
After their career has ended, players have the option of continuing coverage pursuant to the Consolidated
Omnibus Budget Reconciliation Act (“COBRA”)
675
for a period of 18, 29, or 36 months. Players are
required to pay the full cost of coverage plus 2% for administrative costs.
It is important to note that COBRA is an extension of healthcare coverage that employers are required to
provide as a matter of law. Thus, NFL clubs are not unique in providing COBRA coverage, and all of the
American clubs in the leagues discussed herein are also be obligated to provide COBRA coverage to their
former players. In contrast, former players who are residents of Canada can generally obtain healthcare
through government-funded plans at any time during or after their playing career.
b. Health Reimbursement Account (“HRA”) Plan
676
The HRA Plan, first created in 2006, helps to pay out-of-pocket healthcare expenses after players are no
longer employed by an NFL club and after the period of extended medical coverage under the Player
Insurance Plan that is paid by the NFL has ended.
677
To be eligible, players whose last Credited Season
was in 2004 or 2005 must have at least eight Credited Seasons, or, players whose last Credited Season
was in 2006 or later must have at least three Credited Seasons.
A player is eligible to withdraw amounts from his HRA Plan account for medical expenses incurred
provided he files for reimbursement within 24 months of receiving the medical bill to be reimbursed.
To fund the players’ HRA Plan accounts, clubs contribute the amounts to each player’s Health Account.
Players do not contribute their own money to their Health Account. Details on the HRA plan contribution
scheme can be found in Table 3-E.
Table 3-E: NFL HRA Plan Account Contributions
Credited Seasons
Health Account Contribution per Credited Season
per Player
2009 and prior
$25,000
2010
$0
2011–2015
$25,000

!
108!
2016–2020
$30,000
c. Long Term Care Insurance Plan
The Long Term Care Insurance Plan, first created in 2011, provides medical insurance to cover the costs
of long-term care for NFL players (but not their family members). Players are eligible for the Long Term
Care Insurance Plan if they are: (1) vested players under the Retirement Plan; (2) between the ages of 50
and 76; and, (3) have been certified by a licensed healthcare provider as requiring critical supervision, or
requiring the presence of another person within arm’s reach due to inability to perform a required number
of defined activities of daily living. The Plan provides benefits of $150 a day for a maximum of four
years.
678
Players are not required to contribute to the funding of the Plan. In addition, the Plan provides benefits to
all former players who are eligible.
d. Former Player Life Improvement Plan
679
The Former Player Life Improvement Plan, first created in 2007, permits qualifying former players (and
in some cases their dependents) not otherwise covered by health insurance to receive reimbursement for
medical costs for “joint replacements, prescription drugs, assisted living, Medicare supplemental
insurance, spinal treatment, and neurological treatment.” Former NFL players who are vested under the
Retirement Plan are eligible for the plan. However there are many benefits under this plan, some of which
have additional eligibility requirements, so not every player is eligible for every benefit.
3. Disability Benefits
The NFL provides two disability-related benefits: (a) the Disability & Neurocognitive Benefit Plan; and,
(b) the 88 Plan.
a. Disability & Neurocognitive Benefit Plan
680
The Disability & Neurocognitive Benefit Plan provides eligible players with disability benefits, including
benefits based on neurocognitive disability. The Plan provides four types of benefits: (1) Total and
Permanent Disability Benefits; (2) Line-of-Duty Disability Benefits; (3) Mild Neurocognitive Disability
Benefits; and, (4) Moderate Neurocognitive Disability Benefits.
A player is eligible for “Total and Permanent Disability Benefits” if the Initial Claims Committee
681
or
Disability Board
682
determines “(1) that he has become totally disabled to the extent that he is
substantially prevented from or substantially unable to engage in any occupation or employment for
remuneration or profit…, and (2) that such condition is permanent.”
A player is awarded Total and Permanent Disability Benefits pursuant to one of four categories: (1)
Active Football: the player is an active player and the disability results from NFL activities;
683
(2) Active
Nonfootball: the player is an active player but the disability does not result from NFL activities; (3)
Inactive A: the player is a former player who filed for disability benefits within 15 years of his last
Credited Season; or, (4) Inactive B: the player is a former player who filed for disability benefits more
than 15 years after his last Credited Season. Inactive A and Inactive B disability benefits do not have an
eligibility requirement that the disability resulted from NFL activities.
A player is eligible for Line-of-Duty Disability Benefits if the Initial Claims Committee or Disability
Board determines that the player “incurred a substantial disablement… arising out of [NFL] football
!
109!
activities.” Line-of-Duty Disability Benefits address those injuries or disabilities that are not considered
permanent.
A player is eligible for Neurocognitive Disability Benefits if: (1) the player is vested under the Retirement
Plan; (2) the player is under age 55; (3) the player had at least one Credited Season after 1994; (4) the
player does not receive retirement benefits; (5) the player does not receive total and permanent disability
benefits; (6) the player executes a release releasing the NFL and clubs from any liability for head or brain
injuries; and, (7) the player is determined to have mild or moderate neurocognitive impairment.
A player has “mild neurocognitive impairment if he has problems with one or more domains of cognitive
functioning which reflect acquired brain dysfunction but are not severe enough to cause marked
interference in day-to-day activities.”
A player has “moderate neurocognitive impairment if he has problems with one or more domains of
cognitive functioning which reflect acquired brain dysfunction resulting in marked interference with
everyday life activities, but not severe enough to prevent the Player from working.”
A player must submit to a medical examination by a doctor of the Disability Board’s choosing to
determine if the player has neurocognitive impairment.
Details on the disability and neurocognitive benefits can be found in Table 3-F.
Table 3-F: NFL Disability & Neurocognitive Benefits
Type of Disability
Monthly Benefit
Total & Permanent: Active Football
$22,084
Total & Permanent: Active Nonfootball
$13,750
Total & Permanent: Inactive A
$11,250
Total & Permanent: Inactive B
$5,000
Line-of-Duty
$3,000
Mild Neurocognitive
$2,250
Moderate Neurocognitive
$4,000
A player can only receive one of the above benefits at any one time.
According to a 2010 analysis of the NFLPA’s disability claims database, disability benefit applications
had never exceeded 200 applications in a year until 2008 and 2009, when there were more than 400
claims in both years.
684
As of 2010, NFL disability benefit claims were approved approximately 38% of
the time.
685
Importantly, the benefits criteria changed after the 2011 CBA, so current data would not be
comparable. Moreover, according to the same analysis, of the players who filed for disability benefits, the
mean age at which they retired from the NFL was 30.2 years.
686
Additionally, the mean age at which the
player filed for disability benefits was 38.1 years.
687
Finally, through the year 2009, there had been a total of 2,670 disability benefit claims, with 2,423
(90.7%) for orthopedic conditions, 52 (1.9%) for neurological conditions, 18 (0.7%) for psychological
conditions, 18 (0.7%) for cardiovascular conditions, and 159 for other unspecified conditions (6.0%).
688
b. The 88 Plan
689
The 88 Plan, first created in 2006, provides former players suffering from dementia, ALS, or Parkinson’s
disease with benefits. The 88 Plan is named for John Mackey, a Hall of Fame tight end for the Baltimore
!
110!
Colts and San Diego Chargers from 1963–72, who wore number 88 during his career. Mackey suffered
from dementia later in life and died in 2011 at the age of 69.
Vested Players under the Retirement Plan and players who have received Total and Permanent Disability
Benefits under the Disability & Neurocognitive Benefit Plan who have been diagnosed with dementia,
ALS, or Parkinson’s disease are eligible. The 88 Committee, consisting of an NFL designee and an
NFLPA designee, determines whether the player qualifies for the benefit.
The 88 Plan will reimburse or pay the following costs for medical care that are related to a player’s
Dementia, ALS, or Parkinson’s disease: (1) institutional care; (2) home custodial care provided by an
unrelated third party; physician services; (3) durable medical equipment; and, (4) prescription medication.
The maximum benefits are $130,000 per year so long as the player continues to suffer from Dementia,
ALS or Parkinson’s disease. Finally, there is no requirement that the player prove that his condition is
related to his NFL career.
4. Workers’ Compensation Benefits
The NFL CBA requires clubs to provide workers’ compensation coverage or comparable benefits,
including clubs that are “in any state where workers’ compensation coverage is not compulsory or… [are]
excluded from a state’s workers’ compensation coverage[.]”
690
The second part of the preceding sentence
is important. Florida, for example, does not require employers to provide workers’ compensation
coverage.
691
Consequently, players with the Miami Dolphins, Tampa Bay Buccaneers, and Jacksonville
Jaguars would not have workers’ compensation coverage without this provision. Nevertheless, workers’
compensation benefits and statutes have been contentious issues in the NFL. In recent years, the NFL and
its clubs have sponsored legislation in several states, including California, Illinois and Louisiana, to
restrict players’ workers’ compensation benefits.
692
5. Education-Related Benefits
The NFL’s Tuition Assistance Plan, first created in 2002, reimburses players for tuition, fees, and book
costs associated with attending an eligible educational institution. All current NFL players with at least
one Credited Season are eligible for the plan. In addition, former players with at least five Credited
Seasons are also eligible, provided that the costs are incurred within four years of the player’s last season.
For any course in which players seek to use this benefit for reimbursement, the player must have received
a “C” or better in the course and submit his claim for reimbursement within six months of when the final
grade is issued. The maximum reimbursement is $20,000 per year.
693
A former player with at least five
Credited Seasons is eligible for up to $60,000 in reimbursements total.
6. Joint Health-Specific Committees
There are two health-related committees provided for in the NFL CBA: (a) the Joint Committee on Player
Safety and Welfare (“Joint Committee”); and, (b) the Accountability and Care Committee (“ACC”).
a. Joint Committee on Player Safety and Welfare
The Joint Committee, first established in 1977, consists of three representatives chosen by the NFL and
three chosen by the NFLPA.
694
The Joint Committee’s purpose is to “discuss[] the player safety and
welfare aspects of playing equipment, playing surfaces, stadium facilities, playing rules, player-coach
relationships, drug abuse prevention programs and other relevant subjects.”
695
In addition, the NFLPA has
“the right to commence an investigation before the Joint Committee if the NFLPA believes that the
medical care of a team is inadequate.
696
!
111!
While a complaint to the Joint Committee results in a review by neutral physicians, the definition of the
scope of that review process’ authority is vague. The Joint Committee is obligated to act upon the
recommendations of the neutral physicians, but it is unclear what it means for the Joint Committee to act
and there is nothing obligating the NFL or any club to abide by the neutral physicians’ or Joint
Committee’s recommendations. Moreover, there is no indication that the neutral physicians or Joint
Committee could award damages to an injured player.
697
In 2012, the NFLPA commenced the first and only Joint Committee investigation.
698
The nature and
results of that investigation are confidential per an agreement between the NFL and NFLPA.
699
b. Accountability and Care Committee
The ACC, created in 2011, consists of the NFL Commissioner or his designee; the NFLPA Executive
Director or his designee; and six additional members “experienced in fields relevant to healthcare for
professional athletes,” three appointed by the Commissioner and three by the NFLPA Executive
Director.
700
The CBA dictates that the ACC is to: (1) encourage and support programs for outstanding
professional training by club medical staffs; (2) develop a standardized pre-season and postseason
physical examination and education protocol to inform players of the risks associated with playing
football; (3) conduct research into prevention and treatment of illness and injury commonly experienced
by professional athletes; (4) conduct a confidential player survey at least once every two years to solicit
the players’ input and opinion regarding the adequacy of medical care; (5) assist in the development and
maintenance of injury surveillance and medical record systems; and, (6) undertake such other duties as
the Commissioner and Executive Director may assign.
701
Additionally, players can make complaints about
their medical care to the ACC—but the ACC then refers those complaints to the NFL and club
involved.
702
***
With an understanding of the NFL’s health-related benefits, we now turn to our analysis of the other
leagues’ health-related benefits.
B. MLB Health-Related Benefits
As explained in the Introduction, Section C: Collective Bargaining Agreements, in the fall of 2016, MLB
and the MLBPA agreed to and ratified the terms of a new CBA. However, as of the date this Report went
to press, the parties had not yet published the new CBA. Thus, this Section principally relies on
information contained in the 2012 CBA and other documents that existed prior to the new CBA.
Specifically, most of MLB’s health-related benefits are contained in the Major League Baseball Players
Benefit Plan (“Benefit Plan”)
703
includes many of the benefits in which we are interested.
704
In addition to
these documents, we rely on a joint press release issued by the parties summarizing the changes agreed to
in 2016. Nevertheless, the press release does not provide specifics of the changes to the Benefit Plan and
other benefits, i.e., it generally does not provide the amounts by which certain benefits increased. In
discussing certain benefits below, we will indicate those that we understand to have been changed as part
of the 2016 CBA negotiations, but caution the reader that important additional details, nuance or context
are likely to be contained in the full length CBA and a revised Benefit Plan when they are complete.
1. Retirement Benefits
The Benefit Plan includes a Pension Plan and an Investment Plan.
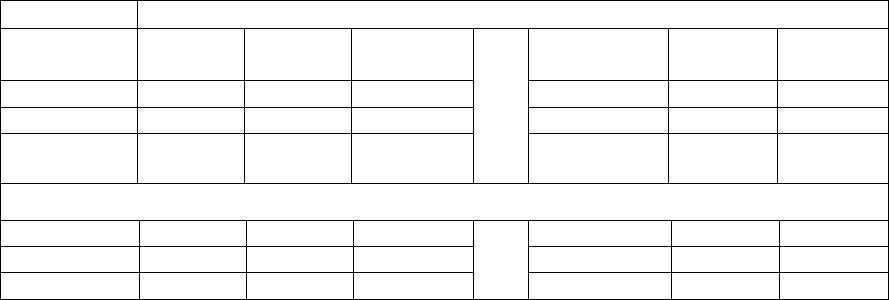
!
112!
a. Pension Plan
The Pension Plan provides monthly payments to eligible former players based on the time period during
which the player played, the player’s retirement age, years of service, and annual compensation.
705
In
2016, MLB and the MLBPA agreed that pension benefits for certain but unspecified classes of retired
players would be increased.
706
However, as discussed above, the specific amounts by which the benefits
increased is not yet publicly known. Thus, what follows is a summary of the Pension Plan prior to the
2016 CBA negotiations.
Fixed monthly payments range from a low of $85.10 to a high of $13,666, with higher payments for
players in more recent eras, players who retire at an older age, players with more years of service, and—
where applicable—players with higher average annual salaries.
707
Players also receive variable monthly
pension payments determined by a base monthly rate (calculated using the same factors as a player’s
fixed monthly payment) weighted by the investment performance of a fund for the variable benefits
relative to a baseline interest rate.
708
Variable monthly payments range from a low of $82 to a high of
$3,000.
709
Players who played in 1980 or later are eligible for the Pension Plan on the first day they are on an MLB
club’s roster.
710
Players who played prior to 1980 are eligible for the Pension Plan in three ways: (1) they
have four years of service;
711
(2) if they played prior to 1970, they reached the age of 65 prior to April 1,
1980;
712
and, (3) if they played in 1970 or later, they reached the age of 62 prior to April 1, 1980.
713
Players with fractional years of credited service receive an adjusted benefit amount.
714
Table 3-G below provides an abbreviated review of the Pension Plan benefits available to MLB players
who played after 1991 and earned a mean of at least $68,212 during the three years of their career during
which their salary was the highest. At the end of this Chapter, Tables 3-J and 3-K compare the monthly
payments of the Big Four leagues’ retirement/pension plans.
In reviewing the Tables below, it is important to understand that the “Retirement Age” is not the age at
which a player retired from MLB. Instead, it is a term used in the Pension Plan to indicate the age at
which a player begins to receive Pension Plan benefits. A player may “retire” for Benefit Plan purposes at
any time between his 45th and 70
1
/
2
th birthday.
715
It is unclear whether a player will receive any Pension
Plan benefits if they do not file for them. Finally, it is also important to note that the maximum annual
pension amounts for players who played after 1991 are generally adjusted annually to equal the
limitations on such plans set by the Internal Revenue Service.
716
In 2016, the limitation on the annual
contributions to pension plans was $210,000.
717
Table 3-G: MLB Player Combined Fixed and Variable Monthly Pension Payments for Players after
1991 (Abbreviated)
Years of Credited Service
Retirement
Age
1
2
3
***
8
9
10+
45
$525
$1,050
$1,575
$4,200
$4,725
$5,250
46
$557
$1,115
$1,673
$4,462
$5,020
$5,578
47
$593
$1,186
$1,779
$4,744
$5,337
$5,930
***
60
$1,427
$2,855
$4,283
$11,422
$12,850
$14,278
61
$1,541
$3,082
$4,624
$12,330
$13,872
$15,413
62
$1,666
$3,333
$5,000
$13,333
$15,000
$16,666
!
113!
b. Investment Plan
The Investment Plan is a 401(k) plan. Under the Investment Plan, players have the option of having a
portion of their compensation for any given year placed into the Investment Plan before taxes are
withheld. The player can determine the amount to be placed into the Plan, subject to maximums set by the
Internal Revenue Service.
718
Generally speaking, if the player does not elect to place any money into the
Plan, an amount equal to the Internal Revenue Service maximum ($18,000 in 2016) will automatically be
placed into the Plan for the player.
719
Although the clubs are not obligated to contribute anything to the
Plan,
720
according to MLB, the clubs contribute millions of dollars each year to the players’ accounts.
721
Additionally, all players are fully vested in their accounts at all times.
722
The NFL also offers a 401(k)
plan.
2. Insurance Benefits
In 2016, MLB and the MLBPA agreed that players’ medical and dental benefits for players would be
“improved in a variety of areas.”
723
However, as discussed above, the specific ways in which the benefits
improvement is not yet publicly known. Thus, what follows is a summary of disability benefits prior to
the 2016 CBA negotiations.
Like the NFL’s Player Insurance Plan, MLB’s Benefit Plan provides players and their families with life
insurance, accidental death and dismemberment insurance, medical coverage, and dental coverage. A
player and his dependents become eligible for health insurance as soon as the player is listed on a club’s
40-man roster.
724
Disabled players and their dependents are also eligible for health insurance.
725
Additionally, former players may continue coverage through COBRA or by enrolling in the inactive
health benefits program.
726
In 2016, according to MLB, “MLB spent over $13 million to subsidize health
care for retired (inactive) MLB players.”
727
MLB expects this amount “to grow in the coming years.”
728
Both the active and inactive player health care programs cover hospitalizations, visits to physicians,
standard preventative care, and prescription drug costs through the use of preferred provider
organizations.
729
MLB’s Benefit Plan also provides some wellness benefits, including access to clinicians for mental health
and treatment for alcohol or drug abuse. However, the plan does not include other benefits included in the
NFL Player Insurance Plan, including child and parenting support services, elder care support services,
pet care services, legal services, and identity theft services.
3. Disability Benefits
Before a player is old enough to begin receiving a pension, he may be eligible for disability benefits under
the Pension Plan. In 2016, MLB and the MLBPA agreed that disability benefits for players would be
“improved.”
730
However, as discussed above, the specific amounts by which the benefits increased is not
yet publicly known. Thus, what follows is a summary of disability benefits prior to the 2016 CBA
negotiations.
Former players with at least four years of service who become totally and permanently disabled and all
active players who become totally and permanently disabled are eligible for disability benefits.
731
Disability payments range from $2,500 to $5,000 a month for the player and $300 to $600 for dependents,
depending on whether the player is active or inactive when he is disabled, the player’s salary the year
before his disability, and whether the player, if inactive, can show by clear and convincing evidence that
he became disabled as a result of his baseball career.
732
Players may receive a stabilizing disability
supplement if, once they begin receiving their pension, their pension is less than their disability
payment.
733
!
114!
MLB’s disability benefits are significantly less than those provided by the NFL. NFL benefits for total
and permanent disability range from $5,000 to $22,084 per month depending on the cause of the
disability. In addition, the NFL offers benefits for disabilities which are less than total and permanent
disabilities, and also offers neurocognitive disability benefits. MLB does not offer either of these benefits,
although there is likely much less of a need for neurocognitive disability benefits in MLB than in the
NFL.
4. Workers’ Compensation Benefits
Although not explicitly provided for in the CBA, MLB clubs, like NFL clubs, pay workers’ compensation
benefits to their players.
734
However, unlike the NFL, there is no provision in the MLB CBA that requires
clubs to provide comparable benefits in states where workers’ compensation coverage is not required.
Consequently, it appears that players in states that do not require coverage, like those for the Tampa Bay
Rays and Miami Marlins in Florida, are not automatically covered.
735
Nevertheless research suggests that
the clubs generally do choose to provide coverage.
5. Education-Related Benefits
MLB offers a “College Scholarship Plan” to its players.
736
As part of the 2016 CBA negotiations, the
parties agreed to “[i]mprovements to the College Scholarship Plan, particularly for players living outside
of the U.S.”
737
In October 2016, we asked MLB for more information about the College Scholarship
Plan, including the criteria for receiving benefits under the Plan and the actual benefits received under the
Plan. MLB responded only by directing us to the description of the College Scholarship Plan in the 2012
CBA, which does not clearly set forth the information we requested.
6. Joint Health-Specific Committees
MLB has a Safety and Health Advisory Committee (“SHAC”), comprised of representatives of both the
clubs and the MLBPA, to “deal with emergency safety and health problems” and to review player
working conditions.
738
The SHAC has advisory authority only,
739
but the parties have agreed to make
“every reasonable effort” to utilize the SHAC before pursuing safety- and health-related grievances
through the CBA’s arbitration procedures.
740
C. NBA Health-Related Benefits
As a preliminary matter, it is important to point out that in the NBA, like the NFL, the amounts paid to
players (current and former) in the form of benefits in most instances decreases the amounts available to
current players in salary.
741
1. Retirement Benefits
The NBA offers three retirement programs: (a) the Players’ Pension Plan; (b) the 401(k) Savings Plan;
and, (c) the Post-Career Income Plan.
742
a. Players’ Pension Plan
The NBA Players’ Pension Plan allows for full vesting rights after three years of service in the league,
743
the same vesting requirement as the NFL’s Retirement Plan for players who played after 1991. Players
can begin drawing their pension at age 45.
744
Under the 2017 CBA, beginning at age 50, the Pension Plan
pays players $572.13 per month for each year of credited NBA service,
745
with the possibility of annual
increases to that figure based on actuarial calculations.
746
According to the NBA, the pension benefits per
year of service are the same for all players that played after 1965, regardless of when they played. The
!
115!
NBA also indicated that players automatically receive Pension Plan payments if they do not file for them.
Lastly, the Pension Plan is funded by the clubs.
747
b. 401(k) Savings Plan
Under the 401(k) Savings Plan, players can contribute a portion of their salary, subject to the maximum
amounts permitted by the Internal Revenue Service ($18,000 in 2016
748
), into a 401(k) plan.
749
Clubs
match 140% of players’ allowed contributions.
750
This is similar to the NFL, which also offers a 401(k)
plan. However, NFL clubs contribute 200% of a player’s contribution. NBA players’ contributions are
automatic, unless the player affirmatively opts out.
c. Post-Career Income Plan
The Post-Career Income Plan (formerly called the Post-Employment Annuity Benefit Plan) is a retirement
plan that purchases annuities for players to provide a source of post-employment income.
751
To fund the
Plan, the NBA contributes 1% of Basketball Related Income,
752753
and players have the option of
contributing up to 10% of their post-tax income into the plan.
754
Annuities under the Plan are payable to a
player a year after his retirement from the NBA or six months after his 30th birthday, whichever is
later.
755
The benefit is paid in the form of installment payments until the player reaches 50 years old or a
joint life annuity paid over the player’s life and his surviving spouse’s life.
756
This is similar to the NFL,
which also offers an annuity plan.
2. Insurance Benefits
The NBA offers three different health insurance or benefit programs through a Voluntary Employees’
Beneficiary Association (“VEBA”): (a) a standard health insurance program; (b) a health reimbursement
account (“HRA Benefit”); and, (c) a Retiree Medical Plan. VEBAs, created pursuant to Section 501(c)(9)
of the Internal Revenue Code, traditionally provide “life, sick, accident, or similar benefits [for] members
or their dependents, or designated beneficiaries.”
757
The VEBA is described in the CBA as providing for
at least some of the benefits discussed in this Section, but its full scope is unclear. By comparison, the
NFL does not have a VEBA.
In addition, the 2017 CBA provides that the NBA and National Basketball Players Association (“NBPA”)
are to “meet and confer to discuss the establishment of a long-term care insurance benefit.”
758
In contrast,
the NFL already offers a long-term care insurance plan.
a. Health Insurance
The NBA provides players and their families with life insurance, accidental death and dismemberment
insurance, medical coverage, vision coverage, dental coverage, and prescription drug insurance
benefits.
759
The 2017 CBA also states that the parties will “establish a mental wellness program for
current players.”
760
The extent of the NBA’s intended mental wellness program is unclear, but, by
comparison, the NFL does offer a variety of wellness benefits, including: access to clinicians for mental
health, alcoholism, and substance abuse; child and parenting support services; elder care support services;
pet care services; legal services; and, identity theft services.
b. HRA Benefit
The HRA Benefit (formerly known as the Supplemental Medical Benefits Program) covers healthcare
costs not otherwise covered by players’ primary insurers, such as costs incurred in connection with the
payment of premiums for health insurance.
761
The benefit is available during players’ careers or after.

!
116!
HRA plans can help to pay out-of-pocket healthcare expenses after players’ careers have ended. The 2017
CBA provides for an HRA Benefit to be created for each player in the amount equal to “the lesser of: (A)
$30,000 and (B) the difference between $150,000 and the sum of all contributions previously made to
fund an HRA Benefit for such player in respect of prior Salary Cap Years… or, if such difference is $0 or
a negative number, then $0.”
762
However, the plan is only available to players who played in the NBA
during and/or after the 2000–01 season, and also appears limited to current players.
763
By comparison, the
NFL offers a health reimbursement account and Former Player Life Improvement Plan to help former
players with medical costs not covered by insurance.
Players who play for the Toronto Raptors are not eligible for the HRA Benefit for the period of time
during which the player is a resident of Canada (instead, they receive an alternative benefit).
764
c. Retiree Medical Plan
The 2017 CBA established medical benefits for former players for the first time.
765
According to the
NBPA, under the new program:
• Retired players with between three and six years of NBA service time
but who are not yet eligible for Medicare would be offered a plan that
includes medical, hospital, and prescription drug coverage with modest
out-of-pocket costs for deductibles and co-pays.
• Those with between seven and nine years of service who are not eligible
for Medicare would be offered the same coverage as the three-to-six-year
players with lower out-of-pocket costs.
• Retired players with at least 10 years of service who are not eligible for
Medicare would be offered the same coverage as the seven-to-nine-year
players, as well as coverage for their families.
• Retired players who are eligible for Medicare who have three to
nine years of service would be offered a $0 deductible and $0 co-pay
plan along with a low-cost prescription drug plan; those with 10+ years
of service would receive this coverage for themselves and their spouse.
766
According to the NBA, eligible former players are not required to pay any premiums for coverage for
themselves. The players can add their family to the insurance by paying premiums at varying amounts
depending on the player’s years of credited service.
767
3. Disability Benefits
NBA players are entitled to disability insurance benefits.
768
The CBA does not specify the benefit
amounts available to the players.
4. Workers’ Compensation Benefits
The 2017 NBA CBA provides that players are entitled to workers’ compensation benefits “in accordance
with applicable statutes.”
769
In reviewing this Report, the NBA explained that the CBA provision is meant
to indicate the clubs’ compliance with workers’ compensation statutes. In practice, the NBA operates a
league-wide workers’ compensation program in which all clubs are required to participate with two
!
117!
exceptions. The Cleveland Cavaliers and Toronto Raptors play in what are known as “monopolistic”
jurisdictions, Ohio and Ontario respectively, where employers are required to obtain workers’
compensation insurance from a state fund or qualify as a self-insurer. According to the NBA, the NBA’s
workers’ compensation program is long-standing but not negotiated with the NBPA. Thus, while
unlikely, the NBA could unilaterally decide to dissolve the program and clubs that play in states where
workers’ compensation is not required, such as Florida and Texas, would no longer be required to provide
workers’ compensation benefits to its players. Nevertheless, in current practice, all NBA players can
receive workers’ compensation benefits.
5. Education-Related Benefits
Beginning with the 2017 CBA, the VEBA provides for “reimbursement of eligible tuition and career
transition expenses.”
770
Players are entitled to a maximum reimbursement of $33,654 per year, and
$101,000 over their lifetime.
771
These benefits are available to players while playing and when their
playing career is over.
Similarly, the NFL’s Tuition Assistance Plan reimburses players for tuition, up to a maximum
reimbursement of $20,000 per year.
6. Joint Health-Specific Committees
The NBA and NBPA have a Labor-Management Cooperation and Education Trust (“Education Trust”).
While the Education Trust’s role is unclear, it seems that could address player health issues.
According to the CBA, the Education Trust is designed to provide “(i) health education programs and (ii)
education and career counseling programs designed to assist the NBA, NBA Teams and NBA players in
solving problems of mutual concern not susceptible to resolution within the collective bargaining process
and to enhance the involvement of NBA players in making decisions that affect their working lives.”
772
The 2017 CBA states that the parties will “meet and confer to discuss the Education Trust establishing a
modified financial education program.”
773
In addition to the Education Trust, there are other committees that have some health-related duties.
First, there is a Committee of Team Physicians with which NBPA representatives meet in order to discuss
“matters related to the medical care and treatment of players,”
774
but this group is not a joint committee in
and of itself and has limited authority of any kind under the CBA. The Committee of Team Physicians is
responsible for periodically reviewing the NBA’s Concussion Policy “in order to keep it current and
consistent with the evolving science of concussion management,”
775
and must consult with NBPA
representatives before making any changes to the Concussion Policy.
776777
Second, there is a Prohibited Substances Committee that consists of one NBA representative, one NBPA
representative, and three jointly selected representatives who are “experts in the field of testing and
treatment for drugs of abuse and performance-enhancing substances.”
778
The Prohibited Substances
Committee advises the NBA and NBPA on its anti-drug policy.
779
In contrast, the NFL’s Joint Committee and Accountability and Care Committee are principally focused
on player health and safety issues.
!
118!
D. NHL Health-Related Benefits
As a preliminary matter, it is important to point out that in the NHL, like the NFL and NBA, the amounts
paid to players (current and former) in the form of benefits decreases the amounts available to current
players in salary.
780
1. Retirement Benefits
The NHL has two retirement plans available to its players: (1) the Retirement Plan, which is a defined
benefit plan; and, (2) a 401(k) plan.
The NHL’s Retirement Plan provides pension payments to players beginning on their 62nd birthday,
except the player may receive actuarially equivalent
781
pension benefits as early as one month after his
45th birthday.
782
A player becomes eligible for participation in the Retirement Plan as of the date of his
first NHL regular season game,
783
and he accrues fractional credited service
784
for each regular season
game during which he is on a club’s roster.
785
The NHL contributes $38 million each year to fund the
Retirement Plan.
786
The application of the NHL’s Retirement Plan to players who played prior to the 2013
CBA is unclear.
To determine the pension payment amounts, the NHL uses a player with ten years of credited service as
its baseline. A player with ten or more years of credited service is eligible to receive the maximum
pension payment permitted under the Internal Revenue Code, which was $210,000 in 2016
787
($17,500/month). A player with less than ten years of credited service will receive a proportional share of
the maximum payment permitted.
788
Thus, if a player played only seven years, he would be eligible to
receive pension payments up to 70% of $210,000 ($147,000).
It is unclear whether players automatically receive Retirement Plan payments or if they must file for
them.
In addition to the Retirement Plan, as part of the 2005 CBA, the NHL and NHLPA established the Fund
for Senior Retired Players.
789
The Fund provides money to approximately 350 former players over the age
of 65 or their widows depending on how many seasons the player played.
790
Both the NHL and NHLPA
contribute $3 million annually toward the Fund.
791
We turn now to the NHL’s 401(k) plan. The 401(k) plan was created as part of the 2012 CBA, replacing a
prior pension plan. A 401(k) plan is a retirement plan created pursuant to section 401(k) of the United
States Internal Revenue Code. There are, however, seven Canadian clubs in the NHL for whom the
United States Internal Revenue Code would not apply. Nevertheless, Canadian tax law does provide for a
retirement plan substantially similar to an American 401(k). Consequently, the NHL has two separate
401(k)-type plans—one for players on American clubs, and one for players on Canadian clubs. To avoid
confusion, for our purposes here, we refer to both of these plans as the NHL’s 401(k) plan.
The 401(k) plan allows players to contribute pre-tax and post-tax portions of their pay into an investment
account up to the limits set by the IRS. In 2016, the maximum pre-tax contribution was $18,000 and the
maximum post-tax contribution was $53,000.
792
While clubs formerly contributed to the old pension plan,
the new 401(k) plan is funded entirely by the players. Additionally, players must voluntarily enroll in the
plan. In contrast, under the NFL’s 401(k) plan, clubs contribute $2 for every $1 contributed by a player
and players are automatically enrolled in the plan.
!
119!
2. Insurance Benefits
The NHL provides insurance benefits for players that include medical coverage, dental coverage, life
insurance, and accidental death insurance.
793
While not a part of its insurance coverage, the NHL, through
its Substance Abuse and Behavioral Health Program, offers players substance abuse and mental health
treatment free of charge. This program is discussed further in Chapter 4: Drug and Performance-
Enhancing Drug Policies. However, there is no indication that the NHL offers other wellness benefits
provided by the NFL, including: child and parenting support services, elder care support services, pet care
services, legal services, and, identity theft services.
Former players who played at least 160 games in the NHL can continue to receive the above benefits for
life provided they apply for coverage within 120 days of the date the player was last covered under the
plan.
794
The former players have to contribute to the costs of their health insurance in amounts that had
not yet been agreed upon in the 2013 CBA.
795
In contrast, former NFL players are only entitled to health
insurance for five years after they are done playing. Finally, for Canadian residents, the health insurance
plan provides coverage for treatment that is not covered by the player’s provincial Canadian health
plan.
796
3. Disability Benefits
The NHL offers a variety of disability benefits.
First, under the Retirement Plan, a player who has at least five years of credited service and becomes
totally and permanently disabled is entitled “to receive disability pension benefits from the Retirement
Plan equal to the value of his accrued pension benefits, actuarially reduced to the age of
commencement.”
797
Second, the NHL provides a “career ending disability policy” providing for a one-time benefit, subject to
the player signing a release, ranging in amount from $200,000 to $1,000,000.
798
To obtain the payment,
the player must release “the Club, the League, the NHLPA, all other Clubs, the insurance carrier, and the
servants, employees, officers and agents of each of the above from any and every additional obligation,
liability, claim or demand[.]”
799
The NFL’s Neurocognitive Disability Benefit also requires players to
execute a release of liability. The NFL’s disability benefits differ in that they are paid monthly, rather
than in a lump sum.
Third, the NHL offers a “serious disability policy” that provides a one-time benefit for the player in the
event he suffers a serious disability, contingent on execution of the above-described release.
800
Table 3-H
below lists the potential serious disabilities and the related benefit amounts:
Table 3-H: NHL Serious Disability Benefits
Disability
Benefit Amount
Loss of Brain Function
$5,000,000
Paralysis
$5,000,000
Organ Failure
$3,000,000
Diagnosis of Terminal Illness
$3,000,000
Loss of a Limb*
$2,500,000
Loss of Two (2) Limbs*
$4,000,000
Loss of Sight in Both Eyes
$4,000,000
Loss of Sight in One (1) Eye
$2,000,000
Loss of Hearing or Speech
$750,000
Loss of Hearing and Speech
$1,000,000

!
120!
Loss of One Hand or One Foot*
$750,000
Loss of Both Hands or Both Feet or One Hand and One Foot*
$1,000,000
* Loss includes loss of use.
There is an important difference between the disability benefits offered by the NFL and the NHL. NHL
disability benefits are only available to players currently on a club’s roster.
801
In contrast, NFL players can
and generally do apply for disability benefits after their career has ended. In particular, the NFL offers
several neurocognitive disability benefits to former players, while the NHL only provides disability
payments for loss of brain function if the player is currently playing.
4. Workers’ Compensation Benefits
NHL players are entitled to workers’ compensation benefits.
802
In addition, like the NFL CBA, the NHL
CBA requires clubs located in states where workers’ compensation coverage is not required for
professional athletes to provide equivalent benefits to the players.
803
Thus, players for the Tampa Bay
Lightning and Florida Panthers are able to receive workers’ compensation benefits despite the fact that
Florida does not require employers to obtain workers’ compensation coverage.
5. Education-Related Benefits
The CBA contemplates the creation or expansion of education-related benefits. Although there is no
formal program, the 2011 CBA states that “[t]he League and the NHLPA shall work together on
developing and improving career counseling and continuing education programs[.]”
804
Indeed, in 2015,
the NHL and NHLPA announced plans to launch a program that would pay for players’ tuition at colleges
and trade schools.
805
The NHL and NHLPA each have committed approximately $1.5 million to the
program, which will begin with current players and hopes to expand to former players.
806
6. Joint Health-Specific Committees
The NHL and NHLPA have formed the Joint Health and Safety Committee, which consists of five
members from each side.
807
The Committee is responsible for “mak[ing] recommendations to the NHL
and the NHLPA for consideration and approval regarding all issues related to Player health and regarding
the safety of the playing environment.”
808
To do so, the Committee is empowered to create working
groups and subcommittees as necessary.
809
The Committee is also responsible for resolving issues
concerning whether club doctors have violated their obligations to the players,
810
monitoring the
electronic medical record system,
811
and creating a list of second opinion doctors.
812
E. CFL Health-Related Benefits
1. Retirement Benefits
The CFL provides a pension plan for players. The CFL pension plan is a defined contribution plan, with
clubs and players paying matching amounts.
813
In 2016, for example, each parties contributed $3,900
(CAD).
814
However, clubs will only contribute the amounts for players who are on the club’s roster for
nine or more games in that season.
815
As a defined benefit plan, the players seemingly are vested in the
pension plan as soon as any money is contributed to their account.
2. Insurance Benefits
The CFL medical plan provides medical coverage,
816
life insurance, and accidental death and
dismemberment insurance coverage.
817
Dental benefits are not included in the medical plan but a “Benefit
!
121!
Plan Advisory Committee may agree to change the benefits, including the addition of dental coverage and
disability” if there is sufficient surplus from the amounts paid by the clubs.
818
In contrast, the NFL provides dental benefits as well as a variety of wellness benefits, including access to
clinicians for mental health, alcoholism, and substance abuse; child and parenting support services; elder
care support services; pet care services; legal services; and, identity theft services.
Also unlike the NFL, the CFL offers no health insurance benefits for former players. However, as long as
the players are residents of Canada, they can obtain healthcare through government-sponsored plans.
3. Disability Benefits
As explained above, disability benefits are not guaranteed under the CFL CBA, but are possible if funding
exists. In contrast, the NFL provides many different types of disability benefits for current and former
players.
4. Workers’ Compensation Benefits
Some provincial statutes prohibit professional athletes, such as CFL players, from receiving workers’
compensation benefits.
819
However, in 2016, the CFLPA submitted an application for players to be
eligible for workers’ compensation benefits in the province of Alberta,
820
where two CFL clubs play. If
successful, the CFLPA reportedly plans to try and expand coverage for workers’ compensation benefits to
other provinces.
821
By contrast, although workers’ compensation payments have been a controversial
issue, all NFL players are currently entitled to such benefits.
5. Education-Related Benefits
The CFL does not offer any education-related benefits, unlike the NFL’s Tuition Assistance Plan.
6. Joint Health-Specific Committees
The CFL and CFLPA have a Joint Committee on Players’ Safety and Welfare.
822
The Committee’s
purpose is to discuss player safety and welfare aspects of playing equipment, playing surfaces, stadium
facilities, playing rules, player-coach relationships, drug abuse prevention programs, and any other
relevant subjects.
823
Any proposed change in a playing rule must be referred to the Committee for
consideration and a recommendation.
824
However, the Committee has no authority to bind either the CFL
or CFLPA on any issue.
825
F. MLS Health-Related Benefits
1. Retirement Benefits
MLS offers a 401(k) plan to its players.
826
Regardless of whether a player contributes, MLS makes
employer contributions equivalent to 3.75% of a player’s base salary.
827
Contributions vest
immediately.
828
2. Insurance Benefits
MLS provides players and their family members with medical insurance, dental insurance, and life
insurance.
829
!
122!
In contrast, the NFL provides a variety of wellness benefits, including access to clinicians for mental
health, alcoholism, and substance abuse; child and parenting support services; elder care support services;
pet care services; legal services; and, identity theft services.
Also unlike the NFL, MLS offers no health insurance benefits for former players.
3. Disability Benefits
MLS does provide long-term disability insurance for its players equivalent to 60% of a player’s salary,
with a monthly maximum benefit of $10,000.
830
The monthly maximum benefit is the same in the 2015
CBA as it was in the 2004 CBA.
831
4. Workers’ Compensation Benefits
MLS players are entitled to workers’ compensation benefits.
832
Additionally, like the NFL and NHL,
MLS clubs that are in states that are not required to provide workers’ compensation benefits are required
to provide equivalent benefits.
833
Thus, players on Orlando City FC are able to obtain the equivalent of
workers’ compensation benefits when they otherwise would have been denied coverage because Florida
does not require employers to provide workers’ compensation benefits. Alternatively, MLS and the
MLSPU have agreed that players can file for benefits in New York state, regardless of where they play.
834
In other words, MLS will not challenge the jurisdiction of the claim.
835
5. Education-Related Benefits
MLS does not offer any league-wide education-related benefits. However, for players who participate in
the Generation adidas program, an initiative designed to grow domestic talent, players can leave college
early and money is placed in escrow for them to complete their college education at a later date.
836
Nevertheless, this benefit is available only to a select group of the most highly-skilled young players—it
is not a league-wide benefit to all players like the NFL’s Tuition Assistance Plan.
6. Joint Health-Specific Committees
MLS has a Health and Safety Committee, which includes one MLSPU representative, that is responsible
for making “recommendations to the Commissioner concerning health and safety procedures and
protocols.”
837
G. Analysis
While we provide an analysis that compares the leagues on the benefits they provide players, it is worth
emphasizing at least two reasons why this is not a full apples-to-apples comparison. First, the mean
number of seasons of play varies across the leagues,
838
such that in some leagues fewer individuals will
make the milestones necessary for vesting or activation of some benefits. Second, while we lack complete
data on the health risks of playing each of the sports, from what we do know the risks associated with
each sport are heterogeneous in at least some respects, such that the need for health insurance and
disability benefits varies from league to league.
With that caveat, Table 3-I provides a comparison of the leagues’ benefits while Tables 3-J and 3-K
provide a comparison of monthly payments under the Big Four leagues’ retirement/pension plans in two
different scenarios.
!
123!
Table 3-I: Comparison of Leagues’ Benefits
Benefit
NFL
MLB
NBA
NHL
CFL
MLS
Pension Plan
Yes
Yes
Yes
Yes
Yes
No
Pension Plan
Vesting
Requirement
3 years (post
1992)
1 day
3 years
1 day
9 games
NA
Severance Plan
Yes
No
No
No
No
No
401k Plan
Yes
Yes
Yes
Yes
No
Yes
Other Deferred
Compensation Plan
Yes
No
Yes
No
No
No
Health Insurance
(Current Players)
Yes
Yes
Yes
Yes
Yes
Yes
Health Insurance
(Former Players,
other than COBRA)
5 years
For life
potentially
For life
potentiall
y
For life
potentially
No
No
Life Insurance
Yes
Yes
Yes
Yes
Yes
Yes
Dental Insurance
Yes
Yes
Yes
Yes
Maybe
Yes
Health
Reimbursement
Account
Yes
No
Yes
No
No
No
Long Term Care
Insurance
Yes
No
Potentiall
y
No
No
No
Wellness Benefits
Many
Some
Some
None
None
None
Disability Benefits
(Current Players)
Yes
Yes
Yes
Yes
Maybe
Yes
Disability Benefits
(Former Players)
Yes
Yes
No
No
No
No
Neurocognitive
Disability Benefits
Yes
No
No
Only for
current
players
No
No
Workers’
Compensation
Yes
Partial
Yes
Yes
Prohibit
ed by
law
Yes
Education-Related
Benefits
Yes
No
Yes
Yes
No
For some
players
Joint Health-
Specific
Committee(s)
Yes
Yes
Yes
Yes
Yes
Yes
In examining the projected monthly payouts under the Big Four Leagues’ retirement/pension plans, we
caution that the plans are complicated and involve many different variables to determine what a former
player’s monthly payment will be, including but not limited to the player’s current income and cost of
living adjustments. In Tables 3-J and 3-K below, we try to provide a picture of the type of retirement
benefits available to players in each of the leagues. For this analysis, we chose the age of 62 for the age at
which the retired player would begin to receive benefits because in the NHL this is the earliest age at
which a player can receive retirement benefits. Then, we chose to analyze players who last played in 2000
and 2015 to provide a spectrum of how the benefits change depending on when the player last played.
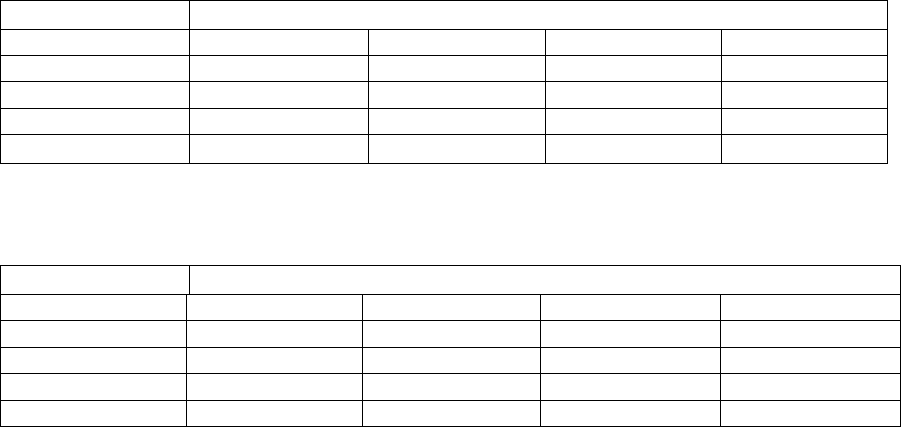
!
124!
Table 3-J: Projected Monthly Payments under the Big Four Leagues’ Retirement Plans (Last
Played in 2000 and Will Take Retirement Benefits at Age 62)
Experience
League
1 Year
3 Years
5 Years
10 Years
NFL
$470
$1,410
$2,090
$3,661
MLB
$1,666
$5,000
$8,333
$16,666
NBA
839
$1,792
$5,375
$8,958
$17,917
NHL
Uncertain
840
Table 3-K: Projected Monthly Payments under the Big Four Leagues’ Retirement Plans (Last
Played in 2015 and Will Take Retirement Benefits at Age 62)
Experience
League
1 Year
3 Years
5 Years
10 Years
NFL
$470
$1,720
$2,810
$5,160
MLB
$1,666
$5,000
$8,333
$16,666
NBA
$1,792
$5,375
$8,958
$17,917
NHL
$1,750
$5,250
$8,750
$17,500
According to the NFLPA, NFL players have “the very best benefits package in professional sports.”
841
This claim seems substantially true. First, the NFL offers every benefit that is provided by any of the
other leagues. Second, the NFL offers several benefits that are not provided by any of the other leagues,
including severance pay, long term care insurance, the Former Player Life Improvement Plan, and
neurocognitive disability benefits for former players. Third, there are several benefits that only the NFL
and a limited number of the other leagues provide: (a) only the NFL, MLB, NBA, and NHL provide
health insurance (beyond COBRA) for former players; (b) only the NFL, MLB, and NBA provide players
with mental health and substance abuse treatment; (c) only the NFL and NBA offer a health
reimbursement account; (d) only the NFL and MLB offer disability benefits to former players; (e) only
the NFL and NBA offer education-related benefits for all players; and, (f) only the NFL, NBA, NHL, and
MLS guarantee workers’ compensation benefits to all of their players.
While overall the NFL thus appears to be the best league for benefits, comparing the leagues’ benefit
offerings is challenging and not without judgment calls. For example, considering the NFL’s higher
injury rates (see Chapter 2: Injury Rates and Policies), it seems appropriate that NFL players would be
entitled to more benefits, such as the NFL’s Long Term Care Insurance Plan and Former Player Life
Improvement Plan. In particular, given the disparities in concussion rates, neurocognitive disability
benefits are likely appropriate in the NFL but may not be needed in some of the other leagues. Moreover,
we have identified three areas in which the NFL might learn lessons for improvement from one or more
of the other leagues.
First, the NFL’s health insurance options for former players appear to be less favorable than those offered
by MLB, the NBA and the NHL. Currently, for players who have vested under the Retirement Plan
(which requires at least three years of Credited Service for players after 1992), the NFL provides the same
health insurance as available to current players for five additional years or the former player can also
obtain health insurance via COBRA. However, COBRA is designed to be a temporary solution and is
generally regarded as expensive relative to other health insurance plans.
842
In contrast, MLB’s Benefit
Plan provides former players the option to continue (or obtain) the same health insurance benefits as
current players for life. While former MLB players have to pay more for their health insurance than
current MLB players, presumably the plans offered are cheaper than COBRA coverage or else the players
!
125!
would have opted for COBRA coverage. Similarly, the NBA’s Retiree Medical Plan is available to
former players for life free of charge and the NHL allows former players who played at least 160 games
to continue with the NHL’s insurance plan for life.
843
The NFL does offer a variety of health benefits that might partially fill the gap for former players,
including health reimbursement accounts, long term care insurance, benefits for uninsured former players,
and disability benefits. Nevertheless, players often have to go through a difficult process to obtain some
of these benefits after they have already had to pay for the care, or care is delayed until they can obtain
the benefits. We believe there may be advantages to allowing former players to continue to obtain some
form of the same health insurance that they were able to receive while playing – ensuring, among other
things, that they can remain in the same network of doctors.
Second, as shown in Tables 3-J and 3-K, the monthly payments to former NFL players under the
Retirement Plan are seemingly the smallest payments of the Big Four leagues. Nevertheless, when all of
the benefits available to former players are packaged together, it is likely that the NFL’s benefits are the
most valuable due to the number of benefits that are available. Consequently, lower Retirement Plan
payments might simply reflect the NFLPA’s preferred allocation of total benefits, i.e., a shifting of the
value of benefits away from the Retirement Plan and to other benefits instead. As with health insurance
benefits, the NFL’s Retirement Plan payments require players to undertake relatively little administrative
work to receive and they are a more secure and stable income source and benefit than some of the other
benefits made available by the NFL. Nevertheless, some might believe it is a better use of player benefit
money to fund benefits and programs for former players who are disabled or impaired in some way as
opposed to providing larger Retirement Plan payments to all eligible former players. All the benefits
available to NFL players must be viewed collectively. For these reasons, as discussed in the
Recommendation, we recommend the NFL consider whether the current allocation of player benefits is
the preferred, most just, and most effective allocation.
Third, MLB and NHL players are vested in their pension plans on the first day they play in those leagues.
By comparison, the NFL requires players to accrue three years of experience (or more depending on when
they played), before they are eligible for retirement benefits (as well as many other benefits). The mean
career of NFL and MLB players are both around five years long.
844
Yet, the NFL’s Retirement Plan likely
excludes and has excluded thousands of former players who did not earn three Credited Seasons. It is
unclear why the NFL requires three years of service (the NBA does as well). The minimum service time
clearly reduces costs of the Retirement Plan, but might also reflect a policy decision as to when an NFL
player has sufficiently contributed to the NFL to deserve pay under the Retirement Plan. Below, we make
a recommendation concerning the vesting requirement for the NFL’s Retirement Plan.
In addition to the above-described potential deficiencies, there is another issue worthy of comment. To
obtain Neurocognitive Disability Benefits after their career is over, the NFL requires players to execute a
release releasing the NFL and clubs from any liability for head or brain injuries when they apply for the
benefits. Similarly, the NHL requires players to release the NHL, clubs, and a variety of other parties for
players to obtain career-ending disability insurance benefits. It could be argued that these releases unfairly
condition benefits to which players are entitled on the relinquishment of their legal rights. On the other
hand, the releases could be seen to ensure players do not seek more benefits than those to which they are
entitled and to prevent litigation. As there are persuasive points for and against the releases, we do not
make a recommendation concerning them. Instead, we merely highlight the issue for potential future
consideration by the leagues, unions, and others.
!
126!
H. Recommendation
Recommendation 3-A: The NFL and NFLPA should consider whether change is necessary concerning
player benefit plans.
As discussed above, we identified three potential areas of concern regarding the benefit plans offered by
the NFL. Also as discussed above, the benefits available to NFL players must be viewed in the context of
one another: increasing one benefit might mean a decrease in another benefit. Below, we identify and
discuss possible changes to the benefit plans, the implementation of which must be weighed collectively.
• The NFL and NFLPA should consider providing former players with health insurance
options that meet the needs of the former player population for life: While the NFL provides
significant benefits to former players, players likely do not take full advantage of those benefits
due to the associated administrative burdens.
845
Additionally, a consistent and reliable health
insurance plan seems preferable to ad hoc and uncertain benefits. The NFL and NFLPA should
consider whether it would be more appropriate to shift some of the value of benefits away from
the unplanned benefits (e.g., disability benefits and the health reimbursement account) to more
stable health insurance options.
846
Where players have only played one or two seasons (and
perhaps games), there might be questions as to whether it is appropriate to provide lifetime health
insurance to someone who was employed for such a short period of time. On the other hand, only
a few games or seasons can have life-lasting effects on a player. One option worth considering is
tiering health insurance benefits and allowing those with less Credited Seasons to qualify for
some but not full benefits.
• The NFL and NFLPA should consider increasing the amounts available to former players
under the Retirement Plan: The monthly retirement benefits represent a more stable benefit
than the other valuable but still uncertain benefits. Consequently, the NFL and NFLPA should
consider whether it would be more beneficial to shift some of the value of benefits away from the
unplanned benefits to the more stable Retirement Plan monthly payments.
• The NFL and NFLPA should consider reducing the vesting requirement for the Retirement
Plan: The purpose of the NFL’s three-year vesting requirement is unclear. The vesting
requirement results in a considerable portion of former players being unable to collect any
retirement benefits. We acknowledge that there may be appropriate policy reasons for such a
limitation, such as a determination as to when a player has sufficiently contributed to the NFL.
Indeed, many employers require a certain number of years of service before accruing certain
benefits.
847
If the vesting requirement is instead principally motivated by cost, then the
distribution of benefits among former players should be reconsidered to determine what is
maximally beneficial for player health. In other words, is the current distribution of benefits
among former players, which largely excludes players with less than three years of experience,
preferred by the NFL, NFLPA, and players, or would it be preferable to reduce the benefits to
players with more than three years of experience to provide some benefits to those with less than
three years of experience? While these considerations are not easy and require a delicate balance,
the exclusion of a significant portion of former players from the Retirement Plan requires an
examination of the vesting requirement. As with health insurance benefits, one option worth
considering is tiering Retirement Plan benefits and allowing those who have played less than
three Credited Seasons to qualify for some if not full benefits.

!
127!
CHAPTER 4: DRUG AND PERFORMANCE-ENHANCING SUBSTANCE POLICIES
This Chapter summarizes the policies of each of the leagues concerning performance-enhancing
substances (“PES”) and drugs of abuse. As explained below, the leagues differ at times in their
categorizations and treatments of different drugs and substances. Where appropriate, we will separate our
analysis of the leagues’ policies by PES and drugs of abuse, but will collectively refer to the policies as
the leagues’ “drug policies.”
Before analyzing the leagues’ drug policies, there are a few concepts and issues that need to be discussed,
including what is meant by a “PES” and a “drug of abuse”; the unique case of marijuana; the purpose for
the drug policies; therapeutic use exemptions; and, the role of unions in drug policies.
Meanings of PES and Drugs of Abuse
The leagues generally do not provide an overarching definition for PES but instead ban a long list of
substances that have the potential to enhance a player’s performance in ways that the league, sports
community, and/or medical community has determined to be unfair, unnatural, and/or unsafe.
848
As will
be shown below, PES are also sometimes referred to as “performance-enhancing drugs” (“PEDs”). This
term is slightly outdated as the term PES now better captures a wider variety of substances that athletes
might try to use to enhance their performance.
Drugs of abuse is a term generally used by the leagues in reference to illegal substances that do not have
the potential to enhance a player’s performance and which present serious health concerns. For example,
MLB defines “drugs of abuse” to include marijuana, synthetic marijuana, cocaine, LSD, opiates, MDMA,
GHB, and PCP.
849
Similarly, the NFL defines “substances of abuse” as all illegal drugs, including but not
limited to, marijuana, cocaine, opiates, MDMA, and PCP.
850
Legal substances, including alcohol and
prescription medications, can also fall within the purview of the leagues’ drugs of abuse policies if
abused, as will be discussed below.
Finally, we use the terms “substance” and “drug” interchangeably. While they are not exactly analogous
terms, the terms are often used interchangeably in the context of professional sports and thus serve our
purposes here.
Marijuana
Before we get into the details of the various policies it is worthwhile to discuss the special case of
marijuana, which we also generally include in the category of drugs of abuse. Marijuana is banned under
federal law and is listed as a Schedule I controlled substance under the Controlled Substances Act, thus
classifying it as a substance which, according to the Act, “has a high potential for abuse” and “has no
currently accepted medical use[.]”
851
Nevertheless, as of February 2017, 29 states have approved
marijuana for medical use, and seven states (Alaska, Colorado, Massachusetts, Maine, Nevada, Oregon,
and Washington) and the District of Columbia have approved it for recreational use in certain
amounts.
852853
Moreover, there is a robust debate about what, if any, are the health and social
consequences of marijuana use.
854
Thus, the argument exists that marijuana should be treated differently
from other “drugs of abuse.”
Some of the leagues have explicitly recognized the uniqueness of marijuana. As will be shown below, the
NFL and NBA treat marijuana differently, and the NBA does not classify marijuana as a drug of abuse.
Moreover, some believe marijuana use is common among NFL players to help manage pain.
855
Amidst at
least some evidence that marijuana can be an effective pain management tool,
856
in 2016, the NFLPA
announced that it would study the issue.
857
Nevertheless, the NFL has insisted that the legalization of
!
128!
marijuana in certain states (including those that are home to NFL clubs), does not change the NFL’s
position—a policy banning marijuana.
858
However, the NFL has stated that it is willing to consider
medically appropriate uses of marijuana, such as for pain management and treatment of concussions, if
recommended by medical experts.
859
Purpose of Drug Policies
The case of marijuana raises the question about why certain drugs are banned, under either a PES or drugs
of abuse policy. A list of reasons why specific drugs might be banned includes: (1) the drugs are
associated with negative health consequences; (2) the drugs are illegal; and/or, (3) the drugs provide the
player with an unfair competitive advantage.
860
Many drugs meet one or more of these criteria. The criteria most closely related with the particular drug
generally determine whether the drug is banned under a PES policy or a drugs of abuse policy. Drugs that
provide an unfair competitive advantage would generally be those classified as a PES while illegal drugs
would generally be considered drugs of abuse. Nevertheless, many PES are also illegal (or obtainable
only with a prescription) and some illegal drugs of abuse can provide a competitive advantage (such as
stimulants). Our analysis is focused on the health consequences of drug use rather than competitive
advantage issues.
Finally, the health consequences of many of the drugs are a constant subject of debate and ongoing
scientific assessment. Whether the positive purposes and effects of certain drugs sufficiently outweigh the
negative consequences is a medical determination and beyond the scope of this Report, but this question
does relate to the purpose of therapeutic use exemptions, an issue to which we now turn.
Therapeutic Use Exemptions
Some prohibited substances might be appropriate or necessary for the treatment of specific medical
conditions. Consequently, sports leagues generally permit what are known as therapeutic use exemptions
(“TUEs”), that permit the player to use a banned substance without violating a drug policy. A good
example of a TUE is the case of American Olympic sailor Kevin Hall. As a result of cancer, Hall needed
testosterone injections to maintain normal levels of the hormone.
861
Hall received a TUE to take
testosterone (normally a banned substance) so that he could participate in the 2004 Olympics.
862863
The availability of TUEs also raises the prospect of players seeking them more for performance-
enhancing purposes as opposed to medical. In 2006, MLB began to test for stimulants, a banned
substance but one nonetheless long considered to be commonly used in MLB.
864
In 2006, 28 players
obtained a TUE for stimulants used to treat attention-deficit disorder (“ADD”), such as Adderall or
Ritalin.
865
The next year, 103 players obtained TUEs for ADD drugs, raising concerns that the TUE
process was being abused.
866
Nevertheless, the prevalence of TUEs for ADD drugs has remained fairly
consistent: 119 in 2013; 112 in 2014;
867
111 in 2015,
868
and 105 in 2016.
869
Approximately 1,375 players
played in a MLB regular season game in 2016.
870
Thus, an estimated 7.6% of them had a TUE for ADD
drugs.
871
Role of Unions
Each of the leagues’ drug policies is the result of collective bargaining with the leagues’ respective
players unions. Indeed, drug testing is generally considered a mandatory subject of bargaining between
employers and a union pursuant to the National Labor Relations Act.
872
The union will look to protect the
players’ rights and interests in all respects when negotiating the drug policy, but what that means is not
always clear.
!
129!
Players have heterogeneous views concerning the most desirable drug policy. When it comes to drugs of
abuse, some players likely do not want any testing out of concerns for their privacy or so that they can
engage in drug-related behavior off of the field. Other players might be concerned with the adverse health
and legal consequences associated with drugs of abuse and instead want robust testing. Similarly, some
players intentionally take PES to try to improve their performance and thus would like to see minimal
testing and discipline for their use. Conversely, some players believe that PES undermine the integrity
and fairness of the game and should be subject to frequent testing and harsh punishment.
Regardless of the players’ and unions’ balancing of these views, the unions always work to protect a
player’s legal and procedural rights. A drug test can be an invasive and personal process. Drug tests are
conducted via the collection of either urine or blood. Urine specimen collection requires a player to be
naked from his knees up and then urinate into a cup with the specimen collector standing directly in front
of him.
873
Blood tests require blood to be withdrawn. Consequently, players and their unions generally
seek to minimize the number of times players have to go through these uncomfortable experiences.
Additionally, the unions want to ensure that the drug tests are reliable in that testing procedures accurately
determine whether a player has failed a drug test. In the 2011 CBA, the NFL and NFLPA agreed that the
NFL would begin to test for human growth hormone (“hGH”), with the specifics to be worked out at a
later date. Nevertheless, it took nearly three years for the NFL and NFLPA to agree on the procedures of
hGH testing due, in part, to concerns about the scientific reliability of the blood tests available at the
time.
874
Another procedural concern of the unions is “non-analytical positives,” i.e., those situations where the
player has not tested positive for a banned substance but has violated a drug policy in some other way,
such as by possessing the drug, engaging in illegal conduct, manipulating the test, or being accused of
having used a banned substance through the testimony of others. Without clear proof that a player has
taken a banned substance (such as through a failed drug test), the unions want to ensure that players are
not unfairly punished for circumstantial evidence.
Finally, unions want to ensure that players receive a fair appeals process, typically understood to include
the right to challenge the validity of the alleged drug policy violation before a neutral arbitrator. The
appeals process and a player’s legal rights thereunder are important issues for players. Nevertheless, they
are legally complicated and more tangential to player health than is our focus in this Report.
Consequently, we do not discuss them here.
***
With this background, we turn to our analysis of the leagues’ drug policies. Specifically, for each of the
leagues, we will describe: (1) the substances prohibited; (2) the types of tests and prohibited conduct; (3)
the number of tests; (4) the administration of the policies; (5) therapeutic use; (6) discipline; (7) treatment;
and, (8) confidentiality.
A. The NFL’s Drug Policies
The NFL has two separate policies: (1) the Policy on Performance-Enhancing Substances (“PES Policy”);
and, (2) the Policy and Program on Substances of Abuse (“Substance Abuse Policy”). Both policies were
most recently amended in 2016. We will describe both policies for each issue of interest.
!
130!
1. Substances Prohibited
a. PES Policy
The PES Policy prohibits specifically listed substances in the following categories: (1) anabolic agents,
including anabolic/androgenic steroids, hormones (including hGH), Beta-2-agonists, anti-estrogenic
agents, and selective androgen receptor modulators (“SARMs”); (2) masking agents, including diuretics,
epitestosterone, and probenecid; and (3) stimulants.
875
Doping methods, including enhancement of oxygen
transfer, chemical and physical manipulation, and gene doping are also all strictly prohibited.
876
The NFL
and NFLPA may mutually agree to modify the prohibited substances list included in the PES Policy.
877
b. Substance Abuse Policy
The Substance Abuse Policy prohibits players “from the illegal use, possession, or distribution of drugs,
including but not limited to cocaine; marijuana;
878
opiates and opioids; methylenedioxymethamphetamine
(MDMA); and phencyclidine (PCP),” as well as the “abuse of prescription drugs, over-the-counter drugs,
and alcohol.”
879
Other substances not enumerated may be prohibited if included in a treatment plan
required by the Substance Abuse Policy (explained further below).
880
An important change concerning certain stimulants was made to the PES Policy and Substance Abuse
Policy in 2014. Prior to 2014, several players tested positive for banned stimulants during the off-
season.
881
Stimulants were banned under the PES Policy but provided the players no competitive
advantage during the off-season. Instead, the players were using the stimulants as recreational drugs.
882
Under the revised PES Policy, if a player tests positive for a stimulant during the off-season, he is deemed
to have violated the Substance Abuse Policy and not the PES Policy.
883
The change is dramatic in terms of
the discipline to be imposed: four games for a first violation of the PES Policy versus no punishment
under the Substance Abuse Policy, as will be explained below.
2. Types of Tests and Prohibited Conduct
a. PES Policy
The PES Policy uses urine and blood tests.
884
A test is “positive” under the PES Policy if the test result reveals the presence of a prohibited substance in
the player’s sample “at the level required by the testing protocols.”
885
Players are also subject to
punishment under the PES Policy for: (1) violations of law (demonstrated by convictions or player
admissions) relating to the use, possession, acquisition, sale, or distribution of steroids, growth hormones,
stimulants, or related substances, or conspiring to do so;
886
(2) using, possessing, or distributing PES as
found through credible evidence;
887
(3) attempting to substitute, dilute, or adulterate a specimen;
888
and,
(4) manipulating a test result.
889
While violations of law, non-analytical positives, attempts to substitute,
dilute, or adulterate specimens, and test result manipulations are not expressly included in the definition
of a “positive test,” they are subject to discipline as will be explained below.
b. Substance Abuse Policy
The Substance Abuse Policy uses urine tests only.
890
For the Substance Abuse Policy, “[t]ests… will be deemed positive if they are confirmed by laboratory
analysis at the identified urine concentration levels.”
891
A player who fails to cooperate fully in the testing
process or who attempts to substitute or adulterate a specimen, alter a test result, or engage in doping
!
131!
methods will be treated as if he produced a positive test.
892
Players who fail to appear for testing are
subject to discipline, but not on the same schedule as those whose specimens result in positive tests.
893
A player also violates the Substance Abuse Policy if he commits a violation of law involving alcohol or
drugs of abuse.
894
In addition to a conviction, a violation of law will also be found where the player enters
into a diversionary program, deferred adjudication, disposition of supervision, or similar arrangement,
including nolo contendere pleas.
895
3. Number of Tests
a. PES Policy
Under the PES Policy, free agent rookies and veterans are subject to pre-employment urine tests,
including testing at the NFL Combine.
896
All players are also subject to at least one annual urine test for
prohibited substances to occur at training camp or whenever a player reports as part of the player’s pre-
season physical.
897
Additionally, ten players per club are randomly selected for urine testing each week
during the pre-season, regular season, and postseason.
898
During the off-season, players under contract
who are not otherwise subject to reasonable cause testing (discussed below) may be tested at the
discretion of the Independent Administrator (subject to a maximum of six combined urine and blood
tests).
899
The PES Policy also allows for blood testing under the following circumstances: (1) 20% of every club’s
roster will receive blood testing once annually; (2) each week during the pre-season, regular season, and
postseason, five players from eight randomly selected clubs who are selected for urine testing will also
receive blood testing;
900
(3) 10% of every club’s roster will receive blood testing in the off-season; and,
(4) pre-employment blood tests may be administered to free agent rookies and veterans, including 30
players randomly selected at the Combine who will undergo urine and blood testing.
901
The Independent
Administrator randomly selects the players to be tested.
Finally, the PES Policy allows for reasonable cause testing for players who have previously tested
positive for PES or for whom there is sufficient credible evidence
902
of prior PES involvement (up to two
football seasons prior to the player’s applicable college draft).
903
In no circumstance may a player undergo
more than 24 combined urine and/or blood tests per year.
904
b. Substance Abuse Policy
Under the Substance Abuse Policy, players are subject to testing on the following terms: (1) a rookie or
veteran player not under contract may be subject to a pre-employment test if that player was not under
contract to his last club on the date of its last game of the preceding season and the player has not had a
test in the four-month period prior (excluding an NFL Combine test); (2) draft-eligible players are subject
to pre-employment tests during the NFL Combine; (3) all players under contract are subject to one annual
test during the off-season; (4) all players in the Intervention Program
905
will be required to provide
specimens when determined by the Medical Advisor (discussed below in Section 4: Administration); and,
(5) a club and player may agree that the player will submit to unannounced testing during the term of his
contract if the club has a reasonable basis for such testing.
906
For players already in the NFL, it is fairly easy not to run afoul of the Substance Abuse Policy. Players
are only tested for drugs of abuse during an off-season window that begins in April and ends in August.
907
So long as players do not use drugs of abuse during this time frame (or sufficiently in advance of this time
frame), they will not test positive under the Substance Abuse Policy and can otherwise use drugs of abuse
without detection or consequences under the Policy during the remainder of the year.
908
Moreover, the
!
132!
NFLPA issues a reminder about the drug testing dates to all players approximately a month before the
drug testing window begins.
909
Because players should be able to avoid problems with the Substance
Abuse Policy fairly easily, the off-season test is referred to even by NFL medical personnel as “an
intelligence test.”
910
4. Administration
a. PES Policy
The Independent Administrator on Performance-Enhancing Substances, jointly selected by the NFL and
the NFLPA, administers the PES Policy.
911
The current Independent Administrator is Dr. John Lombardo,
an expert in PES.
912
Subject to limitations set in the PES Policy, the Independent Administrator is vested
with the discretion to make determinations concerning, among other things, the method by which players
will be subjected to testing each week, the selection of players to be tested each week, the number and
frequency of reasonable cause and off-season tests to administer, the scheduling of medical evaluations
associated with the use of prohibited substances, review and approval of therapeutic use exemptions, and
finding and certifying violations for disciplinary action.
913
The PES Policy also employs a chief forensic toxicologist jointly selected by the NFL and NFLPA. The
toxicologist, among other things, audits the operation of testing laboratories, reviews and certifies lab
results, and provides advice to the NFL and NFLPA on anti-doping. The PES Policy also includes a
jointly selected collection vendor to implement a training and certification process for all persons
involved in the collection of samples under the PES Policy.
914
b. Substance Abuse Policy
The NFL and NFLPA jointly select a Medical Director, who is responsible for developing and
implementing all aspects of the Substance Abuse Policy that relate to the treatment of players.
915
The NFL
and NFLPA also jointly select a Medical Advisor, who has the responsibility of serving as medical review
officer and overseeing selection and testing under the Substance Abuse Policy’s treatment program,
known as the Intervention Program and discussed in detail below.
916
Additional administrators for the
Substance Abuse Policy include treating clinicians,
917
team substance abuse physicians,
918
a chief forensic
toxicologist,
919
collection vendor(s),
920
and club physicians.
921
5. Therapeutic Use
Therapeutic use exceptions (“TUEs”) are available for players under both the PES Policy and the
Substance Abuse Policy by applying to the Independent Administrator of the PES Policy and the Medical
Advisor for the Substance Abuse Policy.
922
“The TUE application should be filled out and submitted by
the player’s treating physician and should include all pertinent medical records documenting the
diagnosis.”
923
The NFL applies the following guidelines to all TUE requests:
1. The medication must be necessary and indicated for treatment of the
specific medical problem for which it has been requested;
2. Acceptable alternative treatments with medications that are not
prohibited were attempted but failed, or reasons for not prescribing these
alternative treatments have been presented;
3. Appropriate evaluation has been completed and all medical records
documenting the diagnosis have been submitted for review; and,
!
133!
4. The applicant may not begin use of the prohibited substance until after
the TUE is granted.
924
6. Treatment
Some of the sports leagues’ drug policies provide for the player to undergo treatment concerning his drug
use in lieu of or in addition to punishment. We thus analyze that issue across the leagues, beginning here
with the NFL.
a. PES Policy
The PES Policy does not provide for any treatment. Nevertheless, treatment might be available through
the player’s club-funded health insurance policy.
b. Substance Abuse Policy
According to the Substance Abuse Policy, “[t]he cornerstone of th[e] Policy is the Intervention
Program.”
925
“Under the Intervention Program, Players are tested, evaluated, treated, and monitored for
substance abuse.”
926
The Intervention Program consists of three possible stages of treatment. If the player
complies with his treatment and does not fail any tests, he will be discharged from the Intervention
Program. However, if the player does not comply or fails drug tests, he will be advanced into more
aggressive stages of treatment and be subject to increasing discipline.
A player can enter the Intervention Program in three ways: (1) a positive test result; (2) “[b]ehavior
(including but not limited to an arrest or conduct related to an alleged misuse of Substances of Abuse
occurring up to two (2) football seasons prior to the Player’s applicable scouting combine) which, in the
judgment of the Medical Director, exhibits physical, behavioral, or psychological signs or symptoms of
misuse of Substances of Abuse”; and, (3) “Self-Referral: Personal notification to the Medical Director by
a Player of his desire voluntarily to enter Stage One of the Intervention Program prior to his being notified
to provide a specimen leading to a Positive Test Result, and prior to behavior of the type described above
becoming known to the Medical Director from a source other than the Player.”
927
Once in the Intervention Program, the players are referred to the appropriate clinical professionals to
develop a treatment plan for the player.
928
The Medical Director must then approve the treatment plan.
929
Additionally, once in the Intervention Program, the player is subject to additional testing at the discretion
of the Medical Director.
930
If a player complies with his treatment plan, he can be discharged from the Intervention Program in as
little as 90 days.
931
If the Medical Director believes the player needs additional treatment or if the player
fails to comply with his treatment plan, such as by failing a test, the player will advance to Stage Two of
the Intervention Program.
932
In Stage Two, a player can be subject to as many as ten unannounced drug
tests per month.
933
If a player complies with his treatment plan in Stage Two, he can be discharged from the Intervention
Program in as little as 12 months.
934
However, again, if the Medical Director believes the player needs
additional treatment or if the player fails to comply with his treatment plan, such as by failing a test, the
player will advance to Stage Three of the Intervention Program and be subject to additional treatment and
evaluation.
935
A player’s path through the Intervention Program is detailed further in Figure 4-A below.
!
134!
7. Discipline
936
a. PES Policy
On the first violation, the PES Policy provides for different punishment based on the type of violation. All
violations are treated similarly in the second and third instances, as illustrated in Table 4-A below.
937
Table 4-A: NFL PES Policy Discipline Schedule
Type of Violation
First
Violation
Second
Violation
Third
Violation
Violation of Law or Sufficient Credible Evidence
938
6 games
10 games
2 years
Positive Test (Diuretic or Masking Agent)
2 games
10 games
2 years
Positive Test (Stimulant or Anabolic Agent)
4 games
10 games
2 years
Positive Test (Prohibited Substance Plus Diuretic,
Masking Agent, Attempt to Adulterate, or Attempt to
Manipulate)
6 games
10 games
2 years
In 2016, approximately 19 NFL players were suspended for violating the PES Policy,
939
an increase from
13 players in 2015, and 16 players in 2014.
940
In addition to the fines and suspensions described above, players potentially face contractual
consequences for violating the PES Policy. When a player has violated the PES Policy, his club is entitled
to proportional forfeiture of bonuses previously paid.
941
For example, if a player received a $10 million
signing bonus for a five-year contract, and the player then fails a PES test after the second season, the
player could be required to return $6 million of the signing bonus to the club.
942
Similarly, if a player is
entitled to have his Paragraph 5 (i.e., base) salary guaranteed in his second season, but fails a PES test
between the first and second seasons, the contract might contain a clause permitting the club to void the
guarantee in the second season.
943
Because NFL compensation is generally not guaranteed, these financial
punishments can be more harmful to a player than the suspensions listed above.
b. Substance Abuse Policy
Players are not disciplined for initial positive test results under the Substance Abuse Policy. Instead,
players are entered into the Intervention Program, discussed above. Provided players comply with their
treatment programs under the Intervention Program, they will not be disciplined.
However, players who fail to comply with the Intervention Program are subject to increasing levels of
discipline. Figure 4-A below demonstrates a player’s potential path and discipline through the
Intervention Program.
Additionally, a player who voluntarily enters the Intervention Program cannot be disciplined so long as he
complies with his treatment plan.
944
In reality, this safe harbor provision is limited by the general
tenuousness of NFL players’ contracts and careers, which are often terminated for a variety of reasons.
Because NFL players will look to avoid anything that sheds negative light on them—including
voluntarily entering the Intervention Program—it is questionable how often players ever take advantage
of the Substance Abuse Policy’s safe harbor provision.
!
135!
In 2016, approximately 26 players were suspended for violating the Substance Abuse Policy,
945
a decrease
from 29 players in 2015, but more than the 23 players suspended in 2014.
946
Many more players were
likely fined, but these statistics are not publicly available pursuant to the Policy’s confidentiality
provisions, discussed next.
Players are also subject to discipline for violations of law involving alcohol or drugs of abuse.
A player’s first offense involving alcohol will generally result in a two-game suspension.
947
If there are
“aggravating circumstances, including but not limited to felonious conduct, extreme intoxication (BAC of
.15% or more), property damage or serious injury or death to the Player or a third party, and/or if the
Player has had prior drug or alcohol-related misconduct, increased discipline may be imposed.”
948
A
second offense involving alcohol results in an eight-game suspension.
949
A player’s first offense involving drugs of abuse will generally result in a four-game suspension.
950
Discipline may be increased if there are aggravating circumstances similar to those discussed above.
951
A
second offense involving drugs of abuse results in a six- to ten-game suspension.
952
Finally, players who violate the Substance Abuse Policy are subject to the same potential contractual
penalties as those discussed above arising out of violations of the PES Policy.
8. Confidentiality
Both the PES Policy and Substance Abuse Policy mandate that players, clubs, the NFL, NFLPA, player
agents, and all persons involved in administering the polices protect the confidentiality of matters covered
by the policies.
953
a. PES Policy
Under the PES Policy, “public disclosure, directly or indirectly, of information concerning positive tests,
appeals or other violations of th[e] [PES] Policy is not permitted.”
954
The PES Policy allows the NFL to
publicly announce or acknowledge disciplinary action against a player when a suspension is upheld by an
arbitrator and to publicly disclose information relating to the discipline of a player to correct inaccurate
public claims made by the player or his representatives.
955
Finally, under the PES Policy, a player, club, or
club employee is subject to a $500,000 fine for breaching the confidentiality provisions.
956
b. Substance Abuse Policy
The Substance Abuse Policy requires confidentiality relating “to the history, diagnosis, treatment,
prognosis, test results, or the fact of participation in the Intervention Program of any Player[.]”
957
The
Substance Abuse Policy allows for disclosure under the same circumstances as the PES Policy and
additionally allows for players to authorize or disclose information and allows the Medical Advisor or
NFL to disclose to a club information about a player who the club is contemplating acquiring.
958
Finally,
like the PES Policy, under the Substance Abuse Policy, a player, club, or club employee is subject to a
$500,000 fine for breaching the confidentiality provisions.
959
With this understanding of the NFL policies we are ready to compare them to what is in place for the
other leagues.
!
136!
B. MLB’s Drug Policies
MLB and the MLBPA have agreed to the Joint Drug Prevention and Treatment Program (“Joint
Program”). The Joint Program, last amended in December 2016, covers both PES and drugs of abuse.
Where it is helpful, we will discuss the Joint Program’s treatment of the different drugs separately.
1. Substances Prohibited
The Joint Program prohibits the use, possession, sale, or distribution of four categories of substances:
drugs of abuse,
960
PES,
961
stimulants,
962
and Dehydroepiandrosterone (“DHEA”).
963
During the term of the
Joint Program, MLB and the MLBPA may jointly agree to ban any additional substances.
964
Additionally,
if the federal government adds a substance to Schedule I, II, or III of the Code of Federal Regulations
Schedule of Controlled Substances, then that substance is automatically added to the list of prohibited
substances as a drug of abuse, PES, or stimulant.
965
However, MLB does not test for stimulants during the off-season.
966
2. Types of Tests and Prohibited Conduct
Like the NFL, MLB uses urine tests for PES, stimulants, and DHEA,
967
and blood tests for hGH.
968
“[I]f any substance identified in the test results meets the levels set forth in the Collection Procedures and
Testing Protocols of the Program,” then that test shall be considered “positive.”
969
Additionally if a player
refuses or, without good cause, fails to take a test, or engages in activity to prevent the collection of a
specimen, then the player will be deemed to have failed a test.
970
Likewise, a test will be considered
positive if a player “attempts to substitute, dilute, mask or adulterate a specimen or in any other manner
alter a test.”
971
Players may also be subject to disciplinary action, under a just cause standard, for “any . . .
violation of [the Joint Program’s prohibitions], including, but not limited to, non-analytical positives.”
972
3. Number of Tests
a. PES
Each player is tested for PES, stimulants, and DHEA upon reporting to spring training and receives at
least one other unannounced test on a randomly selected date between the start of spring training and the
final day of the postseason.
973
In total, 4,800 unannounced tests for PES and stimulants are administered
to randomly selected players during the season
974
and 1,550 unannounced, random tests for only PES and
DHEA are administered during the off-season, in order to ensure that all players are subject to at least one
random off-season test.
975
Each player is also randomly tested for hGH once during spring training,
976
and
900 random, unannounced blood tests for hGH are performed throughout the year.
977
There is no limit on
the number of times an individual player may be tested for hGH.
978
During the 2016 season, MLB conducted 8,281 drug tests.
979
6,634 of the tests were urine and 1,647 were
blood.
980
There were 15 failed tests—12 for PES and three for stimulants.
981
Players are also potentially subject to just cause testing or, in the case of players who violate the Joint
Program, additional follow-up testing. If the Commissioner or the MLBPA notifies the other that it has
“reasonable cause” to believe that a player has “engaged in the use, possession, sale or distribution of a
[PES or stimulant]” in the past year,” then the player may be subject to a test within 48 hours of
notification.
982
Players who test positive for PES are subject to three unannounced tests in the year after
!
137!
the positive test, and players who test positive for stimulants are subject to six unannounced tests in the
year after the positive test.
983
b. Drugs of Abuse
Unlike in the NFL, MLB players are generally not required to undergo testing for drugs of abuse, unless
the Commissioner or MLBPA presents the other with reasonable cause for testing.
984
If a player tests
positive for a drug of abuse after undergoing reasonable cause testing, he is referred to the Treatment
Board for an initial evaluation,
985
after which the Treatment Board may develop a treatment program
consisting of some combination of counseling, in- or out-patient treatment, and follow-up testing.
986
4. Administration
The Independent Program Administrator, jointly selected by the MLBPA and MLB, oversees the Joint
Program.
987
The Independent Program Administrator administers and audits the Joint Program’s testing
regime and develops related educational programs.
988
Additionally, the Treatment Board—consisting of
two representatives (a lawyer and a physician) appointed by the MLBPA, two representatives (a lawyer
and a physician) appointed by MLB, and a fifth neutral labor arbitrator—supervises the treatment of
players who have or are suspected to have used drugs of abuse.
989
Of note, the Independent Program Administrator is responsible for publicly releasing a report by
December 1, of each year that sets forth the number of tests conducted, the number of positive tests that
resulted in discipline, the substances involved in the tests that resulted in discipline, the number of non-
analytical positives that resulted in discipline, and the number of TUEs issued, broken down by the
category of medication.
990
MLB’s PES report is a commendable exercise in transparency. By disclosing its drug testing efforts and
results and subjecting them to public scrutiny, MLB is demonstrating its commitment to the integrity of
the game. While we believe the NFL should seriously consider releasing a similar report, such a report
has minimal (if any) direct impact on player health and thus it is outside the scope of our concern here.
5. Therapeutic Use
As in the NFL, a player with a medical condition that requires treatment by a substance prohibited by the
Joint Program can apply to the Independent Program Administrator for a TUE.
991
The Independent
Program Administrator determines whether or not to grant the TUE after consultation with members of
the Medical Advisory Panel or outside specialists.
992
6. Treatment
a. PES
As with the NFL, the Joint Program does not provide for treatment in the case of PES use.
b. Drugs of Abuse
The Joint Program does provide for treatment in the case of drugs of abuse in a manner substantially
similar to that of the NFL. Under the Joint Program, a player begins treatment for drugs of abuse if he has
previously failed a drug test (as the result of reasonable cause testing), or “is otherwise found to have used
or possessed” a drug of abuse.
993
The player’s treatment program is determined by the medical
professionals on the Treatment Board, who may consult with other treating doctors or experts in the
!
138!
field.
994
The treatment program “may include any or all of the following: counseling, impatient treatment,
outpatient treatment and follow-up testing.”
995
A player is subject to discipline for failing to cooperate
with his treatment plan, as discussed below.
7. Discipline
Punishments for violations of the Joint Program depend on the category of prohibited substance involved,
the nature of the offense, and the number of previous violations (if any). The rules are summarized in
Table 4-B below:
Table 4-B: MLB Joint Program Discipline Schedule
Type of Violation
First
Violation
Second
Violation
Third
Violation
Fourth
Violation
PES Use
996
80 games
162 games
Permanent
suspension;
can apply for
reinstatement
after 2 years
NA
PES Sale or Distribution
997
80–100 games
162 games
Permanent
suspension;
can apply for
reinstatement
after 2 years
NA
Stimulant Use
998
Follow-up
testing
50 games
100 games
Permanent
suspension
Stimulant-Related
Convictions
999
25–50 games
50–100 games
Permanent
suspension
NA
Stimulant Sale or
Distribution
1000
60–90 games
2-year
suspension
Permanent
suspension
NA
DHEA Use
1001
Follow-up
testing
25 games
80 games
Permanent
suspension
DHEA-related Convictions
1002
25–50 games
50–100 games
Permanent
suspension
NA
DHEA Sale or Distribution
1003
60–90 games
2-year
suspension
Permanent
suspension
NA
Failure to Comply with
Treatment Program
1004
15–25 games
25–50 games
50–75 games
At least one year
suspension
1005
Drugs of Abuse Sale or
Distribution
1006
60–90 games
2-year
suspension
Permanent
suspension
NA
Drugs of Abuse-related
Convictions
1007
25–50 games
50–100 games
Permanent
suspension
NA
DHEA is treated differently than other PES. “DHEA is a hormone that is naturally made by the human
body. . . . Athletes and other people use DHEA to increase muscle mass, strength, and energy.”
1008
DHEA
is legal
1009
and can be purchased over the counter as a dietary supplement,
1010
which might explain its
differential treatment. Despite its legality, MLB, the NFL, NBA, NHL, NCAA, and the World Anti-
Doping Agency (“WADA”)
1011
have all banned the use of DHEA.
1012
!
139!
It is unclear whether players who voluntarily refer themselves for treatment can be disciplined under the
Joint Program. In reviewing a draft of this Report, MLB stated:
If a Player comes forward and discloses to the Joint Treatment Board that
he has substance use problem, he will be evaluated and prescribed a
treatment program. If he remains compliant with his treatment program
and the Treatment Board’s recommendations, he will not be subject to
discipline under the Joint Drug Program. This process is described in
Section 4 of the Joint Drug Program.
Nevertheless, based on our reading of the Joint Program, while Section 4 does describe the evaluation and
treatment provided to players, it does not say anything about a player not being subjected to discipline for
voluntarily referring himself for treatment.
8. Confidentiality
Like in the NFL, information about an MLB player’s test results, testing history, and treatment program
are generally confidential.
1013
However, there are many exceptions to this rule. First, MLB and the
MLBPA may, upon request, provide a Congressional committee with an anonymized summary of tests
conducted under the Joint Program.
1014
Second, MLB may inform a club that the club’s player has been
placed in a treatment program.
1015
Third, a club may disclose a player’s treatment history to a potential
trade partner;
1016
MLB may publicly disclose that a player has been suspended for a specific number of
days for violating the Joint Program or for refusing to take or tampering with a test.
1017
Fourth, MLB, in
announcing the suspension of a player, can reveal the specific substance which caused the violation of the
Joint Program.
1018
Finally, both MLB and the MLBPA may disclose details of a player’s testing history to
correct inaccurate or misleading claims made by that player.
1019
C. The NBA’s Drug Policies
The NBA and NBPA have agreed to the Anti-Drug Program. The Anti-Drug Program, last amended as
part of the 2017 CBA, covers both PES and drugs of abuse. Where it is helpful, we will discuss the Anti-
Drug Program’s treatment of the different drugs separately.
1. Substances Prohibited
Prohibited substances in the NBA fall into four categories: (1) drugs of abuse;
1020
(2) marijuana and its by-
products (including synthetic cannabinoids); (3) steroids, PES, and masking agents (“SPEDs”);
1021
and,
(4) diuretics.
1022
Additionally, any steroid or PES that is declared illegal
1023
during the term of the CBA is
automatically added to the list of prohibited substances, and either the NBA or NBPA can convene a
meeting of the Prohibited Substances Committee to request that the Committee add a substance to the list
of prohibited substances.
1024
2. Types of Tests and Prohibited Conduct
The NBA’s Anti-Drug program includes both urine and blood testing.
1025
Any test under the Anti-Drug
program will be considered “positive” for a prohibited substance if: (1) for a test for a drug of abuse or
marijuana, the test confirms levels of the prohibited substance meeting or exceeding the levels set forth in
the CBA;
1026
(2) for a test for a SPED, the test confirms levels of the SPED meeting or exceeding the
levels set forth in the CBA;
1027
(3) for a test for a diuretic, the test confirms any detectable level of a
diuretic;
1028
(4) a player refuses to submit to a test or fully cooperate with the testing process;
1029
(5) a
!
140!
player fails to submit to a scheduled test without reasonable explanation;
1030
or, (6) a player attempts to
substitute, dilute, or adulterate a specimen.
1031
Additionally, even if a player has not failed a test, the NBA’s Anti-Drug Program prohibits the “use,
possession, or distribution” of prohibited substances.
1032
3. Number of Tests
A player is required to undergo random urine testing for prohibited substances at any time, without prior
notice, no more than four times during each season and no more than two times during the off-season.
1033
Players can also be blood tested a maximum of two times during the season and once in the off-season.
1034
The NBA can conduct a maximum of 1,525 total random tests during the season and a maximum of 600
total random tests during the off-season.
1035
Players are also subject to reasonable cause testing. If the NBA or NBPA has reasonable cause to believe
that a player is engaged in the use, possession, or distribution of a prohibited substance, then that party
may request a conference with the “Independent Expert,” who will determine whether reasonable cause
exists to test the player.
1036
If reasonable cause exists, the player may be tested up to four times during the
subsequent six-week period.
1037
4. Administration
A jointly selected NBA/NBPA Medical Director oversees the NBA’s Anti-Drug Program concerning
drugs of abuse and marijuana.
1038
A separate Medical Director is responsible for overseeing the SPED
portion of the Anti-Drug Program.
1039
Additionally, a jointly selected Independent Expert issues
authorizations for reasonable cause testing.
1040
A five-member Prohibited Substance Committee,
consisting of one NBA representative, one NBPA representative, and three jointly selected individuals,
makes recommendations to the NBA and NBPA for changes to the list of Prohibited Substances,
including laboratory analysis cutoff levels.
1041
Finally, the NBA’s Grievance Arbitrator (who handles a
variety of potential grievances under the CBA) is responsible for resolving any and all disputes arising
under the Anti-Drug program.
1042
5. Therapeutic Use
Although it is not mentioned in the CBA, the NBA’s Anti-Drug program does contain a TUE process.
1043
A player can petition the Medical Director of the Anti-Drug program for permission to use a banned
substance.
1044
The Medical Director determines whether the player is entitled to the TUE based upon the
player’s diagnosis and relevant medical information submitted by the player, including but not limited to
a validly issued prescription.
1045
6. Treatment
Like the NFL, the NBA’s Anti-Drug Program includes a treatment component. The NBA’s Anti-Drug
Program has three different treatment programs depending on the substance involved: drugs of abuse
(excluding marijuana); marijuana; and, PES. Discipline for the three programs differs and will be
discussed in the next Section.
a. Drugs of Abuse Program
The Drugs of Abuse Program is a two-stage program that includes education, treatment, counseling, and
additional testing as directed by the Medical Director.
1046
Players enter the Drugs of Abuse Program in
!
141!
one of two ways: (1) by testing positive for a drug of abuse as a rookie;
1047
or, (2) by voluntarily entering
the Drugs of Abuse Program to seek treatment.
1048
b. Marijuana Program
The Marijuana Program also includes education, treatment, counseling, and additional testing as directed
by the Medical Director.
1049
Players enter the Marijuana Program by: (1) testing positive for marijuana;
1050
(2) being found to have used or possessed marijuana by the Grievance Arbitrator;
1051
(3) being convicted
of the use or possession of marijuana;
1052
or, (4) voluntarily entering the Marijuana Program to seek
treatment.
1053
c. SPEDs Program
The SPEDs Program (for steroids, performance-enhancing substances, and masking agents), like the
Drugs of Abuse Program and Marijuana Program, includes education, treatment, counseling, and
additional testing as directed by the SPED Medical Director.
1054
Players enter the SPEDs Program by: (1)
testing positive for a SPED;
1055
or, (2) being found to have used or possessed a SPED by the Grievance
Arbitrator.
1056
Under the 2011 CBA, players could voluntarily enter the SPEDs Program and avoid
discipline,
1057
but that option was eliminated in the 2017 CBA.
1058
7. Discipline
Discipline for a violation of the NBA’s Anti-Drug Program depends on the type of prohibited substance
triggering the violation and, for drugs of abuse only, whether a player is a rookie or a veteran.
a. Drugs of Abuse
Table 4-C below outlines the types of discipline for drugs of abuse in the NBA.
Table 4-C: NBA Drugs of Abuse Program Discipline Schedule
Player Status
First Violation
Second Violation
Rookie
Dismissed and disqualified for at
least one year; contract voided
subject to reinstatement by
agreement of the NBA and
NBPA; enters Drugs of Abuse
Program.
1059
If in Stage 1, suspended until there is
compliance and advanced to Stage 2.
1060
If
in Stage 2, dismissed and disqualified for
at least two years, subject to reinstatement,
and contract voided.
1061
Veteran
Dismissed and disqualified for at
least two years’ subject to
reinstatement by agreement of
the NBA and NBPA; contract
voided.
10621063
For players who entered the Drugs of
Abuse Program voluntarily, if in Stage 1,
suspended until there is compliance and
advanced to Stage 2.
1064
If in Stage 2,
dismissed and disqualified for at least two
years’ subject to reinstatement by
agreement of the NBA and NBPA and
contract voided.
1065
Players who voluntarily enter the Drugs of Abuse Program will not be disciplined provided they comply
with their treatment.
1066
!
142!
In addition to the discipline outlined above, players who are convicted of crimes involving alcohol
(including DUI or DWI) or controlled substances that are not prohibited substances are subject to
discipline as determined by the Commissioner and will be evaluated by the Medical Director of the Anti-
Drug Program, who can mandate counseling.
1067
b. Marijuana
Table 4-D below outlines the types of discipline for marijuana use in the NBA.
Table 4-D: NBA Marijuana Program Discipline Schedule
Violation
Discipline
First
Required to enter Marijuana Program.
1068
Second
Fined $25,000 and required to enter Marijuana Program if not already in.
1069
Third
Suspended for five games and required to enter Marijuana Program if not
already in.
1070
Fourth or more
Suspended for five games longer than immediately preceding suspension and
required to enter Marijuana Program if not already in.
1071
Players who voluntarily enter the Marijuana Program will not be disciplined provided they comply with
their treatment.
1072
c. SPEDs
Table 4-E below explains the discipline meted out for PES use in the NBA.
Table 4-E: NBA SPEDs Program Discipline Schedule
Violation
Discipline
First
Suspended for 25 games and required to enter SPEDs Program.
1073
Second
Suspended for 55 games and required to enter SPEDs Program if not already
in.
1074
Third
Dismissed and disqualified for at least two years’ subject to reinstatement by
agreement of the NBA and NBPA, and required to enter SPEDs Program if not
already in.
1075
Under the 2011 CBA, players who voluntarily entered the SPEDs Program were not disciplined provided
they complied with their treatment.
1076
However, the ability to come forward voluntarily without
punishment was removed in the 2017 CBA.
1077
8. Confidentiality
Except as “reasonably required” in connection with the suspension or dismissal of a player, the NBA, the
clubs, the NBPA, and their affiliates and employees “are prohibited from publicly disclosing information
about the diagnosis, treatment, prognosis, test results, compliance, or the fact of participation of a player
in the [Drug] Program.”
1078
If a player is suspended or disqualified for a violation involving a drug of
abuse or marijuana, the NBA may not publicly disclose the prohibited substance involved, but, if the
player is suspended for conduct involving a SPED, the particular SPED shall be disclosed.
1079
The
Medical Directors, drug program counselors, the Independent Expert, and Members of the Prohibited
!
143!
Substances Committee are also prohibited from public disclosure of information obtained in their
roles.
1080
D. The NHL’s Drug Policies
Like the NFL, the NHL has two separate policies concerning the use of drugs: (1) the Performance
Enhancing Substances Program (“PES Program”); and, (2) Substance Abuse and Behavioral Health
Program (“Substance Abuse Program”). The PES Program was most recently amended as part of the 2013
CBA. The Substance Abuse Program was put into place in 1996 and it has not been changed since then.
We will describe both policies for each issue of interest.
1. Substances Prohibited
a. PES Program
The Prohibited Substances List for the PES Program is based on the WADA Prohibited List, with specific
prohibited substances selected jointly by the NHL and NHLPA for their relevance to professional
hockey.
1081
The Prohibited Substance List is not publicly available, but the parties agreed by letter
agreement accompanying the 2013 CBA to include on the Prohibited Substances List “‘illegal’ stimulants
and amphetamines . . . that are relevant to the sport of hockey.”
1082
b. Substance Abuse Program
The Substance Abuse Program does not define “substances of abuse,” but the Substance Abuse Program
Collection and Laboratory Procedures for Samples includes threshold levels for marijuana, cocaine,
opiates, PCP, amphetamines, and alcohol.
1083
2. Types of Tests and Prohibited Conduct
a. PES Program
The PES Program does not detail the type of specimen that a player must submit, leaving the decision to
the Program Committee (discussed below in Section 4: Administration). Recent news articles indicate
that the PES Program uses urine samples rather than blood testing.
1084
Under the PES Program, a test is “positive,” if: (1) the test indicates levels of the prohibited substance that
exceed the established cutoff levels; (2) the player had an unexcused failure or refusal to take the test; or,
(3) the player attempted to substitute, dilute, mask, or adulterate his test specimen.
1085
While the NHL, like the NFL, employs a “strict liability standard” (i.e., the player will be disciplined
regardless of whether he intended to take a banned substance),
1086
a player has the right to offer an
alternative medical explanation for an adverse analytical finding (i.e. a positive test) under the PES
Program.
1087
If, after considering relevant evidence, the Program doctors determine that a valid alternative
medical explanation exists, then that alternative medical explanation renders the player’s test result
conclusively non-positive and the player is not subject to discipline.
1088
If the Program doctors do not
determine that a valid alternative medical explanation exists, then the doctors must promptly test the
player’s “B” sample,
1089
which was gathered as part of the initial urine specimen collection process. If the
“B” sample tests negative, then the player’s test is conclusively non-positive and the player is not subject
to discipline.
1090
!
144!
b. Substance Abuse Program
The Substance Abuse Program uses urine samples.
1091
To establish a violation of the Substance Abuse Program, there are threshold levels for initial tests and
confirmatory tests for the different substances of abuse.
1092
However, as will be explained further below, it
is important to note that only players who are currently enrolled in the Substance Abuse Program are
tested in an identifiable manner. In other words, there is no identifiable random testing.
3. Number of Tests
a. PES Program
Similar to the NFL, under the PES Program, each NHL club is subject to one team-wide, no-notice drug
test during training camp and one team-wide, no-notice drug test randomly during the regular season.
1093
In addition, “[i]ndividual Players will be randomly selected for no-notice testing during the Regular
Season and Playoffs.”
1094
While the Program Committee may only test up to sixty players during the off-
season, there is no regular season cap.
1095
There is also no limit on the number of times the Program
Committee may test an individual player.
1096
The Program Committee may also test players at any time for reasonable cause if it has “information that
gives it reasonable cause to believe that a Player has, in the previous 12-month period, engaged in the use
of a Prohibited Substance.”
1097
However, the player has 48 hours after receiving Reasonable Cause
Notification to contest the information giving rise to the reasonable cause to an impartial arbitrator.
1098
b. Substance Abuse Program
Unlike the NFL, where all players under contract are subject to an identifiable drug test, the NHL’s
Substance Abuse Program does not subject NHL players to random identifiable testing for substances of
abuse for disciplinary purposes. Tests conducted under the PES Program do report test results for drugs of
abuse but on a de-identified basis.
1099
Only “if a positive result shows a dangerously high level for a drug
of abuse such that it causes concern for the health or safety of the Player or others,” do the Program
Doctors have the right to discover the identity of the player and refer the player for an evaluation under
the Substance Abuse Program.
1100
In response to concerns about cocaine use by NHL players, during the
2015 season it was announced that all tests conducted under the PES Program would include a test for the
drug.
1101
Previously, only one-third of PES Program drug tests tested for drugs of abuse.
1102
Players may also voluntarily enter the Substance Abuse Program.
1103
In fact, voluntarily entering the
program is the principal method by which players begin treatment. It is also possible that players can be
required to undergo a test for a substance of abuse if the NHL or club has reasonable cause to believe the
player has used a drug of abuse, similar to the provision contained in the PES Policy. The Substance
Abuse Program doctors are authorized to require that players in the Substance Abuse Program “undergo
periodic substance testing at a frequency and on a schedule to be determined by the doctors. Such testing
may take place both in season and during the off-season.”
1104
4. Administration
a. PES Program
The Program Committee, comprised of an equal number of NHL and NHLPA representatives and a
consulting expert doctor from each side, administers the PES Program.
1105
The Program Committee is

!
145!
responsible for, among other things, developing an educational program, overseeing the administration of
PES testing, recommending to the NHL and NHLPA which PES from the WADA Prohibited List
1106
they
should include on the Prohibited Substances List, supervising player evaluation and treatment following
positive tests, and administering the TUE process.
1107
b. Substance Abuse Program
“[Q]ualified doctors selected by the League and the NHLPA” administer the Substance Abuse and
Program.
1108
The Substance Abuse Program doctors’ responsibilities include the development of an
educational program, establishment of a multinational counseling network, development of standardized
medical assessment tools for substance abuse problems, making decisions concerning treatment and
follow-up care, and ensuring compliance with the program.
1109
5. Therapeutic Use
a. PES Program
A player may apply to the PES Program Committee for a TUE with respect to a particular prohibited
substance.
1110
“[T]he Program Committee shall review, consider and act upon such Player’s application
expeditiously and approval of the application shall not be unreasonably withheld.”
1111
b. Substance Abuse Program
There is no TUE provision in the Substance Abuse Program.
6. Treatment
a. PES Program
Players who violate the PES Program are referred to the Substance Abuse Program for evaluation and
possible treatment. In contrast, the NFL’s PES Policy does not refer violators to its Intervention Program
for treatment.
b. Substance Abuse Program
Similar to the NFL’s Intervention Program, the Substance Abuse Program is principally a “program of
education, counseling, inpatient and outpatient treatment, follow-up care, and, where appropriate,
sanctions.”
1112
Players who enter the Substance Abuse Program are given an initial evaluation and then a
treatment plan as chosen by the Program Doctors.
1113
7. Discipline
a. PES Program
Table 4-F below explains the types of discipline for PES use by the NHL.
Table 4-F: NHL PES Program Discipline Schedule
Violation
Discipline
First
Suspended for 20 games and referred to Substance Abuse Program.
1114
!
146!
Second
Suspended for 60 games and referred to Substance Abuse Program.
1115
Third
Player permanently suspended, although player can apply for reinstatement
after 2 years.
1116
From the time that the PES Policy was first instituted in 2005 through 2013, it was reported that only one
player tested positive under the PES Policy, causing some to question the effectiveness of the Policy.
1117
As of the date of publication, five players have been disciplined under the PES Policy—though that does
not necessarily mean there have been five positive tests as players could be disciplined for other
violations of the PES Policy. However, because hockey is an Olympic sport, NHL players wishing to play
in the Olympics are also subject to testing by their country’s respective Olympic drug-testing programs
(such as the United States Anti-Doping Agency), and it is thus possible that PES are particularly
uncommon in the NHL.
1118
b. Substance Abuse Program
Table 4-G below explains the types of discipline under the NHL’s Substance Abuse Program. Again, we
note that only players in the Substance Abuse Program are tested in an identified manner, and thus only
those players can be disciplined.
Table 4-G: NHL Substance Abuse Program Discipline Schedule
Violation
Discipline
First
No discipline; enters Stage 1 of Substance Abuse Program.
1119
Second
Suspended during active treatment; enters Stage 2 of the Substance Abuse
Program.
1120
Third
Suspended for a minimum of six months; enters Stage 3 of the Substance Abuse
Program.
1121
Fourth
Suspended for a minimum of one year; enters Stage 4 of the Substance Abuse
Program.
1122
In addition, a player who voluntarily enters the Substance Abuse Program cannot be disciplined provided
he complies with his treatment.
1123
Outside the scope of the Substance Abuse Program, players might still be subject to discipline if they
have violated the law concerning alcohol or a drug of abuse. Indeed, the Substance Abuse Program states
that players may be subject to other discipline outside of the Substance Abuse Program.
1124
The NHL
CBA provides the Commissioner wide discretion to impose discipline for off-ice conduct, including fines,
suspensions, and cancelling a player’s contract.
1125
Any discipline imposed is subject to appeal before a
neutral arbitrator.
1126
8. Confidentiality
a. PES Program
Test results under the PES Program are confidential except that: (1) once a positive test has been
confirmed by the impartial arbitrator (or if no grievance has been filed), the player suspended will be
identified and the fact of and length of his suspension under the Program will be announced; and, (2) if a
player is subject to a transaction that results in a change to his status (e.g., a trade) and that transaction
was completed between the date on which the player tested positive and the date upon which he received
!
147!
his suspension, a club alleging that it was adversely affected by the player’s nondisclosure of his positive
test may file a grievance.
1127
b. Substance Abuse Program
The assessment of alcohol and drug problems under the Substance Abuse Program shall be conducted
“with the assurance of confidentiality.”
1128
The Substance Abuse Program recognizes that “records which
contain information pertaining to the diagnosis or treatment of psychiatric, alcohol- or drug-related
disorders are subject to strict confidentiality” and therefore requires the player-patient’s prior written
authorization for disclosure.
1129
The Substance Abuse program doctors are responsible for “[a]ppropriate
maintenance of confidentiality of Player records.”
1130
E. The CFL’s Drug Policies
The CFL-CFLPA Policy to Prevent the Use of Performance Enhancing Drugs (“PED Policy”) was most
recently amended in April 2016.
The CFL does not have a policy concerning drugs of abuse and the CFL CBA specifically declares that
“there shall be no drug testing conducted in relation to any player in the C.F.L. except as provided for in
the [PED Policy].”
1131
However, the CFL CBA states that the CFLPA and the CFL Player Relations
Committee (“CFLPRC”) “shall continue with a Committee which shall have the mandate of studying and
gathering information with respect to drug abuse related to both illegal and performance enhancing
drugs.”
1132
1. Substances Prohibited
The PED Policy prohibits PES, stimulants, and masking agents.
1133
2. Types of Tests and Prohibited Conduct
Like the NFL’s PES Policy, the CFL’s PED Policy authorizes the collection of blood and urine
samples.
1134
According to the PED Policy, “[e]xcepting those drugs for which a quantitative reporting threshold is
specifically identified in the Prohibited List, the detected presence of any quantity of a Performance
Enhancing Drug, its Metabolites or Markers in a Player’s sample shall result in an Adverse Analytical
Finding.”
1135
In addition to adverse analytical findings, players are subject to discipline for refusing to
comply with the testing provisions, tampering or attempting to tamper with the sample collection process,
administering or attempting to administer (or assisting with, encouraging, or covering up the
administration of) a PES to any other player, and conviction in Canada of a criminal offense for
possession or trafficking of a PES on the CFL Prohibited List.
1136
3. Number of Tests
Beginning with the 2016 season, all players are tested under the PED Policy.
1137
In addition, players are
subject to targeted testing if: (1) “the laboratory has recommended follow-up testing based on their
analytical investigation;” (2) “the Player is presently undergoing counseling and as a condition of their
counseling, they are subject to further testing;” or, (3) “the Player has been granted a retroactive
exemption” for previously refusing to submit to a drug test.
1138
Finally, if a player has previously
committed a violation of the PED Policy, then the player will be subject to mandatory testing for a two-
year period following the violation, up to a maximum of eight drug tests.
1139
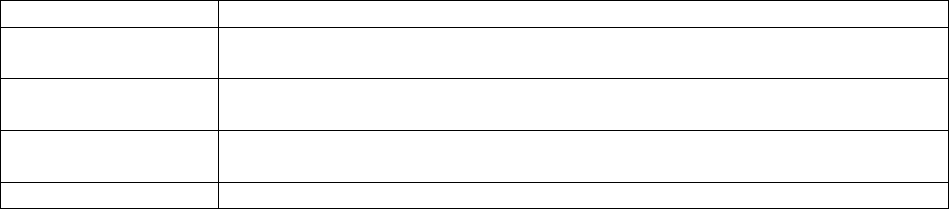
!
148!
The CFL has the authority to reduce testing frequency, at any time and in its sole discretion.
1140
All
testing is done randomly, with no advance notice, and may occur at any time during the calendar year.
1141
4. Administration
The CFL and CFLPA are jointly responsible for administering the PED Policy, but the PED Policy does
not elaborate on the specifics of that administration.
1142
5. Therapeutic Use
The Designated Medical Authority,
1143
a doctor jointly appointed by the CFL and CFLPA for the purpose
of reviewing TUE applications, may grant a TUE to a player if: (2) the player could experience a
significant health impairment if the substance “were to be withheld in the course of treating an acute or
chronic medical condition”; (3) the use of the substance would “produce no additional achievement or
performance other than that which might be anticipated by a return to a state of normal health”; and, (3)
there is not a “reasonable therapeutic alternative” to using the prohibited substance.
1144
6. Treatment
The CFL’s PED Policy makes treatment available to the players. “If a Player is suspended by the CFL
pursuant to the terms of [the PED] Policy, such Player must participate in an assessment and clinical
evaluation, to determine whether a counselling program would be recommended…. The program would
be tailored to meet the specific needs of the Player and may include, but is not limited to, the following:
(a) counselling from medical personnel or substance abuse experts; (b) remedial education that provides
various information including alternatives to the use of performance enhancing substances; and (c)
community service, including speaking to other Players or members of the public about the dangers of
using Performance Enhancing Drugs in sport.”
1145
Nevertheless, “it is at the sole discretion of the player”
whether he receives treatment.
1146
In contrast, the NFL makes treatment available as part of its Substance Abuse Policy but not its PES
Policy.
7. Discipline
Table 4-H below explains the types of discipline for PES use by the CFL.
Table 4-H: CFL PED Policy Discipline Schedule
Violation
Discipline
First
Suspended for two games, must complete educational course, undergo a clinical
evaluation, and subject to additional drug testing for two years.
1147
Second
Suspended for nine games, must complete educational course, undergo a
clinical evaluation, and subject to additional drug testing for two years.
1148
Third
Suspended for one year, must complete educational course, undergo a clinical
evaluation, and subject to additional drug testing for two years.
1149
Fourth
Suspended for life.
1150
!
149!
A player who voluntarily admits a problem using PES is not subject to discipline and will undergo a
clinical evaluation.
1151
In contrast, the NFL’s PES Policy does not offer self-referrals a safe harbor from
discipline.
8. Confidentiality
The CFL, CFLPA, CFL Safety Committee, Sample Collection Authority, and the Substance Abuse
Counseling Organization may not share a player’s medical information.
1152
However, the permitted
disclosure of information about a player’s failed drug test is much broader. As of 2016, the PED Policy
dictates that “the CFL and CFLPA shall disclose the name of every Player who violates the [PED] Policy
including disclosure of the summary details of the applicable violation (substance detected, sanction
imposed, reasons for a sanction reduction, etc.) but only after all appeals available to the Player under the
[PED] Policy have been exhausted.”
1153
Additionally, the PED Policy also authorizes “the CFL
Commissioner and the President of the CFLPA, or their respective designees,… to speak publicly and
disclose any information about a Player that has violated the [PED] Policy.”
1154
F. MLS’ Drug Policies
MLS’ Substance Abuse and Behavioral Health Program and Policy (“Substance Abuse Policy”) covers
both PES and drugs of abuse. The Substance Abuse Policy was most recently amended as part of the 2015
CBA.
1. Substances Prohibited
MLS’ Substance Abuse Policy regulates four types of substances.
First, the Substance Abuse Policy “prohibits the use or possession of any controlled substance without a
prescription issued by a physician licensed to practice medicine.”
1155
The Substance Abuse Policy also
declares that “[p]rescription drugs, even if properly prescribed, may also be prohibited if such drug is not
being used for an approved medical reason[.]”
1156
Second, the Substance Abuse Policy prohibits the use of “street drugs,” including, “without limitation, (1)
amphetamines, (2) barbiturates, (3) benzodiazepines, (4) cocaine, (5) marijuana, (6) methadone, (7)
methaqualone, (8) opiates, (9) phencyclidine (PCP), (10) propoxyphene, (11) ecstasy, and (12) club drugs
including GHB and their analogs[.]”
1157
Third, while MLS “recognizes that alcohol is a legal substance,” the Substance Abuse Policy prohibits
“the use of alcohol on work premises [unless as part of a Club or League function] or reporting to work
under the influence of alcohol or otherwise being affected at work by the consumption of alcohol[.]”
1158
Fourth, the Substance Abuse Policy adopts the WADA Prohibited List for its list of prohibited PES.
1159
2. Types of Tests and Prohibited Conduct
MLS’ Substance Abuse Policy only provides for urine testing.
1160
A player violates the Substance Abuse Policy, in relevant part,
1161
“(i) through receipt of a [failed test], (ii)
use or possession of any controlled substance without a prescription, (iii) abuse of a prescription drug, (iv)
use of alcohol on work premises or reporting to work under the influence of alcohol or otherwise being
affected at work by the consumption of alcohol, (iv) use or possession of [street drugs], [or] (v) use or
!
150!
possession of [PES][.]”
1162
“An adulterated or substituted drug test” is treated as a positive test.
1163
Additionally, a refusal to submit to a drug test is also considered a positive test.
1164
3. Number of Tests
The Substance Abuse Policy dictates that “[a]ll Players are subject to unannounced… testing” for all
prohibited substances.
1165
The Substance Abuse Policy does not set a limit on the number of times a
player can be tested.
1166
4. Administration
The Substance Abuse Policy is “administered by qualified doctors, in associated with a certified
substance abuse and behavioral health counselor (‘Program Professionals’)[.]”
1167
The Program
Professionals are “selected jointly by the [MLS] Commissioner or his designee and the MLS Players
Union[.]”
1168
The Program Professionals are responsible for:
1. Developing an educational program on substance abuse and behavioral
health problems to be presented at least once each year to Players;
2. Overseeing Prohibited Substance and alcohol testing;
3. Establishing a comprehensive multi-national counseling network to
include a 24-hour toll-free number and a network of designated
counseling professionals in each MLS city;
4. Implementing a standardized medical and/or psychological assessment
used to evaluate Players who have violated the [Substance Abuse] Policy
or who self-refer to the [Substance Abuse] Program;
5. Making decisions concerning treatment and aftercare, and ensuring
compliance with those treatment programs. The [Substance Abuse]
Program Professionals shall determine all substance abuse and
behavioral health treatments of Players; and,
6. Selecting and evaluating laboratory, treatment, and aftercare facilities.
1169
5. Therapeutic Use
MLS’ Substance Abuse Policy does not provide any exceptions for therapeutic use.
6. Treatment
MLS’ Substance Abuse Policy provides the possibility of treatment for any violation of the Substance
Abuse Policy, including PES.
1170
A player is required to undergo an evaluation for possible treatment if
the player: (1) refers himself for treatment; (2) has violated the Substance Abuse Policy; or, (3) is
recommended to be evaluated by a league or club official who has “reasonable belief” that the player has
violated the Substance Abuse Policy.
1171
The Program Professionals will make a determination as to
whether or not the player should enter treatment.
1172
Treatment can consist of counseling, outpatient treatment, in-residence treatment at a designated facility,
and necessary aftercare.
1173
Players must following the treatment determinations made by the Program
Professionals.
1174
Also, the costs of treatment are covered by MLS.
1175

!
151!
7. Discipline
Like the NFL, MLS’ Substance Abuse Policy contains a multi-stage treatment program in which the
discipline is determined by the player’s level of compliance with his treatment.
1176
Importantly, this multi-
stage treatment process applies only to drugs of abuse, not PES.
1177
Figure 4-B below shows an MLS
player’s path through the MLS Substance Abuse Policy Program. As compared to the NFL’s Intervention
Program, the level of discipline to be imposed by the MLS Substance Abuse Policy is far less clear. A
player cannot be disciplined for voluntarily referring himself to the Program.
1178
A player who fails a test
for the first time is generally not disciplined for a first offense and is placed in Stage 1 of the Program.
1179
However, upon the recommendation of the Program Professionals, a player can be placed in Stage 2
based on an initial failed test and players in Stage 2 are suspended without pay during treatment and are
only reinstated at the Commissioner‘s discretion.
1180
Generally, speaking, the MLS Substance Abuse
Policy prescribes no specific punishments, leaving discipline to the discretion of the MLS Commissioner,
with the consultation of the Program Professionals.
1181
Moreover, the Substance Abuse Policy does not
explicitly describe how players can exit the Program, which presumably occurs if they comply with
treatment.
Finally, if a player violates the Substance Abuse Policy via the use or possession of PES, his discipline is
determined in the “sole and absolute discretion” of the league, “including, without limitation, fines,
suspension (with or without pay), and/or termination of the Player’s [contract].”
1182
MLS is also the only league that does not provide its players with the possibility of challenging a
violation of the Substance Abuse Policy through a neutral arbitration process. Instead, players can submit
their challenge to a positive test in writing to the Program Professionals who then have the “absolute and
sole” discretion to adjudicate the player’s complaint.
1183
8. Confidentiality
MLS’ Substance Abuse Policy provides limited confidentiality protections for players. A player’s
participation in the treatment phase of the Program is only kept confidential if he is not yet in Stage 1 of
the Program,
1184
which can only occur through a self-referral. If a player is in treatment, MLS “may notify
the Player’s team of [the player’s status and progress] as deemed reasonably necessary.”
1185
If a player has
been suspended or terminated for a violation of the Substance Abuse Policy that did not involve PES,
MLS may disclose “only that a Player has been suspended or terminated pursuant” to the Substance
Abuse Policy.
1186
“If a player is suspended or terminated for use or possession of a [PES], MLS may
disclose such information as it deems necessary/appropriate.”
1187
G. Analysis
The tables below summarize and compare the features of the leagues’ drug policies.
Table 4-I: Comparison of Leagues’ PES Policies
1188
Feature
NFL
MLB
NBA
NHL
CFL
MLS
Independent
administration
Yes
Yes
Yes
Yes
Yes
Yes
Urine tests permitted
Yes
Yes
Yes
Yes
Yes
Yes
Blood tests permitted
Yes
Yes
Yes
No
Yes
No
Maximum number of
annual tests for player
24
No
maximum
Nine
No
maximum
No
maxim
No
maximum
!
152!
without prior violation
um
Therapeutic Use
Exemptions available
Yes
Yes
Yes
Yes
Yes
No
Treatment available
No
No
Yes
No
Yes
Yes
Safe harbor for self-
referrals
No
No
No
No
Yes
No
Discipline for first
violation
Two–Six
games
80 games
25 games
20 games
Two
games
League
discretion
Discipline for second
violation
Ten games
162 games
55 games
60 games
Nine
games
League
discretion
Discipline for third
violation
Two years
Life
Two years
(subject to
reinstatem
ent)
Two years
One
year
League
discretion
Discipline for fourth
violation
NA
NA
NA
NA
Life
League
discretion
Confidential violations
Until
discipline
Until
discipline
Until
discipline
Until
discipline
Until
discipli
ne
Until
discipline
Neutral appeal rights
In part
Yes
Yes
Yes
Yes
No
Table 4-J: Comparison of Leagues’ Drugs of Abuse Policies
Feature
NFL
MLB
NBA
NHL
CFL
MLS
Independent
administration
Yes
Yes
Yes
Yes
No Policy
Yes
Urine tests permitted
Yes
Yes
Yes
Yes
No Policy
Yes
Blood tests permitted
No
No
No
No
No Policy
No
Maximum number of
annual tests for player
without prior violation
One
No tests
Six
No tests
No Policy
No
maximum
Therapeutic Use
Exemptions available
Yes
Yes
Yes
No
No Policy
No
Treatment available
Yes
Yes
Yes
Yes
No Policy
Yes
Safe harbor for self-
referrals
Yes
Maybe
Yes
Yes
No Policy
Yes
Discipline for first
violation
None
None
No
(Marijuana
); One year
for rookies
only or two
years
(other
drugs)
None
No Policy
Determined
by Program
Professiona
ls
evaluation
Discipline for second
violation
Fine
(Marijuana);
Four games
(other drugs)
15–25
games
$25,000
fine
(Marijuana
); 2 years
for rookies
or self-
Suspend
ed
during
treatmen
t
No Policy
League
discretion
!
153!
referrals
(other
drugs)
Discipline for third
violation
4–6 games
50–75
games
Five games
(Marijuana
)
Minimu
m of six
months
No Policy
League
discretion
Discipline for fourth
violation
10 games
(Marijuana);
One year
(other drugs)
At least
One year
Ten games
(Marijuana
)
Minimu
m of
one year
No Policy
League
discretion
Confidential violations
Yes
Yes
Yes
Yes
No Policy
Until
discipline
Neutral appeal rights
Yes
Yes
Yes
Yes
No Policy
No
With the possible exception of how marijuana is regulated, the Big Four’s drug policies do not vary
substantially. Before delving into specific issues of analysis, we note that the leagues and unions balance
multiple factors in creating drug policies, including but not limited to deterrence, treatment, privacy, and
integrity of the game. These policy considerations and value judgments are debatable in many spheres of
the world, not just sports. To be sure, many aspects of these policies impact player health. The three
features of the policies we view as most important and those which we focus on are: (1) the availability of
TUEs; (2) the availability of treatment; and, (3) the opportunity to receive treatment without being subject
to initial discipline. With these issues in mind, we turn to our analysis of how the NFL compares to the
other leagues.
Concerning TUEs, the NFL, MLB and the NBA all offer TUEs for both their PES and drugs of abuse
policies. In contrast, the CFL offers TUEs for its PES policy but does not have a drugs of abuse policy.
We also found no evidence that the NHL offers a TUE for its Substance Abuse Program or that MLS
offers any TUEs. Thus, the NFL’s use of TUEs is at least as good as the other leagues.
All of the leagues, including the NFL, have robust treatment programs for drugs of abuse. However, the
NBA, CFL, and potentially MLS are the only leagues that offer treatment for a player who has violated a
PES Policy. On this issue, it might appear that the NFL can learn compared to the NBA and CFL.
However, there are other relevant considerations concerning the treatment programs offered to players,
discussed next.
The NFL, NBA, NHL, MLS and maybe MLB provide a safe-harbor for players who voluntarily refer
themselves for treatment for drugs of abuse. These provisions importantly allow players to seek help they
might recognize they need without the fear of immediate adverse employment action.
In contrast, no Big Four league offers a safe-harbor for players who have used PES. Under its prior CBA,
NBA players did have a safe-harbor for PES use,
1189
but that option was eliminated in the 2017 CBA.
1190
The NBA does still, however, provide treatment for PES use.
1191
The leagues that do not offer safe-harbor
provisions for PES use may not offer such safe harbors because they believe that there are important
differences between players who take PES and those who take drugs of abuse—we can only speculate
because they have not publicly explained this policy difference. It is possible that these leagues view PES
users as players intentionally looking to cheat the game and their competitors, whereas those using drugs
of abuse need medical care.
However, there is robust scientific evidence supporting the need to provide treatment to PES users. PES
usage has shown to be addictive,
1192
and has been associated with the use of drugs of abuse
1193
(opioids in
!
154!
particular),
1194
body dysmorphic disorder,
1195
depression,
1196
antisocial traits,
1197
mood and personality
disorders,
1198
other psychological disorders,
1199
and cognitive deficits in impulsivity, risk-taking, and
decision-making.
1200
As a result, PES users may experience withdrawal symptoms,
1201
and may be at an
increased risk of suicide.
1202
Consequently, many experts recommend and provide treatment and
counseling for PES users.
1203
H. Recommendation
Recommendation 4-A: The NFL should consider amending the PES Policy to provide treatment to any
NFL player found to have violated the PES Policy.
The NFL and the other leagues recognize that substance abuse is a serious medical issue and, as a result,
provide players with robust counseling and treatment. As discussed above, PES usage has been shown to
be associated with a variety of serious physical and mental ailments. However, only the NBA and CFL
offer treatment for players who have used PES. In light of the potential negative health consequences
associated with PES usage and the treatment provided by the NBA and CFL for PES usage, it seems
prudent for the NFL to consider providing treatment to PES users similar to that provided for by the
Substance Abuse Policy’s Intervention Program.
There is an important clarification to this Recommendation. As stated earlier in this Chapter, we are not
focused on the competitive advantage concerns associated with PES use or the discipline imposed by the
leagues for drug or PES usage. We are focused on the health implications of drug and PES policies. Thus,
our Recommendation should not be read to suggest that because players might need treatment for PES
usage that they should not be disciplined—as is the case for first time offenders of the Substance Abuse
Policy.
As discussed in the Introduction, the NFL declined to review this Report. However, MLB did provide
comments on the Report which may provide insight into the viewpoints of the other professional leagues.
MLB did not agree with this Recommendation, stating:
There are no established treatment programs for PEDs, and since the
recidivism rate for PEDs is fairly low, there is no support for the position
that this class of prohibited substances warrants a response based on
treatment. It is also an established practice of not just MLB, but all other
professional leagues and international anti-doping organizations that the
use of PEDs affects the integrity of play and should be responded with a
disciplinary perspective as opposed to a clinical one. Our experts advise
not including “PED treatment programs” as a recommendation in the
report.
As a preliminary matter, we note that the NBA and CFL do provide treatment to PES users. Thus, there is
a disagreement among the leagues (and potentially also the unions) on this issue, suggesting further
research is needed.
We further reply to MLB with a clarification and with a disagreement. We understand sports
organizations’ need to discipline players who have violated PES policies. Our recommendation does not
seek the elimination or reduction of discipline for PES violations in any way. Instead, we believe it is
appropriate to consider providing players who have violated the PES Policy with counseling, regardless
of any discipline imposed. This is where we and MLB disagree.

!
155!
MLB rejects counseling for PES use on the grounds that “[t]here are no established treatment programs
for PEDs.” As discussed above, experts in the field recommend and do provide treatment for PES usage
and its associated problems. Whether these programs are sufficiently “established,” is beyond our
expertise, but it nonetheless is an issue worth further consideration.
CHAPTER 5: COMPENSATION
This Chapter examines the form and nature of player compensation in the NFL, MLB, NBA, NHL, CFL,
and MLS.
1204
In reviewing this Chapter, it is important to understand that the structures, operations and
finances of the NFL, MLB, NBA, and NHL—the “Big Four”—are considerably different from those of
the CFL and MLS due to, among other things, their long-standing place in the United States and the
amount of their revenues (billions versus millions).
Compensation is an important component of player health. First, the different compensation structures
and systems in the leagues can influence players’ decisions about their physical and mental health, for
example when to play through injury, when to retire, and the like. In their efforts to maximize their
earnings (and sometimes, eligibility for various benefits), some players might sacrifice their short- and/or
long-term physical and mental health.
1205
The compensation structures dictate when or if a player faces
such a trade-off.
Compensation may also be related to health in a second way. Without adequate savings and benefits
during and after NFL play, players may find themselves insufficiently prepared to meet their physical and
mental health needs, especially in the event of crisis.
1206
In addition, as we discussed in greater detail in
Chapter 3, crises in physical and mental health are closely tied to bankruptcy, home foreclosure, and other
serious financial setbacks.
1207
In the worst case scenario, these two outcomes can lead to a vicious cycle—
poor health outcomes lead to financial losses, which worsen the ability to combat physical and mental
health impairments, which in turn further deplete financial resources. Additionally, financial health is also
in and of itself an important component of a person’s health. Financial difficulties can cause stress that
contributes to or exacerbates psychological and physical ailments. NFL players suffer these outcomes as
well, despite their relatively high (but short-lived) compensation.
Before explaining the form and nature of compensation, it is important to discuss two concepts essential
to the leagues’ compensation structures: salary caps; and, free agency. After explaining these key terms,
we then discuss, for each league: (1) its respective salary cap; (2) rookie compensation; (3) veteran
compensation;
1208
(4) minimum, maximum, and average (mean) salaries; and, (5) guaranteed
compensation. At the conclusion of this Chapter, we provide a chart summarizing and comparing some of
the key compensation figures and policies across the leagues.
The Salary Cap
Generally, a “Salary Cap” in sports is the maximum amount of money that a club can spend on its’
players’ salaries collectively in a season.
1209
While some of the leagues use different terminology for their
Salary Cap, and there are various nuances and differences among them, each of the leagues has some
mechanism that restricts or reduces the amounts clubs can spend on player compensation. In each of the
leagues, the Salary Cap is negotiated with a corresponding labor organization, or players association, that
represents the players in negotiating the CBA. In the cases of the NFL, NBA, and NHL, the players
associations have agreed to the Salary Caps in exchange for a minimum percentage of league revenues
being spent on players. Moreover, in the cases of the NFL, NBA, NHL, and CFL, there is also a salary
floor—a minimum amount that the clubs must spend on player salaries. How player contracts are
calculated pursuant to these Salary Caps has a significant impact on the ways players are compensated in
each sport.
!
156!
Free Agency
MLB is the oldest of the leagues, having begun play in 1903.
1210
Beginning in the earliest days of
professional baseball and MLB, every player contract contained what is known as a “reserve clause.”
1211
The reserve clause prohibited players from negotiating with other clubs and granted the clubs an option to
renew the player’s contract on the club’s terms.
1212
If players wanted to play professional baseball, they
had almost no leverage in their contract negotiations.
The reserve clause raised concerns with the Sherman Antitrust Act. Section 1 of the Sherman Antitrust
Act prohibits contracts, combinations, or conspiracies that unreasonably restrain trade.
1213
The reserve
clause was an agreement among the separate baseball clubs not to negotiate with each other’s players and
thus potentially unreasonably restrained the labor market for players’ services. However, in 1922, in
Federal Baseball Club of Baltimore, Inc. v. National League of Professional Baseball Clubs (“Federal
Baseball”),
1214
the Supreme Court of the United States held that MLB was not engaged in interstate
commerce and was thus exempt from antitrust laws.
1215
As MLB grew into the large-scale, national business that it is today, the Supreme Court’s holding in
Federal Baseball seemed questionable, including to the Supreme Court itself. However, in 1953
1216
and
again in 1972,
1217
the Supreme Court upheld MLB’s antitrust exemption and the reserve clause on the
grounds of stare decisis.
1218
The Court reasoned that Congress had permitted MLB’s antitrust exemption
to stand for 50 years and that if anything were going to change, it had to be through legislation.
12191220
The other leagues were not as fortunate. The reserve clause was used in all of the Big Four leagues, but
the Supreme Court limited the antitrust exemption to baseball.
1221
Consequently, as a result of antitrust
litigation in the 1970s, the reserve clause was effectively eliminated in the NFL, NBA, and NHL.
1222
In
1976, MLB players finally were able to extinguish further use of the reserve clause through the
collectively bargained grievance process,
1223
and subsequent collective bargaining efforts.
Without the reserve clause, club owners became concerned that open bidding for players’ services would
financially ruin the leagues. Consequently, the leagues each began to negotiate with their respective
players unions. In 1976, MLB and the MLBPA, the NBA and NBPA, and the NHL and NHLPA all
agreed to new CBAs.
1224
In exchange for a variety of concessions, the players agreed to rules that
reflected the reserve clause’s intent: the clubs would be permitted to control a player’s rights for a certain
number of years, and then, after a player gained a certain level of experience, that player would become a
“free agent,” able to offer his services to any and all clubs at the highest price the market would bear. The
club’s ability to control the player for the first few years of his career is perhaps seen as fair consideration
for the club’s investment in the player’s development, particularly at any minor league level.
While the NFL and NFLPA did not agree to free agency as it existed in the other leagues until 1993,
1225
beginning in the 1970s free agency became and is an integral part of the modern sports landscape. Below,
we generically define three terms common to the concept of free agency in professional sports that are
key to understanding compensation in these leagues. While not all of the leagues use these exact terms,
they all utilize the concepts:
• Exclusive Rights Player: A player whose contract has expired and who, because he has minimal
experience (defined differently by the various leagues), must sign a contract with his prior club,
provided that club offers him a contract that meets the minimum requirements outlined in the
CBA. Exclusive Rights Players have no leverage and thus generally must accept the contract
offered by the club, which is typically for a salary at or near the league minimum.
!
157!
• Restricted Free Agent: A player whose contract has expired and who can sign a contract with
any club but, because the player has only a limited (but more than minimal) amount of experience
(defined variously among the leagues), if the player signs with a new club his prior club is
entitled to some form of compensation, typically draft picks. Further, the prior club has a right of
first refusal on a contract offered by another club as long as it had already made the player an
offer meeting certain minimum criteria outlined in the CBA (“Qualifying Offer”). Restricted Free
Agents have minimal leverage as clubs generally prefer not to pay the required compensation to
the player’s prior club.
• Unrestricted Free Agent: A player whose contract has expired and, because he has reached a
certain threshold of experience defined by the CBA, can sign a contract with any club without his
prior club retaining any rights concerning the player. Unrestricted Free Agents have far more
leverage and options as compared to Exclusive Rights Players or Restricted Free Agents.
Becoming an Unrestricted Free Agent is an important opportunity for players to offer their
services to any and all clubs at the highest price the market will bear (within the confines of the
CBA).
With these important concepts and terms in mind, we turn to analyzing how they are effectuated in the
leagues today and their effect on player health.
A. Compensation in the NFL
The most recent CBA agreed to by the NFL and the NFLPA was executed in 2011 and expires in 2021.
1. The NFL’s Salary Cap
NFL players, as a group, are entitled to different percentages of different revenue sources: (1) 55% of
League Media, which consists of all NFL broadcasting revenues;
1226
(2) 45% of NFL Ventures/Postseason
revenue, which includes all revenues arising from the operation of postseason NFL games and all
revenues arising from NFL-affiliated entities, including NFL Ventures,
1227
NFL Network,
1228
NFL
Properties,
1229
NFL Enterprises,
1230
NFL Productions,
1231
and NFL Digital;
1232
and, (3) 40% of Local
Revenues, which includes those revenues not included in League Media or NFL Ventures/Postseason, and
specifically includes revenues from the sale of pre-season television broadcasts.
1233
These revenues are
collectively known as “All Revenue” or “AR.”
1234
AR in 2017 is estimated to reach $14 billion.
1235
The
players’ share of AR cannot be less than 47% and cannot exceed 48.5%.
1236
The players’ share of AR—the Player Cost Amount
1237
—is one of two essential components for
calculating the Salary Cap.
1238
The other is Player Benefit Costs. Player Benefit Costs are the total
amounts the NFL and its clubs spend on programs and benefits for players, including retired players, in
addition to the costs of providing medical care to NFL players.
1239
The Salary Cap is determined by
subtracting Player Benefit Costs from the Player Cost Amount and dividing by the number of clubs in the
NFL.
1240
In other words, the Salary Cap equals Player Cost Amount minus Player Benefit Costs divided
by 32. Thus, the more that is paid to NFL players—including retired players—in the form of benefits and
medical care, i.e., Player Benefits Cost, the less they are able to receive in the form of salary. Indeed, in
2015, when the Salary Cap was $143,280,000 per club, each club was charged $37,550,000 in Player
Benefit Costs. Thus, out of a possible $180,830,000 that could have been spent on player salaries for each
club, 26.2% was allocated to player benefits.
!
158!
It is important to clarify these figures. As Figure 5-B shows below, about 50% of a club’s revenue is
allocated towards the players (the Player Cost Amount). The club keeps the other 50%. Of the 50%
allocated for the players, in 2015, 26.2% of that was used on player benefits. Thus, in 2015, we can
estimate that each club had approximately $361,660,000 in revenue, $180,830,000 of which would be
available for players. $37,550,000 was spent on player benefits. The $37,550,000 is 26.2% of the Player
Cost Amount and 10.4% of the club’s revenue.
In 2016, the NFL Salary Cap was $155.27 million.
1241
In 2017, the Salary Cap is $167 million.
1242
Importantly, the NFL’s Salary Cap is considered a “hard” Salary Cap in that, with some small exceptions
or nuances, there is no way for a club to exceed the Salary Cap.
1243
In exchange for the hard Salary Cap,
clubs individually must spend at least 89% of their Salary Cap in cash over a four-year period,
1244
and
collectively must spend 95% of their Salary Caps in cash over a four-year period.
1245
However, the Salary
Cap in one season includes prorated portions of signing and option bonuses paid in previous years, even
though no payment is actually made in the most recent season (see Section 4 below for additional
explanation). Consequently, a club’s Salary Cap figure does not represent the actual amount of money
being paid to the players. The cash requirement measures the amount of compensation actually being paid
and thus ensures that clubs are actually paying the players at least some threshold amount of money.
2. Rookie Compensation
Rookie compensation was a major issue during the 2011 CBA negotiations. For example, the 2010 first
overall Draft pick Sam Bradford agreed to a six-year, $78 million contract with the St. Louis Rams,
including $50 million guaranteed before he ever played a game in the NFL.
1246
By comparison, Tom
Brady, at the time a three-time Super Bowl champion and two-time league MVP, received only a four-
year, $72-million contract with $48.5 million guaranteed when he re-signed with the New England
Patriots prior to the 2010 season.
1247
With clubs—and, to some degree, players—unhappy with the
amounts being paid to unproven rookies, the terms regarding rookie compensation were changed
dramatically in the 2011 CBA.
1248
First, contracts for rookie players are now “fixed and unalterable.”
1249
First-round Draft picks are limited
to four-year contracts, with the club retaining the option to extend the contract for a fifth year.
1250
Rookies
drafted in rounds two through seven are limited to four-year contracts, and undrafted rookies can only
sign three-year contracts.
1251
Second, the amount of each rookie’s compensation is largely determined by each club’s Total Rookie
Allocation, i.e., how much a club can spend on its rookies (also known as the “Rookie Salary Cap”). Each
club’s Total Rookie Allocation is calculated based on the club’s amount, round, and position of Draft
picks.
1252
Thus each drafted player has a value within each club’s Total Rookie Allocation. Clubs and
contract advisors (i.e., agents) will not deviate much, if at all, from that assigned value in the total amount
of compensation provided to the player in his rookie contract.
1253
If one drafted player received more than
was allotted for his salary under the Total Rookie Allocation, it means another drafted player would have
to receive less than was allocated for his salary under the Total Rookie Allocation.
Third, a rookie’s compensation generally consists of three items: (1) the base or “Paragraph 5” Salary,
which is listed in Paragraph 5 of the Standard Player Contract; (2) a signing bonus, i.e., a lump sum paid
to the player shortly after signing the contract; and, (3) a Performance Incentive. The 2011 CBA
prohibited several types of contract structures and bonuses that had previously been used to inflate
rookies’ contracts.
1254
For most rookies, the signing bonus is the only portion of their compensation that is
guaranteed, as Paragraph 5 salaries are typically only guaranteed (in whole or in part) for first round Draft
picks.
1255
The Performance Incentive is typically earned only if a player participates in a certain number of
!
159!
the club’s plays and the club meets certain statistical performance criteria such as winning a certain
number of games.
1256
In spite of these changes, rookie compensation still varies dramatically. 2016 first overall pick Jared Goff
signed a four-year fully-guaranteed contract worth $27.9 million, including a $18.5 million signing
bonus.
1257
By contrast, the 253rd and final pick of the 2016 NFL Draft, Kalan Reed, signed a four-year
deal worth $2.4 million, including a $58,540 signing bonus.
1258
Only the signing bonus was
guaranteed.
1259
3. Veteran Compensation
A veteran’s compensation is typically determined by the new contract he signs when his existing contract
has expired or is approaching expiration. Upon expiration of a player’s contract, he meets one of three
definitions of a veteran in the NFL. The three different types of veterans are determined by the number of
Accrued Seasons a player has earned. Generally speaking, a player earns an Accrued Season for each
season he is on the club’s roster for six or more games.
1260
Importantly, a player earns an Accrued Season
for games missed as a result of a football-related injury.
1261
First, an Exclusive Rights Player is a player with less than three Accrued Seasons whose contract has
expired.
1262
An Exclusive Rights Player can only sign a contract with his prior club, provided the club
offers him a contract for at least the minimum permissible salary.
1263
Although drafted rookie contracts
are required to be four years in length, players’ contracts are often terminated before their expiration and
the players then sign new contracts with other clubs. If the contract with the new club expires before the
player has reached three Accrued Seasons, he will be an Exclusive Rights Player. There are dozens of
exclusive rights players every year, most of whom are simply battling to remain on the roster.
1264
Chris Banjo, a safety for the Green Bay Packers is a recent example of an Exclusive Rights Player. Banjo
was not selected in the 2012 NFL Draft, and was out of the NFL until signing with the Jacksonville
Jaguars prior to the 2013 season. When the Jaguars cut Banjo during the 2013 pre-season, he signed a
one-year deal with Green Bay for the league minimum. Banjo, as an Exclusive Rights Player, again
signed one-year deals with Green Bay for the league minimum prior to the 2014 and 2015 seasons.
1265
Second, players with exactly three Accrued Seasons and an expired contract are Restricted Free
Agents.
1266
A Restricted Free Agents can negotiate with other clubs but his prior club, provided it makes
an offer to the player, retains a right of first refusal and the right to receive Draft picks from the other club
as compensation. The round of the Draft pick to which the prior club is entitled varies depending on the
amount of money it offered the player.
1267
There were 74 Restricted Free Agents in the 2015 off-season
and 41 in the 2016 off-season.
Jermaine Kearse, a wide receiver for the Seattle Seahawks, is a recent example of a Restricted Free
Agent. Kearse signed with Seattle as an undrafted free agent prior to the 2012 season. After being
released by the club twice during the 2012 season, in October 2012 Kearse and the Seahawks agreed to a
contract for the 2012, 2013, and 2014 seasons. When Kearse’s contract expired after the 2014 season,
Kearse became a Restricted Free Agent. In the 2015 off-season, the Seahawks offered Kearse a one-year
contract worth $2,356,000, as they were required to do in order to retain their right of first refusal. Kearse
signed the contract.
1268
Third, a player with four or more Accrued Seasons whose contract has expired is an Unrestricted Free
Agent.
1269
An Unrestricted Free Agent is “completely free to negotiate and sign a Player Contract with
any Club, and any Club shall be completely free to negotiate and sign a Player Contract with such player
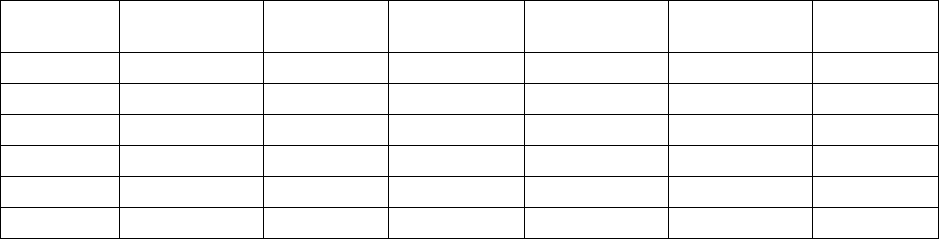
!
160!
without penalty or restriction[.]”
1270
There are typically around 400 Unrestricted Free Agents each off-
season.
A recent example of an Unrestricted Free Agent is Ndamukong Suh. Suh, a defensive lineman, was
selected second overall in the 2010 NFL Draft by the Detroit Lions and signed a five-year contract. When
Suh’s contract expired after the 2014 season, he was an Unrestricted Free Agent and signed a six-year,
$114 million contract with the Miami Dolphins.
1271
The nature of a player’s compensation varies considerably depending on his status. Exclusive Rights
Players typically have no leverage and thus generally must accept the contract offered by the club, which
is typically at or near the league minimum Paragraph 5 Salary (non-guaranteed). Similarly, Restricted
Free Agents typically have minimal leverage as clubs prefer not to pay the required compensation to the
prior club. Consequently, Restricted Free Agents ordinarily sign the contracts the clubs are required to
offer them to retain the right of first refusal. These contracts are non-guaranteed one-year contracts for
between $1.2 and $2.6 million per year.
1272
Unrestricted Free Agents have far more leverage and options. While less skilled Unrestricted Free Agents
might only sign contracts for the league minimum—if they are offered any contract at all—the best
players are able to sign multi-year deals worth tens of millions of dollars, including tens of millions of
dollars in guarantees.
1273
An Unrestricted Free Agent contract includes Paragraph 5 salary as well as many
different types of bonuses, such as a signing bonus; an option bonus (a lump sum paid in the event the
club or player opts to extend or alter the contract in some way); a roster bonus (a lump sum paid in the
event the player is still on the club’s roster at a determined date); and, a workout bonus (a lump sum paid
in the event a player participates in a minimum number of the club’s off-season workouts).
1274
In addition,
players’ contracts might include incentive clauses, which provide players with bonuses based on the
achievement of certain statistical accomplishments.
1275
Of course, players do not need to reach Unrestricted Free Agency to sign the types of contracts discussed
above. The fact that a player’s Unrestricted Free Agency is approaching often causes the player and his
club to negotiate a contract extension that is generally commensurate with what the player would have
received had he reached Unrestricted Free Agency.
1276
4. Minimum, Maximum, and Average (Mean) Salaries
NFL players’ minimum salaries are dependent upon their number of Credited Seasons. Generally, a
player earns a Credited Season (differentiated from an Accrued Season discussed above) when he is
entitled to be paid for at least three regular season games.
1277
Table 5-A below shows the minimum
Paragraph 5 salaries for players based on their number of Credited Seasons and the League Year.
1278
Table 5-A: NFL Minimum Paragraph 5 Salaries
Credited
Seasons
2015
2016
2017
2018
2019
2020
0
$435,000
$450,000
$465,000
$480,000
$495,000
$510,000
1
$510,000
$525,000
$540,000
$555,000
$570,000
$585,000
2
$585,000
$600,000
$615,000
$630,000
$645,000
$660,000
3
$660,000
$675,000
$690,000
$705,000
$720,000
$735,000
4–6
$745,000
$760,000
$775,000
$790,000
$805,000
$820,000
7–9
$870,000
$885,000
$900,000
$915,000
$930,000
$945,000

!
161!
10+
$970,000
$985,000
$1,000,000
$1,015,000
$1,030,000
$1,045,000
The minimum salary is particularly important as nearly half of the players in the NFL only make the
league minimum.
1279
The NFL does not prescribe a maximum salary. However, the Salary Cap and its complicated rules create
barriers that effectively restrict player salaries. For example, when a player receives a signing bonus, even
though the signing bonus is typically paid in one or two lump sums shortly after the contract is executed,
only a portion of the signing bonus counts against the Salary Cap for the year in which the bonus was
paid. For Salary Cap purposes, the signing bonus is prorated equally over the duration of the contract.
1280
Thus, if a player receives an $8 million signing bonus as part of a four-year contract, the signing bonus
will count against the Salary Cap for $2 million each year ($8 million divided by 4 years). However, a
signing bonus can only be prorated over a maximum of five years.
1281
Clubs thus generally prefer not to
sign a player to a contract longer than five years to avoid losing the full benefit of proration.
The concept of an “average” salary in the NFL can be confusing. As discussed above, players often
receive a significant portion of their compensation in upfront lump sum payments and then are paid less
during the remainder of the contract. For example, when Unrestricted Free Agent Ndamukong Suh signed
a six-year, $114 million contract with the Miami Dolphins in 2015, he received a $25.5 million signing
bonus in the first year but his Paragraph 5 salaries for the remainder of the contract averaged $17.16
million.
1282
Thus, it is unclear when the media is reporting “average” salary whether they are calculating
that figure based on the compensation a player will receive in that particular season, or on the average
amount owed to the player over the duration of the contract. Additionally, the details of NFL player
contracts are typically not public, further calling into question the reliability of the data reported by the
media.
In the NFL community, clubs and contract advisors (i.e., agents) generally think of a player’s salary in
terms of the Average Per Year (“APY”). The APY is determined by dividing the contract’s total
compensation by its length. While there are nuances that might call into question whether to include
certain years or forms of compensation in the calculation, the APY is generally a useful method for
understanding the compensation provided to a player pursuant to a contract.
Based on our analysis, the website spotrac.com provides the most reliable publicly available data on
player contracts. Using data from spotrac.com from the second week of the 2015 regular season, the
average NFL player had a contract that was approximately 2.9 years in length and worth approximately
$7.6 million total, or about $2.7 million per year. The median APY was approximately $710,000, and
about 61% of the players had an APY of less than $1 million.
The value or duration of an NFL player contract is less meaningful when considering that NFL contracts
are generally not guaranteed.
5. Guaranteed Compensation
Guaranteed compensation in the NFL is a complicated issue. Many people—particularly some players—
feel that fully guaranteeing a player’s contract is a fair trade for the health risks players undertake. More
important for our purposes here, focused on protecting and promoting player health, if a player’s contract
were fully guaranteed, he would likely feel less pressure to play through injuries in an effort to
continually prove himself to the club and avoid termination of his contract.
1283
However, we have
concerns about the possibility of unintended consequences as well as the feasibility of fully guaranteeing
!
162!
player compensation, which will be discussed in detail in the Analysis and Recommendation Sections
below.
To understand these concerns, in this Section we provide an explanation of guaranteed compensation in
the NFL. Generally, NFL clubs are permitted to terminate a player’s contract without any further financial
obligation to the player for five reasons:
(1) the player “has failed to establish or maintain [his] excellent physical
condition to the satisfaction of the Club physician”;
(2) the player has “failed to make a full and complete disclosure of [his]
physical or mental condition during a physical examination”;
(3) “[i]n the judgment of the Club, [the player’s] skill or performance has
been unsatisfactory as compared with that of other players competing for
positions on the Club’s roster”;
(4) the player has “engaged in personal conduct which, in the reasonable
judgment of the Club, adversely reflects on the Club”; and,
(5) “[i]n the Club’s opinion, [the player is] reasonably anticipated to
make less of a contribution to the Club’s ability to compete on the
playing field than another player or players whom the Club intends to
sign or attempts to sign, or already on the roster of the Club, and for
whom the Club needs Room.”
1284
Players and their contract advisors seek to curtail the clubs’ termination rights as to individual players by
negotiating for some of the player’s compensation to be guaranteed in addendums to the Standard Player
Contract. Guaranteed compensation takes a wide variety of forms (most notably in signing bonuses),
1285
but generally players and their contract advisors seek to guarantee the player’s contract even where he is
terminated for “injury,” “skill,” or “Salary Cap.” An “injury” guarantee will protect against the first
reason listed above for which clubs can generally terminate a player’s contract; a “skill” guarantee will
protect against the third reason; and, a “Salary Cap” guarantee will protect against the fifth reason. A
player might have all or just some seasons of his contract guaranteed for skill, injury, and/or Salary Cap.
In addition, there are other mechanisms in the CBA which can effectively guarantee some or all of a
player’s salary, including Injury Protection
1286
and Termination Pay.
1287
Generally, players and their contract advisors seek to obtain as much guaranteed money as possible in
contract negotiations. Guaranteed compensation provides the player with a secure income that is
otherwise typically threatened by injury. However, there are times when a player might not want to sign
the contract that offers him the most money—guaranteed or unguaranteed. Younger players might eschew
the last year or two of a contract and the money that comes with it in favor of a shorter contract. In doing
so, the player is hoping or expecting that he will be able to complete the shorter contract, reenter the free
agency market, and sign another contract. Such decisions are obviously risky—the player’s career might
end for skill or health reasons under the shorter contract and the player will never have another chance at
another contract. However, if the player is healthy, securing a second free agent contract can be lucrative.
From a club’s perspective, guaranteed compensation is something to be avoided. Guaranteeing all or a
portion of a player’s contract commits the club to a player financially, regardless of whether the player
performs poorly or suffers a career threatening injury. Nevertheless, clubs regularly agree to guarantee
compensation to players to persuade them to join or stay with the club.
!
163!
Changes to the Salary Cap rules as part of the 2011 CBA potentially increased the use of guaranteed
money. Technically, whether a player’s compensation is guaranteed has no effect on the Salary Cap—a
club is limited to a certain amount of player compensation costs regardless of whether that amount is
guaranteed or unguaranteed. Importantly, the amount of player salary that is counted against a club’s
Salary Cap does not necessarily reflect the amount actually being paid to players. As a result of the Salary
Cap’s accounting rules, in any given year a significant portion of a club’s Salary Cap allocation might be
consumed by charges that do not actually reflect a payment being made from the club to players, such as
prorated portions of a signing bonus paid in a prior year. However, the 2011 CBA addressed this
discrepancy by adding a requirement that clubs spend a certain amount of the Salary Cap in cash, that is,
actual payments to the players, regardless of the accounting rules. Probably the easiest way for a club to
ensure that it spends a sufficient amount in cash is to pay lump sum signing bonuses. Signing bonuses are
the most traditional form of guaranteed compensation.
Using the same data from spotrac.com discussed above, one finds that approximately 44% of all
contracted compensation is guaranteed. The data also shows that approximately 70% of players had at
least some guaranteed compensation in their contract and the average amount of guaranteed compensation
in an NFL player contract was $3.4 million. Additionally, 251 players had a contract that included at least
$10 million in guaranteed compensation and 740 players had a contract that included at least $1 million in
guaranteed compensation.
In recent years, the percentage of an NFL player’s contract that is guaranteed appears to have risen.
Although the scope of the guarantees is sometimes debated,
1288
it is not uncommon for marquee players to
sign contracts that guarantee 50% or more of their compensation.
1289
Moreover, the 2011 CBA
significantly curtailed rookie compensation, cutting the amount top Draft picks earned by more than
50%.
1290
In exchange, however, many first round Draft picks’ contracts are now fully guaranteed.
1291
There is also an important caveat to the guaranteed nature of the various bonuses players receive. The
bonuses are almost always subject to proportional forfeiture or voiding if a player violates the contract in
some way, such as by refusing to show up to training camp, failing a test under the NFL’s Policy and
Program on Substances of Abuse (“Substance Abuse Policy”), failing a test under the NFL’s Policy on
Performance-Enhancing Substances (“PES Policy”),
1292
or otherwise engaging in conduct detrimental to
the NFL or the club.
1293
For example, if a player received a $10 million signing bonus for a five-year
contract, and the player later refuses to report to the club for the fifth season in hopes of signing a more
lucrative contract, the player could be required to return $2 million of the signing bonus to the club.
1294
Similarly, if a player is entitled to have his Paragraph 5 salary guaranteed in his second season, but fails a
drug test between the first and second seasons, the contract might contain a clause permitting the club to
void the guarantee in the second season.
1295
With the structure of compensation in the NFL explained above, we are ready to compare it to the other
leagues.
B. Compensation in MLB
The most recent CBA agreed to by MLB and the Major League Baseball Players Association (“MLBPA”)
was executed in 2016 and expires in 2021.
1. MLB’s Tax Threshold
Unlike the NFL, MLB does not have a “Salary Cap” for its clubs, insofar as there is no maximum amount
that clubs can spend on player salaries. Instead, MLB sets a Tax Threshold and applies a “Competitive
!
164!
Balance Tax” for compensation paid to players over that amount. For the 2016 season, the Tax Threshold
was set at $189 million,
1296
and will be $195 million in 2017.
1297
This tax is also known as the “luxury tax”
and is intended to encourage parity by forcing clubs not to exceed the Tax Threshold. The Competitive
Balance Tax ranges from 20% to 50% depending upon how many times the club has previously exceeded
the Tax Threshold.
1298
In 2016, MLB revenues were an estimated $10 billion.
1299
2. Rookie Compensation
Rookies generally are paid the league minimum and have one-year contracts, as will be explained further
below.
1300
3. Veteran Compensation
The 2012 MLB CBA and uniform player contract (“UPC”) divide players into three categories based on
the amount of time they have spent in the major leagues, and which category a player falls into has
important consequences for his salary. A player’s time in the major leagues is tracked by a metric known
as Major League Service Time (“MLST”). A player accumulates one day of MLST for “each day of the…
season [he] is on a Major League Club’s Active List.” One season of MLST is defined as 172 days.
1301
A player with less than three years of MLST is bound to his club by the terms of the UPC, which contains
a reserve clause that effectively allows the club to unilaterally retain his services so long as it pays him
the minimum salary set in the CBA.
1302
A player in this position is said to be “under reserve” to his club,
and has essentially no leverage to influence his base salary—he can either accept his club’s offer (almost
certainly for a salary at or very near the minimum allowed by the CBA), attempt to hold out for higher
pay, or find an occupation outside of MLB.
1303
As a result, skilled players under reserve to their clubs are
paid far less than they would be in an open market for their services.
1304
A player with more than three years but less than six years of MLST is said to be “arbitration eligible,”
and has the right under the CBA to submit the issue of his salary to an arbitration panel, with or without
the consent of his club.
1305
Certain players with more than two but less than three years of MLST are also
arbitration eligible.
1306
These players, known as “Super Two” players, must have accumulated 86 days of
MLST in the immediately preceding season and rank in the top 22% in total MLST among all players
eligible for Super Two consideration.
1307
If an arbitration-eligible player initiates arbitration, he and his club must exchange single-year salary
figures with one another
1308
and submit those figures to a salary arbitration panel consisting of three
arbitrators jointly selected by the MLBPA and MLB.
1309
Salary arbitration proceedings are summary and
winner-take-all: each side has just 90 minutes to argue
1310
for its proposed salary,
1311
and the salary
arbitration panel may award the player a single-year contract for either the proposed salary he submitted
or the proposed salary the club submitted—it may not award any other figure.
1312
This form of arbitration,
also known as pendulum or final offer arbitration, forces the sides to submit reasonable figures in the
hopes that the arbitrator believes their submission is closer to the player’s value than the other side’s
submission.
1313
As a result, approximately 90% of all salary arbitration cases settle before a hearing.
1314
In
effect, the salary arbitration mechanism permits players to receive their free market wages for one season
without the ability to actually negotiate with other clubs.
A player with more than six years of MLST at the completion of the term of his contract becomes a free
agent and is able to offer his services to any and all clubs at whatever price the market will bear.
1315
In
veteran free-agency contracts, there is often a trade-off between contract length and average annual
!
165!
compensation.
1316
Due to risks of injury or performance drop-offs, a player might accept a lower average
annual compensation in exchange for higher total compensation in a longer contract.
1317
MLB’s three-tiered system is similar to the NFL’s use of Exclusive Rights Players, Restricted Free
Agents, and Unrestricted Free Agents. In both leagues, players gain more rights and compensation with
experience.
Most MLB free agents obtain contracts that are short in duration. The share of one-year free agent
contracts signed in each of the seasons from the 2007 season to the 2013 season, for example, has ranged
from 51.43% to 76.52%, and the share of two-year free-agent contracts has ranged from 13.08% to
27.62%.
1318
Between 2007 and 2014, only the 2013 free agency market had more than 20% of free agent
contracts extend beyond three years.
1319
Though most free agents are only able to obtain short-term deals, superstars have been able to bargain for
extremely lucrative long-term contracts. For example, in 2014, the Miami Marlins signed Giancarlo
Stanton, a then-twenty-five-year-old right fielder, to a thirteen-year, $325 million contract,
1320
breaking
the previous record held by the Detroit Tigers infielder Miguel Cabrera’s ten-year $292 million deal.
1321
MLB clubs are thought to have deployed two strategies to minimize players’ opportunities to obtain large
free-agent contracts.
First, clubs have kept star prospects in the minor leagues for a few weeks at the beginning of their rookie
season before having the player join the major league roster. This plan prevents the young player from
achieving the necessary number of days on the roster to accrue a full season of MLST, thus delaying the
player’s free agency by a year.
1322
For example in 2015, the Chicago Cubs waited 11 days before calling
up star rookie third baseman Kris Bryant.
1323
By doing so, Bryant will not be a free agent until after the
2021 season.
1324
Had Bryant started the season with the Cubs, he would be eligible for free agency after
the 2020 season.
1325
Second, clubs have signed players to long-term contract extensions at reduced salaries years before the
player reaches free agency or is salary arbitration eligible.
1326
For example, in 2012, the Pittsburgh
Pirates’ star center fielder Andrew McCuthen had played two seasons and was a year away from being
salary arbitration eligible—and thus likely earning a multi-million dollar salary commensurate with
players of similar skill. Rather than go through salary arbitration in future years and have McCutchen
potentially reach free agency, the Pirates signed McCutchen to a six-year contract worth $51.5 million,
plus a seventh-year at the club’s option for $14.75 million.
1327
The contract means the Pirates control
McCutchen’s rights through his ninth season—three years after when he would have become a free agent
if not for the long-term extension. For McCutchen, the long-term extension provides him long-term
financial security when he otherwise would have been playing on year-to-year contracts until he reached
free agency. As for any player, there was no guarantee that McCutchen would have continued to be
sufficiently healthy and productive to reach free agency and receive a long-term multi-million dollar
contract.
4. Minimum, Maximum, and Average (Mean) Salaries
In 2016, the mean MLB salary was $4.4 million per year,
1328
and the minimum salary was $507,500.
1329
There is no maximum salary for MLB players.
Simple averages are not entirely revealing due to the fact that younger players are limited in their ability
to obtain market wages by MLB’s free agency and salary arbitration rules. Data on the distribution of
!
166!
average annual salaries in 2012 indicate that high salaries are concentrated among a relatively small
number of the league’s players according to the following distribution:
1330
Bottom 20%: $481,593 (The minimum 2012 salary was $480,000)
Second 20%: $505,109
Third 20%: $1,195,785
Fourth 20%: $3,606,888
Top 20%: $11,164,616
Top 5%: $18,363,670
Top 1%: $23,791,667
1331
5. Guaranteed Compensation
Unlike the NFL, MLB contracts are generally understood to be fully guaranteed.
1332
According to
Paragraph 7 of the UPC, clubs may terminate a player’s contract if the player shall at any time:
(1) fail, refuse, or neglect to conform his personal conduct to the standards
of good citizenship and good sportsmanship or to keep himself in first-
class physical condition or to obey the Club’s training rules; or
(2) fail, in the opinion of the Club’s management, to exhibit sufficient skill
or competitive ability to qualify or continue as a member of the Club’s
team; or
(3) fail, refuse or neglect to render his services hereunder or in any other
manner materially breach this contract.
However, in practice, Paragraph 7 is usually nullified in the contracts of any player other than those with
minimal MLST or veterans with little to no leverage. Thus, MLB clubs generally cannot terminate a
player’s contract, i.e., MLB player contracts are generally guaranteed.
C. Compensation in the NBA
The most recent CBA agreed to by the NBA and the National Basketball Players Association (“NBPA”)
was executed in 2017, takes effect on July 1, 2017, and expires in 2024. However, both parties have the
option of terminating the CBA after the 2022–23 season by serving written notice of the exercise of such
option by December 15, 2022.
1333
1. The NBA’s Salary Cap
NBA players are collectively entitled to approximately 50% of Basketball Related Income (“BRI”).
1334
BRI is “the aggregate operating revenues… received or to be received…” by the NBA, NBA Properties,
Inc., NBA Media Ventures, LLC and any subsidiaries.
1335
The NBA’s Salary Cap is determined by
multiplying BRI by 44.74%, subtracting player benefit costs, and dividing by the number of clubs.
1336
The
Salary Cap for the 2016–2017 season is $94.143 million,
1337
and is expected to be $102 million in 2017–
18.
1338
The NBA’s Salary Cap is in the process of considerable growth due to new multi-billion dollar
television contracts for the NBA.
1339
Each club is required to pay its players a total of at least 90% of the
Salary Cap each year.
1340
The NBA’s 2016–17 revenues are projected to be an estimated $8 billion.
1341
Unlike the NFL’s “hard” Salary Cap, the NBA’s Salary Cap is considered “soft,” because there are
multiple exceptions that permit clubs to exceed the Salary Cap. These exceptions will be discussed below
in detail in Section 3: Veteran Compensation.
!
167!
In addition to the Salary Cap, the NBA also has a Tax Level. The Tax Level is a threshold for a club’s
player salaries that is above the Salary Cap. While the 2016–17 Salary Cap was $94.143 million, the Tax
Level was $113.287 million.
1342
The Tax Level is expected to rise to $122 million in 2017–18.
1343
If clubs
exceed the Tax Level, they must pay the league a graduated tax based on how much they have exceeded
the Tax Level.
1344
The Tax Levels increase if the club has exceeded the Tax Level in three or more of the
previous four seasons (i.e., a “Repeater”).
1345
Up to 50% of the total tax payments may be distributed, at
the NBA’s option, to non-taxpaying clubs, and amounts not distributed to non-taxpaying clubs can be
used for other league purposes.
1346
If a club’s total salaries are higher than the Salary Cap but lower than
the Tax Level, e.g., $100 million in 2016–17, the club would not make a tax payment.
Table 5-B: NBA Tax Levels (Non-Repeater)
Incremental Club Salary Above Tax Level
Tax Rate for Increment
$0–$4,999,999
$1.50 for $1
$5,000,000–$9,999,999
$1.75 for $1
$10,000,000–$14,999,999
$2.50 for $1
$15,000,000–$19,999,999
$3.25 for $1
$20,000,000 and over
Tax rates increase by $0.50 for each additional
$5,000,000 increment above the Tax level (e.g., for
Team Salary $20,000,000 to $24,999,999 above the
Tax level, the Tax rate is $3.75-for-$1 for that
increment).
Table 5-C: NBA Tax Levels (Repeater)
Incremental Club Salary Above Tax Level
Tax Rate for Increment
$0–$4,999,999
$2.50 for $1
$5,000,000–$9,999,999
$2.75 for $1
$10,000,000–$14,999,999
$3.50 for $1
$15,000,000–$19,999,999
$4.25 for $1
$20,000,000 and over
Tax rates increase by $0.50 for each additional
$5,000,000 increment above the Tax level (e.g., for
Team Salary $20,000,000 to $24,999,999 above the
Tax level, the Tax rate is $4.75-for-$1 for that
increment).
In 2015–16, seven NBA clubs exceeded the Tax Level and were required to pay a tax, with the Cleveland
Cavaliers paying the most at approximately $54 million.
1347
2. Rookie Compensation
The NBA Draft has two rounds. The initial contract entered into by a first round NBA Draft pick and the
club that drafts the player is called a Rookie Scale Contract.
1348
Rookie Scale Contracts must cover two
seasons, with a club option for the third and fourth seasons.
1349
Clubs must exercise the option for the
third season by October 31 following the player’s first season and must exercise the option for the fourth
season by the October 31 following the player’s second season.
1350
The values of these contracts can be
negotiated between 80% to 120% of the Rookie Scale, agreed to by the NBA and NBPA. There is a
different Rookie Scale for each year of the CBA, with values increasing or decreasing annually at the
same rate as any increase or decrease in the Salary Cap. The first pick in the NBA Draft is given the
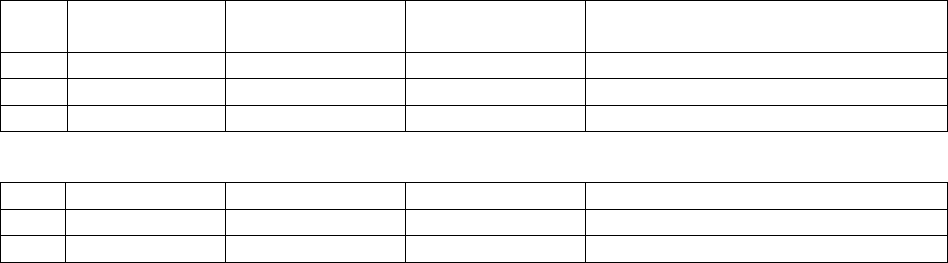
!
168!
greatest Rookie Scale amount, with each subsequent pick receiving a lesser Rookie Scale amount. For
illustrative purposes, the Rookie Scale amounts for the first and last three first round NBA Draft positions
for the 2017–2018 season are as follows
1351
:
Table 5-D: Sample of NBA Rookie Scale (2017–2018)
Pick
1st Year
Salary
2nd Year Salary
3rd Year Salary
4th Year Option (Percentage
Increase over 3rd Year Salary)
1
$5,855,200
$6,949,900
$8,121,000
26.1%
2
$5,238,800
$6,218,300
$7,266,100
26.2%
3
$4,704,500
$5,584,000
$6,525,000
26.4%
***
28
$1,179,100
$1,399,600
$1,635,300
80.5%
29
$1,170,500
$1,389,300
$1,623,400
80.5%
30
$1,162,100
$1,379,300
$1,611,800
80.5%
Second round Draft picks do not operate under any scale. They may sign for any amount at or above the
minimum salary.
1352
Second round Draft picks, however, generally only command a minimum salary or
an amount slightly above the minimum.
1353
Initial contracts for second-round Draft picks are commonly
one, two, or three years in length.
1354
Similar to the NBA, NFL rookie contracts operate on a scale based on the Total Rookie Allocation.
However, the NFL rookies’ salaries are not collectively bargained in the way the NBA’s rookies’ salaries
are.
3. Veteran Compensation
As in the NFL, there are two types of free agency in the NBA: unrestricted and restricted.
1355
Unrestricted
Free Agents are able to sign with any club after their prior contract has terminated and there is nothing
that the player’s prior club can do to prevent him from signing with a new club.
1356
Players become
Restricted Free Agents only in limited circumstances: (1) following the fourth year of a player’s Rookie
Scale Contract; and, (2) for non-first round picks, when the player’s contract has expired and he has been
in the NBA for three or fewer seasons.
13571358
In order to make a player who meets these qualifications a
Restricted Free Agent, the club for which the player last played must make the player a one-year
Qualifying Offer.
1359
The value of the Qualifying Offer is based on, among other things, the player’s Draft
position.
1360
The Restricted Free Agent may choose to accept the club’s Qualifying Offer. In most cases, if he accepts
the Qualifying Offer, the player would become an Unrestricted Free Agent after he completes the one-
year Qualifying Offer contract. If he does not want to sign a contract with the club for which he last
played, the player may sign an offer sheet (which includes principal terms such as base salary, number of
years, and signing bonus) with another club.
1361
The offer sheet must be for more than two seasons.
1362
The player’s prior club then has a right of first refusal for a two-day period.
1363
If the player’s prior club
exercises its right of first refusal, then the player will be under contract with his prior club under the
principal terms of the offer sheet.
1364
If the prior club does not match the terms of the offer sheet and the
player joins a new club, the prior club does not receive any compensation for the loss of the player. In
contrast, in the NFL, clubs that lose Restricted Free Agents are awarded compensatory draft picks
depending on the amount of the player’s new contract.
!
169!
As mentioned above, there are exceptions to the Salary Cap. While there are ten different exceptions,
1365
we list here the most important ones (as summarized by the NBA with minor clarifying edits):
1366
1. Qualifying Veteran Free Agent (“Bird”) Exception:
1367
A team may
re-sign its own free agent to a first-year salary of up to the maximum
player salary if he played for the team for some or all of each of the prior
three consecutive seasons (or, if he changed teams, he did so by trade).
2. Early Qualifying Veteran Free Agent (“Early Bird”) Exception: A
team may re-sign its own free agent to a first-year salary of up to the
greater of (a) 175% of the player’s salary in the last season of his prior
contract; or, (b) 105% of the average NBA player salary for the prior
season, if he played for the team for some or all of each of the prior two
consecutive seasons (or, if he changed teams, if he did so by trade or by
assignment via the NBA’s waiver procedures). A contract signed using
the Early Bird Exception must be for at least two seasons.
3. Non-Taxpayer Mid-Level Salary Exception:
(a) A team may use the Non-Taxpayer Mid-Level Salary Exception to
sign one or more players to contracts with first-year salaries that, in
the aggregate, provide for a total up to $8.406 million in 2017–18
(the Exception amount grows annually by the same amount as the
Salary Cap).
(b) Contracts signed under the Non-Taxpayer Mid-Level Salary
Exception can cover up to four seasons.
(c) A team can use the Non-Taxpayer Mid-Level Salary Exception to re-
sign its own free agent (as well as to sign another team’s free agent),
but cannot use this Exception to acquire a player by assignment.
4. Minimum Salary Exception: A team may sign a player to a one-year or
two-year contract at the applicable minimum player salary (prorated as
appropriate for a 10-Day or Rest-of-Season contract). This Exception
may also be used to acquire by assignment a player who was signed to a
one-year or two-year minimum contract.
The Bird and Early Bird Exceptions are the most significant. These exceptions permit clubs to resign their
best players for maximum or close to maximum salaries without regard to the Salary Cap. If other clubs
wanted to sign these players to maximum contracts, those contracts would count against the Salary Cap.
These rules provide a clear advantage to a player’s prior club in free agency negotiations.
In contrast, the NFL’s Salary Cap has no meaningful exceptions.
1368
4. Minimum, Maximum, and Average (Mean) Salaries
The minimum salary in the NBA depends on the player’s experience level and increases each season. The
minimum salaries for the 2016–17 season (under the 2011 CBA)
1369
and the 2017-18 season (under the
2017 CBA)
1370
are as follows:
!
170!
Table 5-E: NBA Minimum Salaries
Years of Service
2016–17 (2011 CBA)
2017–18 (2017 CBA)
0
$543,471
$815,615
1
$874,636
$1,312,611
2
$980,431
$1,471,382
3
$1,015,696
$1,524,305
4
$1,050,961
$1,577,230
5
$1,139,123
$1,709,538
6
$1,227,286
$1,841,849
7
$1,315,448
$1,974,159
8
$1,403,611
$2,106,470
9
$1,410,598
$2,116,995
10+
$1,551,659
$2,328,652
Unlike the NFL, the NBA CBA includes limits on player salaries. A player who has completed fewer than
seven Years of Service
1371
has a maximum annual salary of 25% of the Salary Cap at the time of contract
execution or 105% of the Salary for the final season of his prior contract, whichever is greater.
1372
However, a player who has four Years of Service at the end of his Rookie Scale Contract, or a second-
round pick or undrafted player who has four Years of Service following the end of the last season covered
by his contract is eligible to receive, from his prior club only, 30% of the Salary Cap in effect at the time
of contract execution, provided that the player has (i) been named twice to an All-NBA first, second, or
third team or named Defensive Player of the Year, in the immediately preceding season or in two seasons
during the immediately preceding three seasons, or (ii) been named as NBA MVP at least once during the
preceding three seasons.
1373
A Player who has at least seven but less than ten Years of Service has a maximum annual salary of 30%
of the Salary Cap in effect at the time of contract execution or 105% of the Salary Cap for the final season
of his prior contract, whichever is greater.
1374
A player with ten or more Years of Service has a maximum
annual salary of 35% of the Salary Cap in effect at the time of contract execution or 105% of the Salary
for the final season of his prior contract, whichever is greater.
1375
The 2017 CBA introduced an important exception to the rule limiting players with at least seven but less
than ten Years of Service to 30% of the Salary Cap. Under the 2017 CBA,
a player who has eight (8) or nine (9) Years of Service at the time the
Contract is executed and rendered such Years of Service for the Team
with which he first executed a Player Contract (or, if he was under a
Player Contract for more than one Team during such period, changed
Teams only by trade during the first four (4) Salary Cap Years in which
he was under a Player Contract) shall be eligible to enter into a
Designated Veteran Player Contract pursuant to which he receives from
his Prior Team up to thirty-five percent (35%) of the Salary Cap in effect
at the time the Contract is executed (the “Designated Veteran Player 35%
Max Salary”) if the player has met at least one of the following criteria at
the time his Contract is executed: (i) the player was named to the All-
NBA first, second, or third team, or was named Defensive Player of the
Year, in the immediately preceding Season or in two (2) Seasons during
the immediately preceding three (3) Seasons; or (ii) the player was
!
171!
named NBA MVP during one of the immediately preceding three (3)
Seasons (the “Designated Veteran Player 35% Max Criteria”).
1376
The Designated Veteran Player rule was reportedly introduced in response to 2014 NBA MVP Kevin
Durant leaving his original team, the Oklahoma City Thunder, for the Golden State Warriors prior to the
2016-17 season.
1377
Had the rule existed at the time, the Thunder would have been able to offer Durant a
contract with a higher annual salary than the Warriors which might have enticed him to stay with the club.
The mean annual salary in the NBA for the 2016–2017 NBA season is between $6.9 million and $8
million,
1378
much more than the $2.7 mean salary for an NFL player. The median salary in the NBA for
the 2016–2017 NBA season is between $4 million and $5 million. In 2016–17, the largest guaranteed
contract in the NBA was Mike Conley’s five-year deal worth $140,529,829 in gross value.
1379
It is worth
noting that NBA players generally have higher salaries than players in other professional sports leagues
due, at least in part, to the fact that NBA rosters are much smaller. An NBA club’s active roster is 12-13
players
1380
while NFL active rosters are 46 players,
1381
MLB active rosters are 25 players
1382
and NHL
active rosters are 23 players.
1383
Also unlike the NFL, the NBA CBA limits a veteran player’s contract length. The default rule in the CBA
is that a player contract may cover up to but no more than four seasons in length.
1384
However, there are
several instances where the CBA deviates from the default rule. For example, a player contract between a
Qualifying Veteran Free Agent and his prior club may cover up to but not more than five seasons and an
extension of a Rookie Scale Contract may cover up to but no more than five seasons.
1385
The mean
contract length in the NBA during the 2016-17 season was 3.1 years.
1386
In sum, the contract rules provide significant advantages to a player’s prior club. The prior club can offer
a contract longer than other clubs and not have that contract count against the club’s Salary Cap. In
addition, players who have reached certain milestones, (such as All-NBA teams or MVP awards), are able
to be paid a higher percentage of the Salary Cap by their prior club than by a new club. It is thus not
surprising that the ten largest contracts in the NBA during the 2016–17 season were all contracts signed
between a player and his existing club.
1387
5. Guaranteed Compensation
The NBA Uniform Player Contract (“UPC”) permits NBA clubs to terminate a player’s contract if the
Player shall:
(i) at any time, fail, refuse, or neglect to conform his personal conduct to
standards of good citizenship, good moral character (defined here to
mean not engaging in acts of moral turpitude, whether or not such acts
would constitute a crime), and good sportsmanship, to keep himself in
first class physical condition, or to obey the Team’s training rules;
(ii) at any time commit a significant and inexcusable physical attack against
any official or employee of the Team or the NBA (other than another
player), or any person in attendance at any NBA game or event,
considering the totality of the circumstances, including (but not limited
to) the degree of provocation (if any) that may have led to the attack, the
nature and scope of the attack, the Player’s state of mind at the time of
the attack, and the extent of any injury resulting from the attack;
!
172!
(iii) at any time, fail, in the sole opinion of the Team’s management, to
exhibit sufficient skill or competitive ability to qualify to continue as a
member of the Team….; or
(iv) at any time, fail, refuse, or neglect to render his services hereunder or in
any other manner materially breach this Contract.
1388
However, the CBA permits clubs and players to agree to “compensation protection,” i.e., a guarantee of a
player’s contract in five circumstances, in the event of the player’s: lack of skill; death; basketball-related
injury; injury or illness; and, mental disability.
1389
Compensation protections are negotiated terms in each
player contract. However, the CBA requires that compensation protection be given in many
circumstances. For sign-and-trade contracts,
1390
the first season of the contract must be protected for lack
of skill.
1391
For Rookie Scale Contracts, all seasons must be protected for lack of skill and injury/illness
for at least 80% of the player’s Base Compensation.
1392
Qualifying Offers made to a Restricted Free Agent
must be protected for lack of skill and injury/illness.
1393
Nevertheless, “[i]n practice, the majority of NBA
contracts (especially for established veterans) are fully guaranteed. Non-guaranteed salary is most often
used for fringe players (either at the beginning or end of their careers) or for the later years of long-term
contracts (often in conjunction with benchmarks that allow the salary to become fully guaranteed over
time).”
1394
Data from spotrac.com gathered during January 2017 shows that 97.3% of NBA player
compensation contracted for at that time was guaranteed,
1395
as compared to about 44% of NFL player
compensation.
While the NBA restricts clubs and players to compensation protection in just five scenarios, the NFL
CBA does not limit the types of guarantees players and clubs can negotiate. Nevertheless, in practice,
NFL contracts are generally only guaranteed against skill, injury, and Salary Cap. The fact that contracts
in the NBA tend to be guaranteed more than those in the NFL is most likely a reflection of the leverage of
the players in contract negotiations over time.
D. Compensation in the NHL
The most recent CBA agreed to by the NHL and National Hockey League Players Association
(“NHLPA”) was executed in 2013 and expires in 2022. In September 2019, both parties have the option
of terminating the CBA, effective September 2020.
1396
1. The NHL’s Salary Cap
NHL players are collectively entitled to 50% of Hockey Related Revenues (“HRR”).
1397
Generally
speaking, HRR “means the operating revenues… from all sources, whether known or unknown, whether
now in existence or created in the future,… of each Club or the [NHL],… derived or earned from, relating
to or arising directly or indirectly out of the playing of NHL hockey games or NHL-related events in
which current NHL Players participate or in which current NHL Players’ names and likenesses are
used[.]”
1398
The NHL’s 2015–16 revenues were an estimated $4.1 billion.
1399
The NHL’s Salary Cap structure includes both an Upper Limit and Lower Limit on club payrolls. To
determine the Upper and Lower Limits, the parties multiply HRR by 50%, subtract player benefit costs,
and then divide by the 30 NHL clubs to reach a midpoint.
1400
The Lower Limit is reached by multiplying
the midpoint by 85% and the Upper Limit is reached by multiplying the midpoint by 115%.
In the 2016–17 season, the Lower Limit is $54 million and the Upper Limit is $73 million.
1401
Finally, the
NHL’s Salary Cap is considered “hard,” because there are no exceptions permitting clubs to exceed the
Salary Cap.

!
173!
The NHL’s Salary Cap is similar to the NFL’s in that it has a hard upper limit (with a few exceptions) as
well as setting some type of salary floor.
2. Rookie Compensation
Almost all NHL rookies are “Group 1 Players”—players who signed their first contract between the ages
of 18 and 24 and are still playing pursuant to the contract.
1402
Group 1 Players are subject to the Entry
Level System. The Entry Level System dictates the length of a player’s rookie contract depending on the
age at which the player first signed the contract:
1403
Table 5-F: NHL Entry Level System
Age at First Contract Signing
Contract Length
18–21
3 years
22–23
2 years
24
1404
1 year
Group 1 Players’ compensation may only take the form of NHL Paragraph 1 (base) salary,
1405
signing
bonuses, games-played bonuses, and performance bonuses.
1406
The players’ compensation in salary,
signing bonuses and games-played bonuses cannot exceed $925,000 in any year of their first contract.
1407
However, a player can negotiate with the club the opportunity to receive performance bonuses that can
raise his compensation up to $3,775,000.
1408
Moreover, the player is eligible for performance bonuses
from the league that can raise his compensation several hundred thousand dollars.
1409
Once a player’s rookie contract expires, he is no longer subject to the Entry Level System. At that point,
the player is either subject to the club’s exclusive rights or enters another Group depending on his age and
experience level, as is explained next.
3. Veteran Compensation
Once a player is no longer subject to the Entry Level System, i.e., his rookie contract has expired, he will
typically transition from being a Group 1 Player into some other Group:
• Group 2: Players with expired contracts, who signed their first contract between the ages of 18
and 24 and have reached a certain level of experience: (1) for players who signed their first
contract between the ages of 18 and 21, three years of minor league or NHL experience; (2) for
players who signed their first contract between 22 and 23, two years of minor league or NHL
experience; and, (3) for players who signed their first contract at 24 or older, one year of minor
league or NHL experience.
1410
Group 2 players are Restricted Free Agents, provided the club has
made a Qualifying Offer.
1411
• Group 3: Players with expired contracts who have either played at least seven years in the NHL
or are at least 27 years old.
1412
Group 3 players are Unrestricted Free Agents.
1413
• Group 4: Players who, while still under contract, instead play in a league not affiliated with the
NHL and then later try to return to the NHL.
1414
Group 4 players are known as “Defected
Players,” and the NHL club from which the player defected retains the right to match any offer in
the event the player returns to the NHL.

!
174!
• Group 5: Players with expired contracts who have played at least ten years in the minor leagues
or NHL and in the final year of their most recent contract did not earn more than the average
salary.
1415
Group 5 players are Unrestricted Free Agents,
1416
but, in reality, any player who would
meet the criteria for Group 5 status would already be a Group 3 player.
1417
The NHL and NHLPA
nonetheless kept the Group 5 status in the CBA in the event it applied in future CBAs due to
possible definitional or criteria changes.
1418
• Group 6: Players with expired contracts who are at least 25 years old, have played at least three
seasons in the minor leagues, a European professional league while on loan from an NHL club, or
the NHL and have played less than 80 NHL games (or 28 games if a goalie).
1419
Group 6 players
are Unrestricted Free Agents.
1420
In addition to the Groups listed above, clubs hold exclusive rights over their players who have an expired
contract and less than three years of experience.
1421
Provided the club offers the player a contract meeting
certain criteria in the CBA, the player can only sign with his prior club.
1422
The NHL is the only Big Four league that takes age into consideration when determining free agent
status.
In addition to the above-described scenarios, the NHL also has a salary arbitration mechanism for
Restricted Free Agents. Players are eligible for salary arbitration depending upon the age at which they
signed their first contract and their minor league, European league (while on loan from an NHL club) and
NHL experience level:
1423
Table 5-G: NHL Salary Arbitration Eligibility
Age at First Contract Signing
Minimum Years of Experience
18–20
4 years
21
3 years
22–23
2 years
24 and older
1 year
An eligible player is always entitled to elect salary arbitration,
1424
while clubs can only elect salary
arbitration in two situations. First, clubs can elect salary arbitration if the player’s prior year salary
exceeded $1,750,000,
1425
a figure that is adjusted upward based on the mean salary in the league and
equaled $1,953,297 in 2016. Second, the club can file for salary arbitration if an eligible player has not
filed for salary arbitration by his July 5 deadline.
1426
Once the salary arbitration process has commenced,
the player and the club both then submit briefs on the player’s value and can request either a one- or two-
year contract, with some restrictions based on the player’s experience level.
1427
The arbitrator renders a
decision within 48 hours and has the discretion to choose the player’s salary,
1428
i.e., unlike in MLB’s
salary arbitration process, the arbitrator is not bound to choose one side’s position, but can determine the
amount at his or her discretion.
4. Minimum, Maximum, and Average (Mean) Salaries
The minimum salary for an NHL player during the 2016–17 season is $575,000.
1429
As for maximum salaries, no player contract can provide for compensation in any year in excess of 20%
of the Upper Limit.
1430
In addition, NHL player contracts are restricted in terms of the variability of the
!
175!
salary over the term of the contract.
1431
Generally speaking, these rules limit how much salaries can
increase or decrease from year to year and prevent clubs from evading the Salary Cap. For purposes of
counting a player’s salary against the Salary Cap in any given year, the player’s average salary over the
term of the contract is used.
1432
Thus, the variability rules prevent a club from adding years that the player
is unlikely to play to the end of the contract for minimum compensation, which can have the effect of
reducing the Salary Cap charge of the contract.
In 2010 (prior to the most recent CBA), the New Jersey Devils are alleged to have tried to do just that.
The Devils and Ilya Kovalchuk agreed to a 17-year contract worth $102 million.
1433
However, in the final
five years of the contract, during which Kovalchuk would have been ages 39–44, Kovalchuk was due to
earn only $550,000 per year, far short of the nearly $9 million per year that he was set to earn in the first
11 years of the contract.
1434
The NHL invalidated the contract on the grounds that it was an illegal attempt
to circumvent the Salary Cap, a decision that was upheld by an arbitrator.
1435
The Kovalchuk case led to
the creation of the variability rules in the 2013 CBA as well as a seven-year cap on player contract length
(eight if the club is re-signing its own player).
1436
The NFL has some similar rules. Rookie contracts cannot increase more than 25% in the second year of
the contract (to avoid possible circumvention of the Total Rookie Allocation),
1437
and contracts extending
beyond the life of the CBA cannot increase more than 30% (to avoid possible circumvention of the Salary
Cap).
1438
The mean salary of an NHL player during the 2016–17 season was approximately $2,892,546,
1439
slightly
more than the estimated $2.7 million mean salary in the NFL. Additionally, the average contract was 3.5
years in length.
1440
5. Guaranteed Compensation
The NHL Standard Player Contract permits clubs to terminate player contracts at their discretion at
certain times during the off-season.
1441
This authority is broader than in the NFL CBA. However, in the
NHL, if the club chooses to terminate the player’s contract, it must “buy out” the player’s contract. The
portion of a player’s salary that must be bought out is determined by his age. If the player is under 26
years of age at the time of termination, the club must pay the player, an amount equal to one-third of the
player’s base salary.
1442
If the player is 26 years of age or older, the club must pay the player, an amount
equal to two-thirds of the player’s base salary.
1443
Clubs must pay the buyout over twice as many years as
are remaining on the term of the contract. Generally, clubs are still obligated to pay any amounts owed to
the player in the form of a signing bonus even if they terminate the player’s contract.
1444
In addition, unlike most NFL players’ contracts, NHL players’ contracts are guaranteed against injury.
The Standard Player Contract provides that if a player is injured during the course of his employment as a
hockey player and is subsequently unable to perform his duties as a hockey player, the club will continue
to pay the player his base salary so long as the player is unable to play up until the expiration date of the
contract.
1445
E. Compensation in the CFL
The most recent CBA agreed to by the CFL and the Canadian Football League Players Association
(“CFLPA”) was executed in 2014 and expires in 2019. The CFL CBA does not specify, but it stands to
reason that all of the below amounts are in Canadian dollars.
1. The CFL’s Salary Cap
!
176!
The CFL CBA sets both a maximum
1446
and a minimum
1447
amount each club can spend on player
salaries:
Table 5-H: CFL Salary Cap Ranges
Season
Range
2015
$4,450,000–$5,050,000
2016
$4,500,000–$5,100,000
2017
$4,550,000–$5,150,000
2018
$4,600,000–$5,200,000
By comparison, in 2016, the NFL’s Salary Cap was $155.27 million,
1448
more than 30 times than the that
of the CFL (in Canadian dollars).
The 2006 CBA entitled players to 56% of league revenues.
1449
However, this provision was eliminated in
the 2010 CBA, which also included an increase in the Salary Cap.
The CFL’s revenues in 2013 were estimated to be approximately $180 million, of which the players
reportedly only received approximately 20%.
1450
This number seems surprising considering the players’
prior guarantee of 56% of revenues. Nevertheless, assuming the estimates of league revenue are accurate,
the accuracy of the reported revenue split is borne out by simple calculations. There are nine teams in the
CFL. Assuming all of them spent to the maximum of the Salary Cap in 2016, they would have spent
$45,900,100 on player salaries collectively. That figure only represents only 25.5% of the CFL’s
estimated $180 million in revenue. The fact that three of the clubs make their financial statements public
supports the estimate of the league’s revenues.
1451
2. Rookie Compensation
CFL rookies sign a one-year contract with a one-year club option.
1452
If the club exercises the option, the
contract must provide the player with at least the same level of salary and bonus payments (except signing
bonus) that the player earned under the prior contract.
1453
The club option can only be exercised once.
1454
3. Veteran Compensation
Upon expiration or termination of a player’s rookie contract (including any option years), a player in the
CFL becomes an Unrestricted Free Agent and can sign with any club without any compensation to the
player’s prior club.
1455
In contrast, NFL players are only Unrestricted Free Agents after the expiration of their rookie contract if
they have obtained four Accrued Seasons—which would necessarily happen if the player plays until the
expiration of his CBA-mandated four-year rookie contract.
4. Minimum, Maximum, and Average (Mean) Salaries
The minimum salary for an CFL player in the 2016 season was $52,000.
1456
There are no maximum
salaries in the CFL. Nevertheless, the Salary Cap imposes limitations on player salaries collectively.
The mean CFL player salary is approximately $80,000 per year.
1457
This income is supplemented by
signing bonuses and post-season playoff compensation.
1458
!
177!
Many CFL players supplement their income with a secondary career, including the league’s 2013 Most
Outstanding Player, Calgary Stampeders running back Jon Cornish.
1459
Although growth in league
revenues suggests the number is decreasing, the Stampeders communications director estimated that 10%
of the club’s roster holds secondary jobs.
1460
In 2014, the last year where such data was made public, the
highest paid player in the CFL was reportedly B.C. Lions quarterback Travis Lulay, who earned a salary
of approximately $450,000.
1461
5. Guaranteed Compensation
As a general matter, CFL contracts are not guaranteed.
1462
The Standard Player Contract provides clubs
the right to terminate the player’s contract in five situations:
(1) “in the opinion of the said Medical Committee, the Player is not
completely fit to participate in football activities”
1463
;
(2) “the Player fails at any time during the term of th[e] Contract to
demonstrate sufficient skill and capacity to play football of the calibre
required by the Club”
1464
;
(3) “the Player’s work or conduct in the performance of th[e] Contract is
unsatisfactory”
1465
;
(4) “where there exists a limit to the number permitted of a certain class of
Player and the Player, being within that class, should not be included
amongst the permitted number”
1466
; and,
(5) “termination of th[e] contract is in the best interest of the Club having
regard for the competitiveness of the Club as a whole or the formation of
a team with the greatest overall strength.”
1467
These situations are very similar to the situations under which an NFL club can terminate a player’s
contract. Most importantly, both in the NFL and CFL, clubs can terminate contracts if the player is
injured or no longer good enough.
Despite CFL clubs’ termination rights, the CBA does provide certain veteran players with some level of
protection. Players are entitled to 100% of their salary for the remainder of that season if their contract is
terminated after a certain point in the season, depending on their level of experience:
1468
Table 5-I: CFL Player Salary Protection Against Injury
Years of Experience
Required Games to Receive Salary
6 or more
9
5
10
4
11
The CFL’s salary protection for certain veterans is similar to the NFL’s Injury Protection
1469
and
Termination Pay
1470
benefits.
Finally, CFL rookies receive signing bonuses which are typically considered guaranteed compensation. In
2015, the first overall pick of the CFL Draft, lineman Alex Mateas, received a signing bonus of
$20,000.
1471
!
178!
F. Compensation in MLS
MLS and the MLS Players Union (“MLSPU”) agreed to the most recent CBA in 2015, which expires in
2020.
In analyzing the MLS compensation structure, it is important to understand how the labor relations
dynamic between MLS and MLSPU is potentially different from that of the other sports leagues. MLS,
formed in 1995, was structured in an effort to be considered a single-entity under the antitrust laws,
1472
a
distinction further explained below. In operational terms, rather than having each club owned and
controlled by a different person or entity, as in the other sports leagues, all of the clubs in MLS are owned
and controlled by Major League Soccer, LLC, a Delaware limited liability company.
1473
Major League
Soccer, LLC then has operator-investors, entities that have bought into MLS for the right to a certain
amount of control over a single MLS club.
1474
However, the amount of control is significantly less than in
the other American sports leagues, as the clubs have to abide by strict MLS rules concerning player
compensation and transactions.
1475
Generally, MLS negotiates the contracts with players and then
allocates the players to the clubs,
1476
or the clubs choose among the players hired by MLS.
1477
MLS’ structure was designed to avoid the antitrust litigation and scrutiny common to the other
professional sports leagues.
1478
As we discussed in the beginning of this Chapter, Section 1 of the
Sherman Antitrust Act prohibits contracts, combinations, or conspiracies that unreasonably restrain
trade.
1479
If an organization or joint venture is considered a single entity, there can be no multiplicity of
parties agreeing to rules that might unreasonably restrain a market—such as the market for players’
services through eligibility rules, a Salary Cap, or free agency rules as have often been the subjects of
litigation in other leagues. In other words, without multiple parties there cannot be the contract,
combination, or conspiracy necessary for antitrust scrutiny.
1480
Nevertheless, within a year of beginning play, in Fraser v. Major League Soccer, L.L.C., several players
sued MLS alleging that its rules on player compensation and mobility were violations of the antitrust
laws. The United States District Court for the District of Massachusetts found that MLS was a single-
entity and thus dismissed the plaintiffs’ Section 1 antitrust claims.
1481
The remainder of the plaintiffs’
claims was dismissed after a jury found that the plaintiffs had failed to adequately allege a relevant
market in which MLS had allegedly violated the antitrust laws.
14821483
On appeal, the United States Court
of Appeals for the First Circuit was skeptical that MLS’ structure constituted a single entity for purposes
of antitrust law, but declared that the question “need not be answered definitively in this case.”
1484
The
Court of Appeals nevertheless affirmed the dismissal of the plaintiffs’ claims based on the jury’s
determination.
1485
Thus, the effectiveness of MLS’ efforts to be considered a single entity is questionable.
After the Fraser case, MLS players formed the MLSPU to negotiate terms and conditions of employment
with MLS in a CBA.
1486
However, without the clear threat of antitrust litigation (and the concomitant
treble damages), the players and MLSPU potentially lack the authority and leverage of other professional
sports unions.
1487
But as MLS has grown both in revenues and clubs, control and financial investment by
the operator-investors has increased, causing some to question whether MLS’ operations are sufficiently
centralized to potentially be considered a single entity for purposes of antitrust law.
1488
In sum, because of MLS’ structure, MLS—as compared to other professional sports leagues—is
potentially less concerned that its rules concerning player compensation and employment are a violation
of antitrust law, which would subject it to treble damages.
1489
Consequently, MLS has more leverage in
CBA negotiations with the MLSPU than other leagues do with their unions. This lack of union power is
shown, in part, in MLS’ compensation structures.

!
179!
1. MLS’ Salary Cap
The Salary Cap for the 2017 season is $3,845,000,
1490
and increases about 7% annually.
1491
However,
during the 2017 season, MLS clubs are permitted to acquire up to three players whose salaries exceed
$480,625,
1492
but whose salaries will only count against the Salary Cap in the amount of $457,500 (or less
if they are under the age of 24).
1493
These players, known as Designated Players, are considered important
for MLS to attract and retain high-quality players who might otherwise play in Europe.
1494
In the 2016
season, there were 49 designated players.
1495
The 46 Designated Players for whom salary information is
available earned an average of $1,766,329.
1496
Of the 49 designated players, only 9 were American-
born.
1497
MLS’ revenues are approximately $600 million per year,
1498
less than 5% of the NFL’s approximately $14
billion in annual revenue.
2. Rookie Compensation
Unlike the Big Four leagues, MLS does not have compensation rules specific to rookies.
3. Veteran Compensation
Prior to the 2015 CBA, veteran MLS players had no free agency. Under the old system, players with
expired contracts could be redrafted by other MLS clubs without any say in where they were assigned.
1499
The 2015 CBA initiated a limited form of free agency. Players with expired contracts who are 28 or older
and have played at least eight years in MLS now have the ability to select their MLS club.
1500
The players’
salaries will be restricted based on their prior salaries: players who previously made more than $200,000
can receive a 15% increase; players who made between $100,000 and $200,000 can receive a 20%
increase; and, players who made less than $100,000 can receive a 25% increase.
1501
4. Minimum, Maximum, and Average (Mean) Salaries
The minimum salary in MLS for the 2016 season was $62,500 per year.
1502
There is no maximum player salary in MLS.
1503
However, the maximum amount a player’s salary can
count against the Salary Cap is $457,500 (unless they are a Designated Player).
1504
There are also
complicated accounting mechanisms by which clubs can “buy down” a player’s Salary Cap charge.
1505
The mean salary of an MLS player in 2016 was $290,246, and the median salary was $108,900.
1506
However, the average salary figure is skewed by the distribution of salaries. Out of 558 MLS players, 22
of them made $1 million per year or more, with four players (Michael Bradley, Gerrard Steven, Frank
Lampard, and Kaka) making $6 million per year or more.
1507
When these 22 players are removed from the
calculation as outliers, the average salary of the remaining 536 players is only $169,886.
1508
Similarly,
when the salaries of the 46 Designated Players for whom salary information was available in 2016 are
removed as outliers, the average salary drops to $156,847.
1509
Due to these wide disparities in player
income, the MLSPU made it a priority to try and establish a “middle class” in MLS, including by
providing for some form of free agency and raising the minimum salary.
1510
5. Guaranteed Compensation
The contract of any player 24 years old or older who has at least one year of playing experience is
automatically guaranteed,
1511
meaning that it cannot be terminated “solely because of the quality of the
Player’s on-field performance or the fact that the Player may have sustained an injury during the
!
180!
performance of his duties as an MLS Player.”
1512
As a result, the majority of MLS player contracts are
guaranteed.
1513
In 2016, the average MLS player contract had an average of $317,892 in guarantees.
1514
However, if one
removes the 46 Designated Players for whom there was salary information as outliers, MLS player
contracts contain, on average, $168,821 in guaranteed compensation.
1515
G. Analysis
The below table summarizes some of the key provisions and figures concerning compensation structures
in professional sports, subject to the various nuances and intricacies discussed above.
Table 5-J: Comparisons of Leagues’ Compensation Statistics and Policies
NFL
MLB
NBA
NHL
CFL
MLS
Mean Annual
Salary
$2.7
million
$4.25
million
$6.9-8
million
$2.89
million
$80,000
$290,246
Mean Career
Length
5.0
years
1516
5.6
years
1517
4.8 years
1518
5.6 years
1519
3.2
years
1520
3.2 years
1521
Minimum
Salary (2016)
$450,000
$507,500
$543,471
$575,000
$52,000
$62,500
Maximum
Salary
No
No
Yes
Yes
No
No
Maximum
Contract Length
No
No
Yes
Yes
No
No
Unrestricted
Free Agency
Rights
After four
seasons
After six
seasons
After five
seasons for
first round
picks
Depends on
age and
experience
Upon
expiration
of rookie
contract
28 years old
and eight
years of
experience
Guaranteed
Compensation
~ 44%
~ 100%
~ 90%
For injury
and one-
third or two-
thirds of the
player’s
salary
Almost
none
For players
24 and older
with 1+
years’
experience
Salary Cap Type
Hard
Luxury
Tax
Soft and
Luxury Tax
Hard
Hard
Soft
Guaranteed
Share of
Revenue
Yes
No
Yes
Yes
No
No
At the beginning of this Chapter, we identified two key ways in which compensation and compensation
structures affect player health: (1) influencing players’ decisions about playing with injuries; and, (2)
players’ retirement planning and eventual retirement. We are most concerned with how compensation and
compensation structures affect player behavior and decision-making concerning their health, i.e., what are
the consequences of the current compensation regimes on players’ short- and long-term health.
Unfortunately, these are questions that we cannot fully answer at the present.
!
181!
To effectively and rigorously compare how the different leagues’ compensation structures affect player
health decisions would require the ability to control for the various levers, including free agency rules,
salary and contract limitations, salary cap structure, and the level of guaranteed compensation.
Additionally, one would likely also want to be able to control for other relevant factors, such as career
length, career earnings and injury outcomes. The type and amount of health-related benefits, discussed at
length in Chapter 3, also impact player compensation structures. Each of the leagues’ compensation
structures is an amalgam of these various levers and factors. This is a challenging analysis that requires
more data than is currently available and thus we cannot fairly assess which leagues’ overall
compensation structures among the Big Four are best for players.
1522
There is, however, one compensation issue that is the subject of frequent discussion and thus merits
further analysis: guaranteed compensation. As discussed above, many people believe that NFL player
health could be improved through guaranteeing more of their compensation. The belief is that by
guaranteeing a player’s future compensation, he will not feel pressured to play through injuries to protect
his status on the club. On this and related issues, many would argue that MLB’s system is the most
player-friendly, because compensation is almost entirely guaranteed, there is no hard Salary Cap, there is
no maximum salary, and, there is no maximum contract length.
1523
It is thus not surprising that, as of
February 2017, the 23 largest contracts among these sports leagues are all for MLB players.
1524
However,
MLB players are not guaranteed a share of the revenue like in other leagues and must wait six years
before becoming an Unrestricted Free Agent, the longest wait of the Big Four and thus it is not clear that
their compensation arrangement is preferable.
The NFL and NFLPA are frequently criticized—by players,
1525
the media
1526
and academics, among
others—for what is perceived as the lack of guaranteed contracts as compared to the other leagues.
1527
However, the issue is complicated. As a preliminary matter, when discussing the compensation paid to
players, one must also consider the benefits the players receive. As is discussed in Chapter 3 of this
Report, the NFL generally provides a benefits package superior to those offered in all of the other
leagues. The additional complications on this issue are discussed below in the Recommendation Section.
H. Recommendation
Recommendation 5-A: The NFL and NFLPA should research the consequences and feasibility of
guaranteeing more of players’ compensation as a way to protect player health.
As discussed above, guaranteed compensation in the NFL is a complicated issue. While many people—
and players in particular—have expressed a desire for increased guaranteed compensation, it is not clear
that fully guaranteed compensation would be beneficial to players collectively such that it ought to be
preferred to the status quo.
As a preliminary matter, the NFLPA itself has expressed mixed views about the guaranteed contracts. In a
2002 editorial in The Washington Post, then-NFLPA Executive Director Gene Upshaw acknowledged
that the possibility of guaranteed contracts “is severely undermined by the risk of a career-ending injury”
and touted the benefits available to players as an alternative.
1528
Then, in two reports issued by the NFLPA
in or around 2002 and 2007 respectively, the NFLPA asserted that NFL player compensation is, in fact,
largely guaranteed by explaining that more than half of all compensation paid to players is guaranteed.
1529
However, importantly, this statistic does not mean that half of all compensation contracted was
guaranteed—indeed, as discussed above, approximately 44% of all contracted compensation is
guaranteed. Players are often paid guaranteed money (e.g., a signing bonus or roster bonus) in the first or
second year of the contract only to have the base salaries (the unguaranteed portions) in the later years of
the contract go unpaid because the player’s contract was terminated.

!
182!
With this background in mind, there are several reasons why fully guaranteed compensation might not be
beneficial to players collectively. First, while fully guaranteed contracts might be good for the players
who receive them, it could result in many players not receiving any contract at all. If clubs were forced to
retain a player of diminishing skill because his contract was guaranteed, a younger or less proven player
might never get the opportunity to sign with the club.
1530
Relatedly, clubs might continue to provide
playing opportunities to the players with larger contracts in order to justify those contracts, preventing
younger players from establishing themselves as starting or star players and earning higher salaries. It is
also likely that under a system of guaranteed compensation, player salaries would decrease (at least in the
short-term)—particularly the salaries of the highest paid players and players who are less certain to add
value to a roster—as clubs would be more cautious about taking on the financial liabilities, especially
given the Salary Cap in place in the NFL. Similarly, clubs also may seek to minimize their financial
liabilities by reducing roster sizes, which might cost marginal players their jobs, while again reducing
opportunities for young or unproven players to join a club.
There are also logistical challenges to implementing fully guaranteed contracts. The finances and
operations of the NFL and its clubs are greatly intertwined with the fact that NFL contracts have never
been fully guaranteed. Since 1993, NFL clubs have had to comply with a strict Salary Cap that
necessarily influences the types of contracts clubs are willing to offer, including the possibility of
guaranteed compensation. Fully guaranteed contracts would be a fundamental and monumental alteration
to the current business of the NFL that, at a minimum, would require a gradual phasing in process.
1531
It is possible that a rate of guaranteed contracts less than 100% but more than the current 44% is also
optimal. Given the varying factors to be weighed and considered, it is not clear what percentage of
guaranteed compensation would maximize player health for the most NFL players.
Clearly this is a complex issue, with the potential for substantial unintended consequences. Thus, we
recognize the likely health value of guaranteed contracts, while simultaneously recognizing that it may
not be the right solution for all players. Importantly, as discussed above, players who value a contractual
guarantee over potentially higher but uncertain compensation may negotiate for that protection
individually, as many currently do. Moreover, we expect that other recommendations made in this Report
and, more importantly, our other Report, Protecting and Promoting the Health of NFL Players: Legal and
Ethical Analysis and Recommendations, including key recommendations related to the medical
professionals who care for players,
1532
if adopted, would make great strides toward protecting and
promoting player health such that guaranteed compensation would be less critical for that purpose.
Ultimately, we recommend further research into this question, including player and club perspectives,
economic and actuarial analysis, and comprehensive consideration of the relevant trade-offs,
ramifications, and potential externalities. In the meantime, we note that the trend toward greater use of
contractual guarantees can help promote individual player health and allow individual negotiation by
players based on their own goals and priorities.
CHAPTER 6: ELIGIBILITY RULES
Each of the leagues has rules governing when individuals become eligible to play in their leagues. While
we fully acknowledge the unique nature and needs of the leagues and their athletes, we believe the
leagues can learn from the other leagues’ policies.
Leagues’ eligibility rules affect player health in two somewhat opposite directions: (1) by potentially
forcing some players who might be ready to begin a career playing for the leagues to instead continue
playing in amateur or lesser professional leagues with less (or no) compensation and at the risk of being
injured; and, (2) by protecting other players from entering the leagues before they might be physically,

!
183!
intellectually, or emotionally ready. As will be shown, the NCAA’s Bylaws are an important factor in
considering the eligibility rules and their effects on player health and thus must be included in this
discussion. This issue too is discussed in our Recommendations.
In this Chapter we explain each of the leagues’ eligibility rules as well as the rules’ relationship to player
health, if any. But first, we provide: (1) information on the eligibility rules’ legal standing; (2) general
information about the leagues’ drafts that correspond to their eligibility rules; (3) an explanation of the
NCAA and its relevance to the leagues’ eligibility rules; and, (4) insurance options that might be available
to players before joining one of the leagues.
Legal Standing of the Eligibility Rules
Each of the sports leagues we discuss in this Report, except MLS
1533
, consists of member clubs that are
individually owned and operated, with the league serving as a centralized, governing body. The clubs
compete both on and off the field, court, or ice.
1534
Off the field, most notably, clubs compete in the labor
market for players’ services, bidding against one another on the terms of a contract in hopes of persuading
a player to sign with their club. Eligibility rules put a limitation on this market by prohibiting certain
potential players from participating in the market. The clubs—through the eligibility rules—have
collectively agreed not to bid and contract for the services of particular classes of individuals.
The clubs’ eligibility rules have the potential to violate the antitrust laws.
1535
Section 1 of the Sherman
Antitrust Act prohibits contracts, combinations or conspiracies that unreasonably restrain trade.
1536
The
eligibility rules restrain trade by prohibiting potential players from contracting with clubs. Whether this
restraint is “unreasonable” requires a complicated antitrust analysis of a variety of legal and factual
factors.
1537
Nevertheless, the leagues’ eligibility rules have been generally treated as not subject to antitrust scrutiny.
Certain collective actions by the clubs are exempt from antitrust laws under what is known as the non-
statutory labor exemption. The non-statutory labor exemption exempts restrictions imposed by a multi-
employer unit—such as sports clubs—where the restrictions were negotiated with a labor organization,
i.e., a union, as part of the collective bargaining process.
1538
For each of the professional sports leagues
discussed in this Report, there is a corresponding union that represents the players and negotiates a
collective bargaining agreement (“CBA”) with the league. Consequently, based on at least the decision of
the United States Court of Appeals for the Second Circuit in the Clarett case (explained below), it appears
that so long as the eligibility rules are negotiated with the union, they will be exempt from the antitrust
laws.
15391540
The eligibility rules in the NFL, NBA, NHL, and CFL are all collectively bargained with those leagues’
respective players associations and are thus exempt from antitrust law.
1541
Below, we discuss each of these
leagues’ eligibility rules as well as the unique circumstances of MLB’s and MLS’ eligibility rules.
In most cases, the leagues’ eligibility rules are designed, in part, to require players to enter the leagues
through their respective drafts. As will be discussed below, the size of these drafts can have important
impacts on player decisions concerning their eligibility. Table 6-A provides information about the drafts.
Table 6-A: Leagues’ Drafts
NFL
MLB
NBA
NHL
CFL
MLS
Month
April/May
June
June
June
May
January
Length
Seven
40
Two
Seven
Seven
Four

!
184!
Rounds
1542
Rounds
1543
Rounds
1544
Rounds
1545
Rounds
1546
Rounds
1547
Approximate
Number of
Players
255
1,215
60
210
60
84
The NCAA
The NCAA is a non-profit unincorporated association headquartered in Indianapolis through which the
nation’s colleges and universities govern their athletic programs. The NCAA consists of over 1,200
member institutions, all of which participate in the creation of NCAA rules and voluntarily submit to its
authority.
1548
The NCAA’s member institutions hire a President to oversee its affairs, currently Mark
Emmert, formerly the President of the University of Washington.
As will be demonstrated below, the majority of players in the leagues played college sports at NCAA
member institutions and according to the NCAA’s rules before joining their respective leagues. The
NCAA’s rules have a substantial impact on players and their decisions about when to join one of the
professional leagues.
The NCAA Bylaws declare that “[o]nly an amateur student-athlete is eligible for intercollegiate athletics
participation[.]”
1549
Moreover, there must be “a clear line of demarcation between college athletics and
professional sports.”
1550
Consequently, student-athletes are generally barred from receiving any
compensation of any kind for their athletic ability other than a scholarship,
1551
and stipends to cover the
full cost of attendance.
1552
The NCAA Bylaws also limit a student-athlete’s options concerning joining one of the leagues. The effect
of certain NCAA Bylaws will be discussed in the course of this Chapter but here we highlight two
specific Bylaws that affect player health and eligibility.
First, NCAA Bylaws generally prohibit players from hiring agents
1553
or retaining a lawyer to represent
them in contract negotiations.
1554
Were they permitted in NCAA sports, agents and attorneys would have
the ability to communicate with professional clubs about a player’s prospects and also, if the player has
been drafted but has collegiate eligibility remaining (as will be explained below), negotiate with the club
so the player can make an informed decision about whether to return to college or turn professional.
While some student-athletes may have the sophistication or support to do this by themselves, it stands to
reason that they could benefit from the advice of experienced counsel. Nevertheless, NCAA Bylaws
prohibit players from having lawyers who have any direct contact with professional clubs.
1555
There is, however, an important caveat to this discussion. In 2014, the NCAA approved allowing the five
most competitive and highest revenue producing conferences (ACC, Big 12, Big Ten, Pac-12, and SEC)
to write their own rules on certain matters.
1556
As a result, in 2016, these conferences agreed to allow high
school baseball players who are drafted to have an agent negotiate a potential contract with an MLB
club.
1557
The player must pay the agent a market rate and if the player chooses to enroll in college rather
than sign with the MLB club, he must terminate the relationship with the agent.
1558
This rule, which can
be adopted by other conferences, will provide baseball players with a meaningful opportunity to consider
whether to turn professional instead of enrolling in college.
Second, NCAA Bylaws effectively prohibit basketball and football student-athletes from returning to
intercollegiate athletics if they are eligible for the draft but are undrafted.
1559
College basketball student-
athletes are, however, permitted to declare for the NBA Draft and attend pre-Draft workouts and return to
school provided they withdraw their name from the NBA Draft and had never hired an agent.
!
185!
Nevertheless, the players still are unable to actually weigh the results of having been drafted against the
possibility of returning to school. Thus, players in both basketball and football must weigh whether they
are physically, emotionally, and intellectually ready for the professional ranks, or to return to college and
play for free while risking an injury that might jeopardize their ability to ever play professionally.
The NCAA and some of these Bylaws are currently the subject of lawsuits throughout the country. The
lawsuits principally contend that the NCAA’s prohibition against student-athletes earning pay while
playing violates various legal doctrines and laws, notably the Sherman Antitrust Act’s prohibition against
agreements that unreasonably restrain trade.
1560
Nevertheless, the NCAA Bylaws are still in existence as
of today and thus play an important role in analyzing leagues’ eligibility rules and their effect on player
health.
To address the concerns of student-athletes who are weighing whether to turn professional, in 1990 the
NCAA created the Exceptional Student-Athlete Disability Insurance (“ESDI”) program.
1561
We discuss
the ESDI and other insurance options next.
Players’ Insurance Options
In light of the NCAA’s rules prohibiting players from being compensated while playing college sports (as
many are effectively required to do for reasons explained below), some athletes might want insurance
policies to protect against an injury preventing or reducing their future professional earnings. Such
athletes generally have two options: (a) the NCAA’s ESDI program; and, (b) loss of value insurance
policies through private insurers.
Student-athletes who demonstrate that they have the potential to be selected in the first three rounds of the
NHL Draft, the first two rounds of the NFL Draft, or the first round of the NBA, MLB, or Women’s
National Basketball Association (“WNBA”) Draft are eligible for the NCAA’s Exceptional Student-
Athlete Disability Insurance (“ESDI”) program.
1562
The program pays student-athletes a lump sum
payment 12 months after determining that the player has suffered permanent total disability.
1563
The ESDI program, administered through HCC Specialty Underwriters Company, used to cap coverage at
$5 million for projected first-round NFL Draft picks and men’s basketball student-athletes,
1564
while
coverage for baseball, men’s ice hockey and women’s basketball was capped at $1.5 million, $1.2
million, and $250,000, respectively.
1565
However, the amount of coverage is now determined by the
insurer “based upon [the student-athlete’s] prospective status in the upcoming draft.”
1566
The premiums
cost between $3,000 and $6,000 annually for each $1 million of coverage, depending on the sport and the
player’s position, which is considered a few thousand dollars less expensive than a private policy.
Beginning in 2014, the NCAA has permitted colleges to pay the premiums on behalf of the player.
1567
Alternatively, student-athletes may take out loans to pay for the insurance without losing their amateur
status for the NCAA.
1568
Approximately 40 to 50 athletes participate in the ESDI program each year, and
the majority of those athletes are college football players.
1569
In addition to the ESDI program, players might also consider obtaining a loss of value (“LOV”) insurance
policy through a private insurance company. LOV policies provide benefits to players whose draft stock,
and thus the expected value of their contract, decreases due to injury.
1570
For example, if a highly touted
college player suffered an injury that prevented him from being the first overall pick in the draft, a LOV
policy would have paid him the difference between the contract of the first overall pick and the player’s
actual, lesser contract.
In 2014, the NCAA approved permitting players to obtain loans based on the player’s future earnings to
pay for the premiums of LOV policies.
1571
And because LOV policies are provided by private insurers
!
186!
rather than the NCAA, any player is able to obtain one if an insurance company is willing to provide
coverage.
While LOV policies have reportedly become more common in recent years,
1572
research has not revealed
any publicly available data on how many players are obtaining the policies or whether any have had
difficult repaying the loans used to pay the premiums.
In 2015, for example, former Oregon and current NFL cornerback Ifo Ekpre-Olomu collected on a LOV
policy.
1573
Ekpre-Olomu was projected as a first round pick in the 2015 NFL Draft before tearing his ACL
towards the end of the 2014 college season.
1574
As a result of his injury, Ekpre-Olomu dropped to the
seventh round of the NFL Draft.
1575
Ekpre-Olomu’s policy provided him with a $3 million payment as a
result.
1576
In another instance, following the 2016 NFL Draft, former Notre Dame linebacker Jaylon Smith
reportedly collected a $900,000 LOV policy after a knee injury dropped him from the first round into the
second round of the Draft.
1577
With this background information covered, we are now ready to examine the NFL’s player eligibility
rules before comparing them to the other leagues.
A. Player Eligibility Rules in the NFL
The 2011 NFL CBA provides that: “No player shall be… eligible for the [NFL] Draft, until three NFL
regular reasons have begun and ended following either his graduation from high school or graduation of
the class with which he entered high school, whichever is earlier.”
1578
Because there are no football
leagues in the world comparable to the NFL in terms of skill and pay, the NFL’s eligibility rule
effectively requires almost all players to attend college for at least three seasons before they can enter the
NFL Draft.
1579
The NFL’s eligibility rule has faced legal challenges. In 2004, former Ohio State running back Maurice
Clarett initiated an unsuccessful legal challenge to the NFL’s eligibility rule. After a stellar freshman
season in the fall of 2002 in which Clarett led Ohio State to the national championship, Clarett was
suspended by the NCAA for the entire 2003 season due to a variety of NCAA rules infractions.
1580
Rather
than not play the 2003 season and then seek an uncertain reinstatement from the NCAA for the 2004
season, Clarett wished to enter the NFL Draft.
1581
However, because he was not yet three years removed
from his high school graduation, Clarett was ineligible for the Draft.
Clarett sued the NFL, arguing that the NFL’s eligibility rule violated the antitrust laws. After initially
winning in the United States District Court for the Southern District of New York, the United States
Court of Appeals for the Second Circuit, in an opinion written by then-Judge Sonia Sotomayor, reversed.
The Second Circuit held that the NFL’s eligibility rule, even though it was not contained within the CBA,
had been collectively bargained with the NFLPA and was thus immune from antitrust law pursuant to the
non-statutory exemption.
1582
In 2006, to help avoid future challenges, the NFL and NFLPA added the
eligibility rule to the CBA.
The NFL’s eligibility rule creates health-related pressures on two groups of potential players. We discuss
each in turn.
First, the NFL’s eligibility rule affects those college players who have already proven themselves as NFL
prospects but are not yet eligible for the Draft. These players might be concerned about remaining healthy
until they are eligible for the Draft (e.g., freshmen and sophomores). For example, in 2012, sophomore
South Carolina defensive lineman Jadeveon Clowney established himself as the most dominant player in
college football.
1583
Many in the media argued that Clowney would have been the first overall pick in the
!
187!
2013 Draft if not for the NFL’s eligibility rule.
1584
However, because of the eligibility rule, Clowney was
forced to return to South Carolina for the 2013 season. Clowney had a less impressive 2013 season,
including missing several games due to injuries. Clowney’s diminished performance and missed game
time caused some, including South Carolina’s head coach Steve Spurrier, to speculate that Clowney was
more concerned with protecting his NFL Draft status than playing college football.
1585
Clowney was
ultimately selected with the first overall pick in the 2014 NFL Draft.
1586
While Clowney’s story still ended in him being highly drafted, there have been many players who
suffered injuries in college and, as a result, saw their NFL Draft stock drop significantly. For example,
Adewale Ogunleye, from the University of Indiana, was one of the country’s best defensive players
between 1996 and 1999 and considered leaving college early after his junior season in 1998. However,
Ogunleye returned to college and suffered a knee injury during the 1999 season that caused him to go
undrafted and left him unable to play in 2000.
1587
Ogunleye ultimately went on to have a successful ten-
year career in the NFL.
Clowney’s former teammate at South Carolina, Marcus Lattimore, provides another interesting example.
Lattimore, a running back who was First-Team All-SEC in his freshman year,
1588
tore multiple ligaments
in his knee in both his sophomore and junior seasons.
1589
Lattimore was drafted by the San Francisco
49ers in the fourth round of the 2013 NFL Draft, but never played in an NFL game before retiring in 2014
due to ongoing knee problems.
15901591
Fortunately, Lattimore reportedly was eligible for a $1.7 million
payment from a disability insurance policy.
1592
The Clowney, Ogunleye, and Lattimore stories all demonstrate the perils of being prevented from
entering the NFL. A football player might suffer health problems at any time, but at least if the player is
in the NFL, he will have earned (or be entitled to) some money before facing them.
The second group of potential players affected by the NFL’s eligibility rule is comprised of those players
who are eligible for the Draft and who also have college eligibility remaining (e.g., juniors) but are
considering entering the NFL Draft. These players (such as Ogunleye) often face a difficult choice
between entering the Draft or playing another year of college football—during which time they may
improve their skill and improve their Draft prospects, play for a championship at the collegiate level with
their current teammates, and/or finish (or come closer to finishing) their educations, but also risk being
injured.
The NFL’s eligibility rule coupled with the short average duration of NFL careers, rookie contract
structures, and free agency rules all place at least some pressure on players to leave college early for the
NFL Draft. The mean career length of a drafted player is about five years.
1593
NFL rookie contracts are
limited to four years plus a club option for a fifth-year for first round picks and four years for all other
Draft picks.
1594
In addition, the form of rookie contracts is restrictive, limiting the amount players can
potentially earn to amounts far below what Unrestricted Free Agents
1595
might earn on the open
market.
1596
Finally, players cannot even become Unrestricted Free Agents until they have played at least
four seasons.
1597
Consequently, the typical player might only have one year left in his career when he is
finally able to reach free agency and offer his services to the highest-bidding club.
All of this causes some players to believe they need to be in the NFL as soon as possible to capitalize on
the limited timespan during which they can expect to be a healthy and productive NFL player. In
particular, it is common to hear coaches or the media discuss the limited “lifespan” or “tread on the tires”
for running backs.
1598
If not for the NFL’s eligibility rule, it is likely that some players would choose to
enter the NFL Draft after their freshman or sophomore year of college, or maybe even high school, in
order to maximize the perceived potential length of their NFL careers.
!
188!
To assist these players, in 1994, the NFL created an Advisory Committee to help student-athletes
determine their potential Draft round in the NFL Draft and assist them in making the decision of whether
or not to leave school early.
1599
The Advisory Committee is comprised of NFL club general managers,
personnel directors, and scouts, and performs evaluations of student-athletes upon request from the
student-athlete or his athletic department.
1600
The Advisory Committee historically provided the student-
athlete with an estimated range of rounds that the student-athlete should expect to be drafted (e.g., rounds
three through five).
1601
In an effort to discourage players from entering the Draft early, the Advisory
Committee’s assessments are now separated into five categories: “As high as the first round; as high as
the second round; as high as the third round; no potential to go in the first three rounds; and no potential
to be drafted.”
1602
The Advisory Committee’s assessments are confidential so it is thus impossible to
judge their accuracy unless a player discloses them.
Despite the Advisory Committee’s work, recent data suggests that many players declare for the NFL
Draft before they are ready. In 2014, 45 of the 107 players (42%) who left college early were not
drafted;
1603
in 2015, 24 of the 84 early entrants (29%) went undrafted;
1604
and, in 2016, 30 out of the 107
early entrants went undrafted (28%).
16051606
Although those players had the opportunity to sign as
undrafted free agents with any club, they were not guaranteed any compensation if they did so and their
careers are likely to be shorter than those of drafted players.
1607
A player also cannot go through the Draft process and then, if not drafted, return to college football.
Pursuant to NCAA Bylaws, a player who declares for the NFL Draft has only 72 hours to rescind his
declaration or he cannot return to play college football.
1608
The NFL requires student-athletes to declare
for the NFL Draft (which takes place in April or May) by January 15.
1609
Thus, if a player has gone
through the Draft in April or May, he is long past the January 18 (January 15 plus 72 hours) deadline to
return to college football.
Even if the deadline for a player to rescind his declaration for the Draft were extended until after the
Draft, NCAA Bylaws create an additional hurdle to players considering entering the Draft. A college
football season ends in December or January but the NFL Draft is not until April or May. In that interim
period, almost all prospective NFL players undergo extensive training to enable them to show off their
skills at the NFL Combine and in other workouts in front of NFL clubs. The costs of that training and the
player’s living expenses during this time period—which are typically at least $30,000—are almost always
paid for by agents. Consequently, to enter the NFL Draft, a player generally needs an agent—something
forbidden by NCAA rules. Thus, a player who enters the NFL Draft and undertakes the requisite training
to be drafted essentially gives up his NCAA eligibility, which prevents him from playing college football
in the future.
1610
Despite the pressures the NFL’s eligibility rule creates, the NFL’s stated purposes for the rule are largely
to protect player health. In the Clarett case, the NFL offered four reasons for its eligibility rule: “[1]
protecting younger and/or less experienced players—that is, players who are less mature physically and
psychologically—from heightened risks of injury in NFL games; [2] protecting the NFL’s entertainment
product from the adverse consequences associated with such injuries; [3] protecting the NFL clubs from
the costs and potential liability entailed by such injuries; and [4] protecting from injury and self-abuse
other adolescents who would over-train—and use steroids—in the misguided hope of developing
prematurely the strength and speed required to play in the NFL.”
1611
The NFL’s eligibility rule imposes a strict delay on when players can enter the league. Given the injury
concerns about playing football, players are often anxious to get to the NFL as soon as possible to
maximize their potential earnings. Nevertheless, players must weigh their desire to enter the league with
an understanding of whether or not they are physically prepared for the NFL.
!
189!
Now that we have an understanding of the NFL player eligibility rules we are ready to compare them to
the other major leagues.
B. Player Eligibility Rules in MLB
As a preliminary note, comparing player eligibility rules between the NFL and MLB from a health
perspective is likely of diminished significance due to the different injury rates in the sports, discussed at
length in Chapter 2. With that note in mind, we detail the player eligibility rules in MLB and their
substantial difference from those of the NFL.
Players’ eligibility to play in MLB depends on where the player is a resident. The eligibility rules
differentiate players who are residents from the United States
1612
or Canada from those who are not.
American and Canadian players who have never previously contracted with a major or minor league
baseball club
1613
are subject to MLB’s First-Year Player Draft, known as the “Rule 4 Draft,” because the
Draft is set out in Rule 4 of MLB’s Major League Rules
1614
(“MLR”)—but not the CBA).
1615
Additionally,
when players are eligible for the Rule 4 Draft depends on their education status.
The principal result of the Rule 4 Draft is that, generally, once a player enters college, he cannot enter the
Draft again until after his junior year of college (unless he is 21). If the player plays beyond his junior
year, he cannot enter the Draft until his collegiate eligibility has expired, which is typically after his
senior year. Next, we provide a more detailed description of the Rule 4 Draft’s nuances.
High school players are not eligible for the Draft—and thus not eligible for MLB—while “the student is
eligible for participation in high school athletics.”
1616
High school athletic eligibility typically terminates
at the earlier of eight semesters of enrollment or graduation.
1617
A high school player may become eligible
for the Draft prior to graduation if he has become ineligible for high school competition due to his age,
because he has completed the maximum number of allowable semesters of attendance without graduation,
or if “the maximum number of seasons in which the player was eligible to participate in any major sport
has passed,” though in no case may a high school player be obligated “to report for service prior to the
normal graduation of the class with which [he] originally entered high school.”
1618
Additionally, a high
school player who drops out of high school prior to the expiration of his athletic eligibility must remain
out of school for “365 days including the date of withdrawal” before he is eligible for the Rule 4 Draft.
1619
Of the 1,216 players drafted in 2016’s Rule 4 Draft, only 300 (24.7%) were drafted directly out of high
school.
1620
The remaining players all played at least some college or junior college baseball. However,
once a player decides to enter college, his eligibility for the Rule 4 Draft becomes restricted.
Subject to a number of exceptions discussed below, a college
1621
player is ineligible for the Rule 4 Draft
from the “date [he] attends the first class in [his] freshman year” until “the graduation of the class with
which [he] originally entered college,” or the graduation of a subsequent undergraduate class “if [he]
retains eligibility to play baseball at [his] college in [that] year.”
1622
The general rule that a college player is not eligible until the graduation of the class with which he entered
college does not apply to a college player:
(1) who is at least 21 years old and is currently between school years;
(2) who has completed [his] junior year and is currently between school
years;
!
190!
(3) who has completed the full period of [his] eligibility for intercollegiate
baseball;
(4) whose association with [his] college has been terminated by reason of
scholastic deficiency
1623
; or,
(5) who withdraws from college and remains out [of college] for at least 120
days (including the date of withdrawal).
1624
Some high school players may also enter junior colleges. Junior college players are eligible for the Draft
after either their first or second year at the school.
1625
MLB’s different rules result in the possibility that a player can be drafted multiple times. A player drafted
after high school may choose to enter college instead of signing. Players might believe they will have
more opportunity to play and develop in college than in the minor leagues. Then, if the player enters a
four-year college, he cannot be drafted again until he is 21 years of age or after his junior year. If he is
still not ready to sign, he can return for his senior season. In each case, the player does not choose to enter
the Draft—he is automatically subject to the Draft. Therefore, a player could be drafted after high school,
after his junior year of college, and then a third time after his senior year of college.
1626
While MLB’s Draft rules provide considerable flexibility, there have been occasions where players
thought they were sufficiently prepared for MLB before they could be drafted. After completing his
sophomore year of high school in 2009, during which he batted .626, Bryce Harper earned his General
Educational Development (“GED”) and enrolled in a junior college to face better competition.
1627
After
one year in junior college, Harper was selected as the first overall pick in the 2010 Rule 4 Draft at the age
of 17. Nevertheless, Harper’s situation (and talent) is considered anomalous.
We now discuss the eligibility rules for foreign (i.e., non-U.S./non-Canadian) players, assuming they have
not entered an American or Canadian college or otherwise become a resident of the United States. These
foreign players are never subject to the Rule 4 Draft.
1628
Instead, an international player is eligible to sign
a professional contract if he is “17 years old at the time of signing, or . . . will attain age 17 prior to either
the end of the effective season for which the player has signed or September 1 of such effective season,
whichever is later.”
1629
In lieu of a draft, MLB clubs engage in a competitive scouting and bidding process for international
talent, particularly as the rate of foreign-born players has increased. In 2016, 27.5% of players on clubs’
opening day rosters were foreign-born.
1630
Moreover, 22.3% of all MLB players were from South or
Central American countries.
1631
Unfortunately, the scouting and bidding process has been fraught with problems. In Latin American
countries, young baseball players—some not even in their teens—are often found and then controlled by
“buscones,” or street agents.
1632
The buscones control MLB clubs’ access to the players and can
effectively sell the players to the clubs, taking a portion of the players’ signing bonus for themselves.
1633
MLB club personnel have also been caught defrauding their clubs by taking a portion of the signing
bonus allocated for the player (and often splitting it with the buscone).
1634
In addition, there are
widespread problems with identity fraud. Players desperate to reach MLB claim to be younger than they
are or might even pretend to be someone else entirely.
1635
While MLB and MLB clubs have taken steps to
prevent identity fraud and to eliminate the influence of buscones (by having their own academies), many
have also argued that the best way to resolve the issues is through an international Draft.
1636
The 2011 CBA created an International Talent Committee charged with “discuss[ing] the development
and acquisition of international players, including the potential inclusion of international amateur players
!
191!
in a draft, and to examine the rules and procedures pursuant to which international professional players
sign contracts with clubs.”
1637
As part of its mandate, the International Talent Committee was to provide
the MLBPA and MLB with advice on “[t]he appropriate age at which international amateur players
should be signed to professional contracts.”
1638
Other than its first meeting in 2012,
1639
our research has
not revealed any output from the International Talent Committee. At the time of this writing there is still
no draft for international players.
During the 2016 CBA negotiations, it was reported that MLB and the MLBPA seriously discussed the
possibility of a draft for international players.
1640
However, the sides were not able to reach an agreement.
Instead, the parties agreed that Clubs would be subject to a “Signing Bonus Pool” that limited the amount
of compensation Clubs could provide to international players.
1641
The Signing Bonus Pool is a maximum
of $5.75 million, growing annually with league revenues.
1642
Importantly, regardless of how a player ends up with an MLB club—whether through the Draft or as an
international signee—almost all players will play several seasons with the minor league clubs affiliated
with the MLB club that drafted them before signing an MLB contract
1643
or playing in an MLB game, if
they ever even do. Indeed, only about 17% of drafted players ever reach the major leagues.
1644
Players
signed to minor league contracts are not members of the MLBPA and are not entitled to the same rights
and benefits as major league players.
1645
Whereas the minimum salary for a major league player was
$507,500 in 2016,
1646
minor league players often earn between $10,000 and $20,000 per season.
1647
Additionally, for either domestic or international players, health generally would not be a factor in
considering how to proceed with their professional eligibility.
International players generally want to get into international camps or onto minor league clubs affiliated
with MLB clubs as soon as possible, i.e., as soon as they are eligible. MLB’s eligibility rule permits
international players to sign at age 17 (or slightly earlier) and thus is a minimal (if any) barrier to entry for
international players. These camps and clubs generally provide international players with the best
resources—including coaching, housing, and healthcare—that they have ever experienced, while also
increasing their chances of one day making the Major Leagues. In doing so, these players forfeit the right
to ever play college baseball—an unlikely career trajectory for international players anyway. Thus,
international players generally gain little by not entering into a professional contract as soon as they are
able.
MLB’s eligibility rules also do not create health-related concerns for American and Canadian players.
MLB’s eligibility rules do not prevent American and Canadian players, apart from very rare
circumstances (e.g. Bryce Harper), from entering MLB as soon they believe it is in their best interests.
They have the opportunity to become a major leaguer at various times and as early as age 17. By the time
a player reached the skill level necessary to be drafted by an MLB club, he almost certainly would have
reached the age of 17. Thus, the eligibility rule generally does not force players to make difficult
decisions concerning their health.
NCAA eligibility rules, however, can affect an American or Canadian player’s choices. American or
Canadian players who have been drafted by MLB clubs often have to consider whether to forego a
signing bonus worth tens or hundreds of thousands of dollars from an MLB club to play or continue
playing in college. Choosing to remain in college subjects the player to the risk of career-ending or
threatening injury without compensation. As discussed above, the NCAA’s ESDI program attempts to
alleviate some of these concerns.
The NFL and MLB eligibility rules are very different. The NFL eligibility rules effectively require a
player to play three years in college and permit the player one chance to determine when is best for him to
!
192!
enter the NFL. In contrast, MLB eligibility rules allow a player to be drafted multiple times, including
right out of high school.
The differences in the rules are perpetuated by the NCAA’s rules and also the role of agents. A player
becomes ineligible for NCAA competition once he signs with an agent.
1648
However, to be drafted in
MLB, a player does not need an agent. MLB’s Draft is held in June—shortly after a high school or
college player would have finished his season and thus their prior results will largely determine their
Draft performance. As discussed above, college football players almost always need the help of an agent
to prepare for the NFL Draft—help that is forbidden by NCAA rules. As a result, even if the NFL adopted
a system whereby players have the ability to be drafted multiple times like that of MLB, it would be
useless due to the NCAA’s rules.
The number of rounds in each league’s draft also plays an important role. The MLB Draft has 40 rounds.
Additionally, MLB clubs generally do not even sign many of the players they draft and, of the athletes
they do sign, all of them will have to prove themselves in the minor leagues before reaching the MLB
club. Consequently, MLB clubs have much more flexibility in drafting players who might not yet be
ready for MLB. In contrast, the NFL Draft is only seven rounds and every player will immediately join
the NFL club, creating considerably more pressure on NFL clubs to use each and every Draft pick wisely.
NFL clubs do not have the luxury of drafting players who might instead prefer to return to college.
C. Player Eligibility Rules in the NBA
The NBA’s eligibility rules differentiate between American players and international—including
Canadian—players.
1649
American players must meet three criteria to be eligible for the NBA Draft, summarized as follows:
1. The player is or will be at least 19 years old during the calendar year in which the Draft is
held;
1650
2. At least one NBA season must have elapsed since the player’s graduation from high school (or
the graduation of the class with which the player would have graduated high school);
1651
and,
3. The player must meet one of the following seven conditions:
a. The player has graduated from a four-year college or university in the
United States (or is to graduate in the calendar year in which the Draft is
held) and has no remaining intercollegiate basketball eligibility; or,
b. The player is attending or previously attended a four-year college or
university in the United States, his original class in such college or
university has graduated (or is to graduate in the calendar year in which
the Draft is held), and he has no remaining intercollegiate basketball
eligibility; or,
c. The player has graduated from high school in the United States, did not
enroll in a four-year college or university in the United States, and four
calendar years have elapsed since such player’s high school graduation;
or,
d. The player did not graduate from high school in the United States, and
four calendar years have elapsed since the graduation of the class with
which the player would have graduated had he graduated from high
school;
1652
or,
!
193!
e. The player has signed a player contract with a ‘professional basketball
team not in the NBA’ . . . and has rendered services under such contract
prior to the January 1, immediately preceding such Draft; or,
f. The player has expressed his desire to be selected in the Draft in a
writing received by the NBA at least sixty days prior to such Draft (an
“Early Entry” player)[.]
1653
International players must meet two criteria to be eligible for NBA Draft:
1. The player must be at least 19 years old during the calendar year in which the Draft is held;
1654
and,
2. The player must meet one of the following three conditions:
a. The player is or will be twenty-two years of age during the
calendar year of the Draft; or,
b. The player has signed a player contract with a “professional
basketball team not in the NBA” . . . that is located in the United
States, and has rendered services under such contract prior to the
Draft; or,
c. The player has expressed his desire to be selected in the Draft in
a writing received by the NBA at least sixty days prior to such
Draft (an ‘“Early Entry” player).
1655
The NBA’s eligibility rules and their evolution have been controversial. Prior to 1971, the NBA required
players to be four years removed from high school graduation in order to be eligible for the Draft.
1656
In
1970, Spencer Haywood, a former Olympic basketball player who chose to play in the professional
American Basketball Association (“ABA”)
1657
rather than finish college, sued the NBA, alleging that the
NBA’s eligibility rule violated the antitrust laws.
1658
The United States District Court for the District of
California agreed and enjoined the NBA from enforcing its eligibility rule.
1659
Two weeks after the
District Court’s decision, the United States Court of Appeals for the Ninth Circuit stayed the injunction
pending the NBA’s appeal.
1660
However, two weeks later, the Supreme Court of the United States
reinstated the injunction.
1661
Haywood and the NBA then settled the case, with the NBA agreeing to allow
players who were less than four years removed from high school graduation to enter the NBA if they if
they could demonstrate “financial hardship.”
1662
In 1976, the eligibility rule was removed in its
entirety.
1663
Despite the NBA’s removal of the eligibility rule, almost all players continued to spend at least some time
in college before entering the NBA.
1664
Between 1976 and 1995, no players entered the NBA without first
attending college.
1665
In 1995, Chicago high school star Kevin Garnett was chosen with the fifth overall
pick in the Draft, beginning a wave of high school players trying to make the leap straight to the NBA.
Between 1995 and 2005, 39 high schoolers were selected in the NBA Draft.
1666
However, some high schoolers went undrafted
1667
or otherwise had unsuccessful NBA careers, causing
many to believe that they had tried to make the NBA too soon.
1668
As a result, the NBA sought and
obtained the current eligibility rule as part of the 2005 CBA.
1669
Nevertheless, many have also criticized
the current eligibility rule for the creation of so-called “one-and-done” players, that is, players who play
one season of college basketball (as required by the eligibility rule), before entering the NBA Draft.
1670
These players are able to enroll in college, take the minimum number of classes in their first semester, go
to some of their classes as the college basketball season winds down in their second semester, declare for
the Draft, and drop out of school having completed only four or five general education classes.
1671
Since

!
194!
the initiation of the current eligibility rule, 95 players have left college after only one season and were
drafted by an NBA club (a mean of 8.6 per Draft), with mixed success in the NBA.
1672
There are also college players who are eligible for the Draft but, if they have collegiate eligibility
remaining, debate whether to return to college. For these players, the NBA’s eligibility rule is not a
concern but only their readiness for the NBA and the potential for injury at the collegiate level. The
NCAA’s ESDI program, discussed above, is an attempt to alleviate some of the concerns about possible
injury. In addition, beginning in 2016, the NCAA amended its rules to permit underclassmen players to
participate in the NBA’s pre-Draft Combine to allow players to better gauge their Draft potential.
1673
Following the Combine, a player now has ten days to withdraw from the Draft and return to college
(provided he never signed with an agent).
1674
Instead of playing NCAA basketball, some American players have chosen instead to go play
professionally in foreign countries before entering the NBA Draft,
1675
with mixed success. In 2008,
Brandon Jennings, a highly acclaimed high school basketball player from California, decided to play
professional basketball in Italy instead of playing college basketball. After one season in Italy, Jennings
was selected 10th overall in the 2009 NBA Draft and has had, as of the publication of this Report, a
successful NBA career.
1676
Jeremy Tyler, another California basketball player who, in 2009, opted to play
professionally overseas rather than play college basketball in the United States, had less success.
16771678
In addition to playing NCAA basketball or overseas, players have one other option before they are
eligible for the NBA. Players can play in the NBA Development League (“D-League”).
1679
The D-League,
started in 2001, is the NBA’s official minor league, consisting of 22 clubs with players hoping to reach
the NBA.
1680
Indeed, more than 30% of current NBA players have played in the D-League at some
point.
1681
Of most relevance, the minimum age to play in the D-League is 18 years old, one year younger
than the NBA’s requirement.
1682
However, no high school player has ever foregone the NCAA for the D-
League
1683
and most D-League players are undrafted former college players or NBA veterans trying to
make a comeback.
1684
The low salaries (reportedly between $19,500 and $26,000
1685
) likely deter players
from considering the D-League as their best option.
1686
The NBA’s eligibility rule is generally considered the most controversial in sports. To its critics, the rule
prevents young men capable of playing in the NBA from pursuing their chosen career (or at least
choosing to try to play in the NBA) and instead forces them to enroll in college for a brief period of time
even if they have no interest in academics.
1687
Others believe requiring players to mature more before
entering the NBA is essential for their development as both players and people.
1688
Additionally, some
have suggested that by having rookies play at least one year of college basketball, they will be more
familiar to fans and thus be more interesting and marketable to NBA fans.
1689
For these reasons, leading
up to the 2017 CBA negotiations, the NBA suggested requiring players to be at least two years removed
from high school before entering the NBA Draft.
1690
Nevertheless, the NBPA resisted those suggestions
and no changes were made to the eligibility rule in the 2017 CBA.
1691
The NBA and NFL eligibility rules are similar in that they both effectively require players to play at least
some time in college. While the NBA requires one year and the NFL requires three years, both leagues’
rules are generally designed to keep players out of the professional leagues until they are sufficiently
physically and mentally mature, thus arguably protecting both the players and the clubs’ investments in
those players.
D. Player Eligibility Rules in the NHL
To be eligible to play in the NHL, a player must be at least 18 years old and have sufficient vision in both
eyes (a requirement discussed further below).
16921693
To reach the NHL, players are subject to the NHL
!
195!
Draft unless the player is at least 22 years old or is at least 21 years old and played hockey for at least one
season in North America when he was 18, 19, or 20.
1694
The NHL’s Draft and eligibility rules are complicated by the heavily international nature of the NHL. In
the 2016–17 season, 48% of the players were born in Canada, 24.8% were born in America, and the
remaining 27.2% of players were from 13 different European nations.
1695
All players are subject to the
NHL Draft, regardless of their nationality.
The five principal sources of NHL Draft picks are: (1) the Canadian Hockey League, an organization of
three hockey leagues (Quebec Major Junior Hockey League, Ontario Hockey League, and the Western
Hockey League) (“Canadian Juniors”); (2) the United States Hockey League (“USHL”), an American
junior hockey league; (3) American colleges; (4) players playing in European professional leagues; and,
(5) American high schools.
1696
The Canadian Juniors are for players between the ages of 16–20 and
operate like a semi-professional league: the players generally continue to be in school of some kind and
receive a few hundred dollars a month as a stipend.
1697
The NCAA considers Canadian Juniors to be
professional leagues due to the compensation and benefits the players receive.
1698
Consequently, many
young players face a difficult choice between playing hockey for American colleges or playing in
Canadian Juniors.
1699
About 50% of NHL players played in Canadian Juniors,
1700
while about 30% of
NHL players went to an American college.
1701
While the USHL is also for players between the ages of
16–20, it does not provide players a stipend and thus they retain their NCAA eligibility.
The NHL’s eligibility rules provide flexibility for players. High school and college players can be drafted
and choose to instead play college hockey. The drafting NHL club generally holds the player’s rights until
he graduates college, meaning no other club can draft or sign the player.
1702
In the case of non-North
American players, the drafting NHL club holds the player’s rights for four years if the player is 18 or 19,
or two years if he is 20.
1703
After each collegiate season, the player can decide whether to return to college
or to begin his NHL career with the club that drafted him.
The purpose of the NHL’s age requirement is unclear. However, in deciding to return to college as
opposed to enter the NHL, several players have cited the need to continue to grow physically and to gain
weight to be prepared for the NHL.
1704
Thus, assuming age is a proxy for physical size, the NHL’s
eligibility rule prevents players who might not be physically ready for the NHL from entering
prematurely.
Concerning the vision requirement mentioned above, the NHL By-Laws declare ineligible “[a] player
with only one eye, or one of whose eyes has a vision of only three-sixtieths (3/60ths) or under.”
1705
In the
1970s, NHL draftee Greg Neeld, who had lost his left eye in a Juniors game, sued the NHL, alleging that
the rule violated the antitrust laws. The NHL’s rule was ultimately determined to be reasonable and not in
violation of the antitrust laws.
1706
The United States Court of Appeals for the Ninth Circuit determined
that “the primary purpose and direct effect of the League’s by-law was not anticompetitive but rather
safety,” as there was “bound to be danger to players who happen[ed] to be on Neeld’s blind side.”
1707
The NHL’s eligibility rules are generally flexible and do not force players to either abstain from entering
the NHL or to enter the NHL. Players have a variety of options and generally enter the Draft when their
skills and size have sufficiently developed to play in the NHL.
The NHL’s eligibility rule is similar to MLB’s in that it provides players multiple opportunities to
determine when to enter the NHL. The NHL’s eligibility rule thus differs from the NFL’s in many of the
same ways that MLB’s rule does. Prospective NHL players—like prospective MLB players—can easily
be drafted without the assistance of an agent, and thus do not need to risk their NCAA eligibility to
consider whether to turn professional like prospective NFL players do. Additionally, prospective NHL

!
196!
players—also like prospective MLB players—will have to prove themselves in the minor leagues before
reaching the NHL. The minor league system provides NHL—and MLB—clubs several years to develop
their draft picks into productive professionals. In contrast, the NFL does not have a minor league and thus
NFL clubs are under pressure to draft players who are going to have an impact in a relatively short period
of time.
E. Player Eligibility Rules in the CFL
The CFL’s eligibility rules depend on whether the player is a National Player or an International Player.
National Players are those who are Canadian citizens at the time of signing the player’s first CFL
contract, or a player who was physically resident in Canada for an aggregate period of five years prior to
turning 18 years old.
1708
International Players are players who do not meet the criteria to be a National
Player.
1709
National Player eligibility is further differentiated based on whether the player plays in the Canadian
Interuniversity Sport (“CIS”) League, Canada’s equivalent of the NCAA, or in the NCAA or National
Association of Intercollegiate Athletics (“NAIA,” the NCAA’s much smaller American competitor).
National Players who play in the CIS are eligible for the CFL Draft three years after completing their first
year of CIS eligibility.
1710
Under the CIS By-laws, a football player is “charged with a year of eligibility
for each year of competition where the athlete participated in” more than one regular-season game.
1711
Thus, under normal circumstances, a National Player is not eligible for the CFL Draft until he has played
four years of college football. This rule was created in 2013 to eliminate the ability of “redshirt” juniors to
enter the CFL Draft. In college athletics, when a player is “redshirted,” it means he will not compete in
athletics that season,
1712
and that season will not count against the number of seasons that the player is
permitted to play. Therefore, a redshirted player would not be charged with a year of eligibility under CIS
By-laws. A redshirted junior would be a fourth-year player academically but who has only played three
seasons of college football (having sat out the redshirt season). The CFL’s current eligibility rules no
longer permit redshirt juniors to enter the CFL Draft.
1713
National Players who play NCAA or NAIA football are only eligible for the CFL Draft after they have
completed their senior year of eligibility.
1714
Thus, redshirt juniors playing college football in the United
States are also barred from the CFL Draft. Before the rule changes in 2013, juniors who were National
Players playing college football in the United States could be drafted by CFL clubs but still return for
their senior season.
1715
The CFL club would retain rights to the player upon their graduation.
1716
The prior
regime required CFL clubs to speculate on which National Players would choose to leave college after
their junior season for the CFL or choose to instead return to college and play a senior season with the
hopes of maybe making the NFL.
1717
The change was made to improve predictability in the Draft as to
which National Players would actually play in the CFL.
1718
In stark contrast to the rules for National Players and the rules of the NFL, the CFL imposes no age or
education requirements for International Players.
1719
Thus, American high school players could choose to
play in the CFL as opposed to playing college football in the United States. Although our research has not
revealed a case where that actually occurred, we have found at least one case where it was considered. In
2009, star high school running back Bryce Brown was reportedly considering foregoing college for the
CFL.
1720
Brown ultimately chose to attend the University of Tennessee and later Kansas State University
before being selected in the 2012 NFL Draft.
While the CFL eligibility rules permit American players to enter at any time, they are very restrictive of
National Players. Effectively, a National Player cannot join the CFL until he has played four years of
college football. While the rule might assist National Players in obtaining their college degree, it also
!
197!
subjects them to the wear and tear of four years of college football before they can consider becoming
professional. It is likely that some National Players believe they are physically prepared for the CFL prior
to graduation and would prefer to enter the CFL earlier so as to avoid the risk of injury or diminished
skill. However, the CFL rules do not permit a National Player to make that choice.
The CFL’s eligibility rule is more restrictive than that of the NFL’s. Whereas the NFL’s rule only requires
players to play three years of college football, the CFL requires four years of college for National players
(the only players relevant for this discussion). Additionally, the CFL’s eligibility rule does not appear to
be concerned with player health—but is instead principally concerned with CFL clubs’ ability to know
which players are likely to play in the CFL.
F. Player Eligibility Rules in MLS
In contrast to all of the other leagues, MLS does not have an eligibility rule. Players need not be of a
certain age or have reached a certain level of education to play in MLS. Indeed, in the 2016 season, there
were 18 teenagers on MLS rosters, with the youngest player being 16.
1721
Notably, Freddy Adu began
playing with MLS’ D.C. United club in 2004 at the age of 14.
1722
Although there is no eligibility rule, players arrive at MLS via a wide variety of paths. The path by which
a player arrives at MLS determines the process by which the player reaches his club:
1. Allocation Process: U.S. Men’s National Team players, elite youth U.S. National Team players,
and former MLS players returning to MLS after playing with a non-MLS club for a transfer fee of
greater than $500,000 are allocated to clubs pursuant to MLS’ Allocation Ranking List (which is
in the reverse order of the prior season’s standings).
1723
2. SuperDraft: Clubs can nominate players to be in the MLS SuperDraft and only nominated
players can be drafted.
1724
College players, non-collegiate international players, and players from
Generation adidas are eligible for the Super Draft.
1725
3. Discovery Process: Clubs can scout and sign players who are not under contract to MLS and
who are not subject to the Allocation Process or SuperDraft.
1726
The Discovery Process is
typically used to sign foreign players who were not nominated for the SuperDraft.
1727
4. Homegrown Players: Clubs may sign a player to his first professional contract without
subjecting him to the SuperDraft if the player has been a member of the club’s youth academy for
at least one year.
1728
Normally, MLS’ different drafting and signing processes do not place pressure on players. There are a
wide variety of soccer leagues around the world and generally, if a player is good enough, he will have
opportunities. MLS’ rules are generally designed to assist MLS in competing against more talented and
better paying European leagues for players’ services. For example, players signed to Generation adidas
contracts are given incentive-laden contracts that provide the opportunity for greater compensation than if
the player had completed his college degree while also placing money in escrow for them to complete
their college education.
1729
The Generation adidas education payments are similar to the NFL’s Tuition Assistance Plan, which
reimburses players for tuition, fees, and books from attending an eligible education institution. However,
while the Generation adidas program is limited to only some elite players, all current NFL players with at
least one Credited Season are eligible for the Tuition Assistance Plan. Former players with at least five
!
198!
Credited Seasons are also eligible provided that the costs are incurred within four years of the player’s
last season.
Now that we have reviewed the policies of the major leagues we are ready to analyze the NFL’s policies
by comparing them to these leagues’ policies.
G. Analysis
The leagues’ eligibility policies vary. MLS has the most liberal eligibility policy, with no minimum age
requirement, while, by requiring several years of college, the NFL and CFL are the most restrictive.
All of the eligibility rules seemingly are at least partially concerned with when a player is “ready” to enter
a professional league. Readiness is an important concept, but difficult to define. In our view, a player is
ready when he is able to enter the league safely, in terms of protecting his health,
1730
and maximize his
success across various domains, including physically, mentally, and emotionally. Each of the leagues,
often through negotiations with the unions, has made a judgment as to when they think the typical player
is ready, or at least ready enough. In so doing, the leagues have helped protect clubs from drafting and
investing in players who are not ready, and also potentially helped to protect players who need more time
to prepare for a successful and healthy career.
1731
However, without more empirical analysis, we cannot
say for certain when players—individually or collectively—are ready and thus whether the eligibility rule
is fair or successful. No such data currently exists and would be challenging to gather. We discuss this
issue further in the Recommendations.
The NBA is the one league that potentially has the data to inform its eligibility rule. Between 1995 and
2005, 35 high schoolers were selected in the NBA Draft.
1732
Concerned that many of these players were
not ready for the NBA, the NBA instituted its current eligibility rule in the 2005 CBA. Since the initiation
of the current eligibility rule, 95 players have left college after only one season and were drafted by an
NBA club.
1733
One could, in theory, compare the career and health outcomes of the high schoolers that
entered the NBA with those of the one-and-done players and with upperclassmen to potentially evaluate
whether the NBA’s eligibility rule has been effective at preventing players from entering the NBA before
they are ready.
1734
Such a comparison would be helpful, if not conclusive (in part because of selection
effects and other research design problems), in understanding the value of delaying eligibility. Indeed, in
2017, NBA Commissioner Adam Silver discussed the need for the eligibility rule to be “studied” more
closely, including better understanding various factors that affect or are affected by the rule.
1735
While the
NBA’s consideration of this issue is laudable, the data from any such study would have limited
generalizability to the other leagues due to the different demands of each sport.
The Women’s Tennis Association (“WTA”) provides a useful example. WTA’s eligibility rule, probably
more than any other sports organization, is the result of considerable analysis and study. In the early
1990s, there was concern about the well-being and career longevity of teenage players competing on the
WTA Tour.
1736
At the time, fourteen- and fifteen-year-old players were permitted extensive play on the
WTA Tour.
1737
As a result, in 1994, the WTA Tour formed an Age Eligibility Commission to study the
Tour’s eligibility rule.
1738
The Age Eligibility Commission, consisting of sports medicine and sports
science professionals, gathered and analyzed extensive anecdotal, statistical, medical, and scientific
evidence. Among the data gathered was evidence that an early start to a player’s career correlated to an
earlier departure from the Tour.
1739
Based on such evidence, the Commission recommended a revised
eligibility rule,
1740
adopted in 1995, that instituted a graduated maximum number of tournaments for
players beginning at age 14 and with no limits after players reach age 18.
1741
In 2004, the Age Eligibility
Commission’s successor, the Age Eligibility Advisory Panel, conducted an extensive re-examination of
the rule, again gathering a variety of anecdotal, statistical, medical, and scientific evidence.
1742
The Age
!
199!
Eligibility Advisory Panel concluded that the 1995 rule change had been helpful to young players and
enhanced their career longevity, while recommending some minor tweaks.
1743
The comparison of the leagues’ policies highlights two clear issues with the NFL’s eligibility rule, but,
generally, neither is of the NFL’s making.
First, the NFL’s requirement that players effectively play at least three years of college football might
ensure that only sufficiently physically mature players enter professional football, but it also requires
players to risk their physical health longer without getting paid—and in a sport with higher injuries rates
than that of the other leagues, as discussed in Chapter 2: Injury Rates and Policies. While the NCAA’s
ESDI program tries to alleviate some of these issues, players have legitimate concerns that they will
suffer a career-altering or ending injury before they are able to reach the professional level and earn any
money from their athletic skills. This is at least in part a problem resulting from the NCAA’s prohibition
on student-athletes being compensated. Whether the NCAA’s rules are fair is beyond the scope of this
Report, but it is clear that the rules create a problem for players who have the potential to reach the NFL
but who are required—or might prefer—to continue playing college football.
Second, in light of the fact that players are not paid for playing in college, it is understandable that many
want to enter the NFL as soon as possible. Specifically, players will want to enter the NFL after their
junior year of college, the first time they are permitted under the NFL’s eligibility rule. However, whether
the player is ready for the NFL is a difficult question to answer and may not be resolved until many years
later—if ever. If the player is undrafted, NCAA rules effectively prohibit the player from returning to
college football, and the player’s football future is in serious doubt. Once again, although this problem
intersects with the NFL’s eligibility rule, it is the primary result of the NCAA’s rules, not the NFL’s.
Ultimately, without more data, it is unclear what the optimal eligibility rule is in any of the leagues. Thus,
it is also unclear whether any of the leagues can learn from each other on this issue. As a result, we cannot
assess the reasonableness of the NFL’s current eligibility rule. The rule seemingly prevents players from
joining the NFL before they are ready, which both protects those players from injury in the NFL and
protects the clubs from investing in players who are not yet ready to play at a professional level. While
there are likely to occasionally be players who are ready to join the NFL before the end of their junior
season,
1744
there are going to be outliers to any rule and, without data suggesting otherwise, we cannot say
the NFL’s eligibility rule is not reasonable or sufficiently considerate of player health. For this reason our
main recommendation is for the NFL to continue to gather data to permit a better evidence-based
evaluation of its current policy, as well to consider the interplay of its rules with the NCAA’s.
H. Recommendations
Recommendation 6-A: The NFL should consider performing or funding research analyzing when a
player might be “ready” for the NFL.
Currently, the NFL’s eligibility rule appears to be the NFL’s best guess as to when players, as a general
rule, are ready to play in the NFL. However, we are unaware of any rigorous body of data to support the
NFL’s eligibility rule as it is currently written. While the NFL’s eligibility rule seems reasonably
protective of player health based on what is currently known, data could substantially buttress the rule—
or prompt changes to it as necessary. For the sake of player health, the NFL should make efforts to gather
this data.
Among the data that might be valuable in this context are: players’ ages when they enter the league;
players’ height and weight; players’ position; players’ professional results; players’ injury histories;
players’ financial health; players’ education; players’ psychological health; and, players’ post-career

!
200!
activities. This and other data may need to be gathered before, during, and after the player’s career, as
relevant; there may also be questions related to the precise definition of player success for purposes of
this analysis, although certain thresholds on either end of the spectrum will be evident. While some of this
data does currently exist, the ideal comparison would be between players who entered the league under
the current rule and those who entered earlier (or later) on an alternative rule. Because the current
eligibility rule has been in place for decades, direct comparison is difficult. However, it is possible that
the NFL—potentially with the help of others—could learn something from the data that is already
available, for example, comparing the outcomes of players who enter the league at different ages beyond
the eligibility threshold. Of course, this will not answer the question of how individual players might fare
if they could enter the league even earlier than the current rule permits,
1745
but it may nonetheless provide
some helpful information for comparison between players who are younger or older at entry.
Recommendation 6-B: The NFL should reconsider the interplay of its eligibility rules with the NCAA’s
rules as they concern player health and take appropriate action if necessary.
The NFL’s eligibility rule coupled with the realities of the NCAA’s rules cause tremendous pressure on
prospective and future NFL players. While these NCAA rules are not the NFL’s creation, the NFL should
nevertheless acknowledge that the football careers of prospective or future NFL players are substantially
affected by the NCAA’s rules and take steps within its power to address those problems. The combination
of the two organizations’ rules creates situations that many find inequitable and it is thus appropriate for
the NFL to reconsider its eligibility rules’ applicability in those situations and whether anything can be
done to change them.
1746
CONCLUSION
We began this Report by explaining the pressing need for research into the overall health
1747
of NFL
players; the need to address player health from all angles, both clinical and structural; and the challenges
presented in conducting such research and analysis. The issues and parties involved are numerous,
complex, and interconnected. To address these issues—and ultimately, to protect and improve the health
of NFL players—requires a diligent and comprehensive approach to create well-informed and meaningful
recommendations for change.
We believe part of that comprehensive approach is for the NFL and NFLPA to learn from other
professional sports leagues when possible. In many respects, the leagues and their games are very
different and thus it can be challenging to draw comparisons. Nevertheless, the leagues face a series of
common issues, such as labor negotiations, stadiums and arenas, fan interest, multimedia platforms, and
many others. But perhaps the most important issue is player health. In recent years, each of the leagues
has had to make a fresh and comprehensive examination of its player health policies and practices. We
anticipate the leagues will continue to engage in this examination for many years to come.
The leagues have the opportunity to learn a great deal from one another in light of their shared interest in
player health. In this Report we have identified many areas in which the policies and practices of the NFL
concerning player health appear superior to those of the other leagues. Indeed, the NFL’s player health
provisions are generally the most protective of player health among the relevant comparators.
Nevertheless, we also identified several areas in which the policies and practices of the NFL concerning
player health could potentially be improved by comparison to the other leagues:
1. The CFL CBA, unlike the NFL CBA, requires that pre-season physicals “to determine the status
of any pre-existing condition” be performed by a neutral physician.
2. The standard of care articulated in the NHL and MLS CBAs, unlike the NFL CBA, seemingly
requires club doctors to subjugate their duties to the club to their duties to the player at all times.
!
201!
3. MLB, unlike the NFL, has a concussion-specific short-term injury list.
4. The MLB, NHL, and CFL injury reporting policies, unlike the NFL, do not require the disclosure
of the location on the body of a player’s injury.
5. MLB, the NBA, and the NHL, unlike the NFL, generally offer health insurance to players for life.
6. Among the Big Four leagues, the retirement plan payments offered by the NFL are the lowest.
7. MLB and NHL players, unlike in those in the NFL, are vested in their pension plans on the first
day they play in the league.
8. The NBA and CFL, unlike the NFL, offer treatment to players who have violated their
performance-enhancing substance policies.
9. The amount of player compensation that is guaranteed in the NFL is substantially lower than in
the other Big Four leagues.
10. The NFL has the most prohibitive eligibility rule of the leagues (except the CFL).
It is important to note that where we have identified these differences, we have also explained the
different nuances and contexts. In many cases, the NFL’s policies might be justifiably different than the
other leagues and perhaps even superior, despite their apparent deficiency. Thus, it is essential that all of
these differences be examined in a full and fair context.
There is still, however, room for improvement, as each Chapter’s Recommendations show. Additionally,
our Recommendations are only as useful as their implementation. For these reasons, we make the
following final Recommendations.
Final Recommendation 1: The leagues and unions should continue to coordinate on player health
issues and to consider each other’s policies and practices.
Indications are that the leagues do communicate with each other concerning common issues on a regular
basis. Similarly, the unions communicate on common issues. This coordination is assisted by the fact that
many doctors, lawyers, and other professionals are advisors to multiple leagues or unions. It is important
that the leagues and unions continue—and perhaps increase—their level of coordination on player health
issues. As many of the leagues have increased their interest in and funding of research—particularly
medical research—concerning player health issues, valuable data is being created that can help inform
other leagues’ policies and practices. We urge the leagues to share this data—not just with each other but
with all researchers. Moreover, by combining resources the leagues might be able to take on broader and
better projects than they can alone. Finally, as leagues continue to make advancements in player health
policies and practices, it is important that the other leagues and unions take note of those advancements,
consider their possible application to their respective organizations, and make the necessary changes to
protect and promote player health. The leagues are tremendously powerful and influential institutions—
by working together, they can maximize their ability to be positive change agents in player health.
Final Recommendation 2: The media, academics, the leagues, and the unions should continue to
police the advancement of player health.
Following this Report, we do not intend to be a passive voice in the process of improving player health. It
is our hope to be able to periodically review progress on the issues discussed in this Report and provide
additional reports. However, in addition to any progress reports from the authors of this Report or the
Football Players Health Study at Harvard University, we urge and trust that others—in particular the
leagues and unions—will heed the message of this Report and hold other stakeholders accountable.
***
NFL football has a storied history and holds an important place in this country. The men who play it

!
202!
deserve to be protected and have their health needs met and it is our fervent hope that they will be met.
We hope this Report furthers that cause.
APPENDIX A – COMPILATION OF RECOMMENDATIONS
Below, for ease of reference, is a compilation of all of the Recommendations made in this Report.
I. Club Medical Personnel
Recommendation 1-A: Pre-season physicals for the purpose of evaluating a player’s prior injuries
should be performed by neutral doctors.
The CFL requires pre-season physicals for the purpose of evaluating a player’s prior injuries to be
performed by a neutral doctor. The NFL should adopt the same rule. The use of neutral doctors ensures
that players’ medical history is being recorded in an accurate manner, i.e., in a manner that correctly
details a player’s injury history and the ways in which those prior injuries are manifesting themselves
today. Clubs—and thus club doctors—have an incentive to minimize players’ injuries and declare them
fit to play in order to avoid further financial liability. For example, if an NFL player is injured during one
season, and fails the pre-season physical the next season, the player is entitled to an Injury Protection
benefit, an amount equal to 50% of his Paragraph 5 Salary (i.e., base) for the season following the season
of injury, up to a maximum payment of $1,150,000 (in 2016).
1748
If the player is still injured during the
next pre-season, he can obtain Extended Injury Protection, a benefit that permits a player to earn 50% of
his salary up to $500,000 for the second season after suffering an injury that prevented the player from
continuing to play. Additionally, similar to the CFL, if the club doctor finds that a player is healthy
enough to play, a player’s potential Injury Grievance
1749
is undermined. In these situations, the club
doctor, acting in the interests of the club, might be motivated to find that the player is healthy enough to
play during the pre-season physical, preventing the player from receiving benefits and compensation to
which he is entitled. While we do not know if such practices are common or widespread, in our Report
Protecting and Promoting the Health of NFL Players: Legal and Ethical Analysis and Recommendations,
we provided examples from players attesting that such situations do occur.
1750
Whatever the frequency, a
structural conflict still exists and needs to be addressed. A neutral doctor avoids the potential for bias, and
ensures players are receiving their just compensation and care.
As discussed in the Introduction, the NFL declined to review this Report. However, MLB did provide
comments on the Report which may provide insight into the viewpoints of the other professional leagues.
In reviewing a draft of this Report, MLB expressed its disagreement with this recommendation, stating:
The recommendation (1-A) that preseason physical examinations be
performed by a neutral doctor misses the point of the PPE
[preparticipation physical evaluation]. Continuity of care is an important
aspect of player health care and it is the view of our medical experts that
having a separate physician for the preseason exam would result in worse
care during the season. The recent Consensus Monograph on PPE, which
was prepared by several national physician groups and is viewed as the
governing document on these types of exams, does not include a
recommendation for independent physicians.
While we generally agree with MLB that continuity of care is important, we disagree with MLB’s
comment for several reasons.
!
203!
First, it is important to understand we believe there is a structural conflict of interest whereby NFL club
doctors provide care to players while also providing services for the club.
1751
As a result, players have
business reasons to be concerned about the outcome of the pre-season physical. As explained above, club
doctors may not accurately record a player’s condition, which can negatively affect his contract status and
benefits to which he is entitled.
Second, our recommendation would not affect continuity of care as MLB’s comment seems to suggest.
Assuming doctors working for the club continue to treat players (which is not what we recommend), the
club doctor would have full access to the results of the pre-season physical and is also permitted to re-
examine the player at any time, including during the pre-season. However, a physical performed by a
neutral doctor should be used to establish the player’s pre-existing conditions in order to better protect the
player’s business interests.
Third, MLB’s reference to the consensus monograph
1752
is misplaced. The monograph specifically states
that it “is intended to provide a state-of-the-art, practical, and effective screening tool for physicians who
perform PPEs for athletes in middle school, high school, and college.”
1753
Thus, the monograph does not
apply to professional sports, and does not speak to the issues raised above.
II. Injury Rates and Policies
Recommendation 2-A: The NFL, and to the extent possible, the NFLPA, should: (a) continue to
improve its robust collection of aggregate injury data; (b) continue to have the injury data analyzed by
qualified professionals; and, (c) make the data publicly available for re-analysis.
As explained above, each of the Big Four leagues and MLS seems to have a quality injury tracking
system, allowing for the accumulation of current information about the nature, duration, and cause of
player injuries. As stated above, we rely on this data in this Report because it provides the best available
data concerning player injuries, although we cannot independently verify the data’s accuracy.
Nevertheless, if accurately collected, this data has the potential to improve player health through analysis
by qualified experts so long as it is made available to them. In particular, analysis potentially could be
performed to determine, among other things, the effects of rule changes, practice habits, scheduling, new
equipment, and certain treatments, while also identifying promising or discouraging trends and injury
types in need of additional focus.
1754
Notably, the NFL already conducts this type of analysis through
Quintiles.
However, the NFL does not publicly release its aggregate injury data (nor does any other league).
1755
The
NFL does release some data at its annual Health & Safety Press Conference at the Super Bowl. However,
the data released at the Press Conference is minimal compared to the data available and the analyses
performed by Quintiles. For the data to have the potential meaningful applications mentioned above, it
must be made available in a form as close to its entirety as possible. Such disclosure would permit
academics, journalists, fans, and others to analyze the data in any number of ways, likely elucidating
statistical events, trends, and statistics that have the opportunity to improve player health. To be clear we
are recommending the release of more aggregate data, not data that could lead to identification of the
injuries of any particular player or cause problems concerning gambling.
Publicly releasing injury data, nevertheless, comes with complications that we must acknowledge. While
more transparency in injury reporting is necessary, the nuances of such data can easily be lost on those
without proper training. Sports injury prevention priorities in public health can be swayed by public
opinion and heavily influenced by those with the most media coverage. Making injury data publicly
available may allow those with the media access to dictate the agenda regardless of the actual
implications of the data. As a result, it may be harder for injury trends that may be more hazardous, but
!
204!
less visible in the media, to get the attention they need, even when the data clearly shows the importance
of these issues. Thoughtful, balanced, peer-reviewed results may have difficulty competing against those
statistics which garner the most media attention. For this and other reasons, in our report Protecting and
Promoting the Health of NFL Players: Legal and Ethical Analysis and Recommendations, we
recommended that “[t]he media… engage appropriate experts, including doctors, scientists, and lawyers,
to ensure that its reporting on player health matters is accurate, balanced, and comprehensive.”
1756
The
medical, scientific, and legal issues concerning player health are extremely complicated, which demands
that the media take care to avoid making assertions that are not supported or that do not account for the
intricacies and nuance of medicine, science, and the law.
In light of these concerns, one possible intermediate solution is to create a committee of experts that can
review requests for data and determine whether or not the usage of the data is appropriate and will
advance player health. Indeed, the Datalys Center for Sports Injury Research and Prevention performs this
role concerning access to NCAA student-athlete injury data.
1757
Moreover, such committees have also
been formed in the clinical research setting.
1758
Recommendation 2-B: Players diagnosed with a concussion should be placed on a short-term injured
reserve list whereby the player does not count against the Active/Inactive 53 man roster until he is
cleared to play by the NFL’s Protocols Regarding Diagnosis and Management of Concussions.
1759
According to the leading experts, 80–90% of concussions are resolved within seven to ten days.
1760
Thus,
concussion symptoms persist for longer than ten days for approximately 10–20% of athletes. In addition,
there are a variety of factors that can modify the concussion recovery period, such as the loss of
consciousness, past concussion history, medications, and the player’s style of play.
1761
Consequently, a
player’s recovery time from a concussion can easily range from no games to several games. The uncertain
recovery times create pressure on the player, club, and club doctor. Each roster spot is valuable and clubs
constantly add and drop players to ensure they have the roster that gives them the greatest chance to win
each game day. As a result of the uncertain recovery times for a concussion, clubs might debate whether
they need to replace the player for that week or longer. The club doctor and player might also then feel
pressure for the player to return to play as soon as possible. By exempting a concussed player from the 53
man roster, the club has the opportunity to sign a short-term replacement player in the event the
concussed player is unable to play. At the same time, the player and club doctor would have some of the
return-to-play pressure removed.
In fact, MLB already has such a policy. MLB has a seven-day Disabled List (as compared to its normal
10- and 60-day Disabled Lists) “solely for the placement of players who suffer a concussion.”
1762
Why treat concussions differently than other injuries in this respect? This is a fair question to which there
are a few plausible responses. First, in terms of the perception of the game by fans, concussions have
clearly received more attention than any of the other injuries NFL players might experience and thus the
future of the game depends more critically on adequately protecting players who suffer from them.
Second, concussions are much harder to diagnose than other injuries, such that there may be a period of
uncertainty in which it would be appropriate to err on the side of caution.
1763
Third, both players and
medical professionals have more difficulty anticipating the long-term effects of concussions as compared
to other injuries, given current scientific uncertainties concerning brain injury.
1764
Fourth, and perhaps
most importantly, it is much harder to determine the appropriate recovery times for concussions as
compared to other injuries.
1765
These reasons all support a recommendation to exclude concussed players
from a club’s Active/Inactive roster, but we recognize that the key feature of players potentially feeling or
facing pressure to return before full recovery may be shared across any injury a player may experience.
Thus, it may also be reasonable to consider extending this recommendation to injuries beyond
concussions.
1766

!
205!
In reviewing a draft of our Report, Protecting and Promoting the Health of NFL Players: Legal and
Ethical Analysis and Recommendations, the NFL argued that “[t]he current NFL roster rules actually
provide greater flexibility” than is recommended here.
1767
The NFL explained that because “[t]here is no
limitation on how long a player may be carried on the 53-man roster throughout the season without being
‘activated,’… a player who is concussed routinely is carried on his club’s 53-man roster without being
activated until he is cleared.”
1768
However, for the reasons explained above, we believe concussions
should be treated differently. All 53 spots on the roster are precious to both the club and the players. The
uncertainty surrounding recovery from a concussion presents unique pressures that can be lessened with
the approach recommended here.
Indeed, the NFL’s practice has been to treat concussions differently from other injuries. As part of its
Concussion Protocol, players suspected of having suffered a concussion during a game are examined by
doctors unaffiliated with the club, and to be cleared to play in the next game they must be cleared by
doctors unaffiliated with the club. For all other injuries, club doctors are the only ones to examine and
clear players to play. Additionally, in 2016, the NFL sent a memo to all clubs directing them not to
comment on a player’s progress in returning from a concussion.
1769
Instead, the NFL directed clubs to
state only “that the player is in the concussion protocol under the supervision of the medical team, and the
club will monitor his status.”
1770
This is in contrast to the clubs’ open discussion of players’ other injuries.
The Washington football club essentially proposed our recommendation at the 2016 owners' meetings.
Washington proposed amending the NFL bylaws to provide that a player who has suffered a concussion,
and who has not been cleared to play, be placed on the club’s Exempt List, and be replaced by a player on
the club’s Practice Squad on a game-by-game basis until the players is cleared to play. Unfortunately, the
proposal was not adopted.
Recommendation 2-C: The NFL should consider removing the requirement that clubs disclose the
location on the body of a player’s injury from the Injury Reporting Policy.
In our Report Protecting and Promoting the Health of NFL Players: Legal and Ethical Analysis and
Recommendations, we recommend the NFL consider fining and/or suspending players if they discuss or
encourage targeting another player’s injury.
1771
However, the need for this Recommendation would be
reduced if the NFL’s Injury Reporting Policy did not openly disclose the location on the body of players’
injuries, a requirement imposed only by the NFL, NBA and MLS.
The gambling-related interests of full disclosure likely do not outweigh the risks of targeting by other
players created by the Injury Reporting Policy.
1772
While additional data—including from federal law
enforcement authorities—could inform this analysis—it seems unlikely that the risks of injury
information being sold on a black market are so high to justify a known risk of players intentionally
aiming to hit a player in an area known to be injured because of the Injury Reporting Policy. Similarly,
we see no inequity in clubs not knowing the full extent of an opposing club’s player injuries.
Consequently, we recommend that the NFL consider removing the requirement that clubs disclose the
location of a player’s injury from the Injury Reporting Policy.
III. Health-Related Benefits
Recommendation 3-A: The NFL and NFLPA should consider whether change is necessary concerning
player benefit plans.
As discussed above, we identified three potential areas of concern regarding the benefit plans offered by
the NFL. Also as discussed above, the benefits available to NFL players must be viewed in the context of
!
206!
one another: increasing one benefit might mean a decrease in another benefit. Below, we identify and
discuss possible changes to the benefit plans, the implementation of which must be weighed collectively.
• The NFL and NFLPA should consider providing former players with health insurance
options that meet the needs of the former player population for life: While the NFL provides
significant benefits to former players, players likely do not take full advantage of those benefits
due to the associated administrative burdens.
1773
Additionally, a consistent and reliable health
insurance plan seems preferable to ad hoc and uncertain benefits. The NFL and NFLPA should
consider whether it would be more appropriate to shift some of the value of benefits away from
the unplanned benefits (e.g., disability benefits and the health reimbursement account) to more
stable health insurance options.
1774
Where players have only played one or two seasons (and
perhaps games), there might be questions as to whether it is appropriate to provide lifetime health
insurance to someone who was employed for such a short period of time. On the other hand, only
a few games or seasons can have life-lasting effects on a player. One option worth considering is
tiering health insurance benefits and allowing those with less Credited Seasons to qualify for
some but not full benefits.
• The NFL and NFLPA should consider increasing the amounts available to former players
under the Retirement Plan: The monthly retirement benefits represent a more stable benefit
than the other valuable but still uncertain benefits. Consequently, the NFL and NFLPA should
consider whether it would be more beneficial to shift some of the value of benefits away from the
unplanned benefits to the more stable Retirement Plan monthly payments.
• The NFL and NFLPA should consider reducing the vesting requirement for the Retirement
Plan: The purpose of the NFL’s three-year vesting requirement is unclear. The vesting
requirement results in a considerable portion of former players being unable to collect any
retirement benefits. We acknowledge that there may be appropriate policy reasons for such a
limitation, such as a determination as to when a player has sufficiently contributed to the NFL.
Indeed, many employers require a certain number of years of service before accruing certain
benefits.
1775
If the vesting requirement is instead principally motivated by cost, then the
distribution of benefits among former players should be reconsidered to determine what is
maximally beneficial for player health. In other words, is the current distribution of benefits
among former players, which largely excludes players with less than three years of experience,
preferred by the NFL, NFLPA, and players, or would it be preferable to reduce the benefits to
players with more than three years of experience to provide some benefits to those with less than
three years of experience? While these considerations are not easy and require a delicate balance,
the exclusion of a significant portion of former players from the Retirement Plan requires an
examination of the vesting requirement. As with health insurance benefits, one option worth
considering is tiering Retirement Plan benefits and allowing those who have played less than
three Credited Seasons to qualify for some if not full benefits.
IV. Drug and Performance-Enhancing Drug Policies
Recommendation 4-A: The NFL should consider amending the PES Policy to provide treatment to any
NFL player found to have violated the PES Policy.
The NFL and the other leagues recognize that substance abuse is a serious medical issue and, as a result,
provide players with robust counseling and treatment. As discussed above, PES usage has been shown to
be associated with a variety of serious physical and mental ailments. However, only the NBA and CFL
offer treatment for players who have used PES. In light of the potential negative health consequences
!
207!
associated with PES usage and the treatment provided by the NBA and CFL for PES usage, it seems
prudent for the NFL to consider providing treatment to PES users similar to that provided for by the
Substance Abuse Policy’s Intervention Program.
There is an important clarification to this Recommendation. As stated earlier in this Chapter, we are not
focused on the competitive advantage concerns associated with PES use or the discipline imposed by the
leagues for drug or PES usage. We are focused on the health implications of drug and PES policies. Thus,
our Recommendation should not be read to suggest that because players might need treatment for PES
usage that they should not be disciplined—as is the case for first time offenders of the Substance Abuse
Policy.
As discussed in the Introduction, the NFL declined to review this Report. However, MLB did provide
comments on the Report which may provide insight into the viewpoints of the other professional leagues.
MLB did not agree with this Recommendation, stating:
There are no established treatment programs for PEDs, and since the
recidivism rate for PEDs is fairly low, there is no support for the position
that this class of prohibited substances warrants a response based on
treatment. It is also an established practice of not just MLB, but all other
professional leagues and international anti-doping organizations that the
use of PEDs affects the integrity of play and should be responded with a
disciplinary perspective as opposed to a clinical one. Our experts advise
not including “PED treatment programs” as a recommendation in the
report.
As a preliminary matter, we note that the NBA and CFL do provide treatment to PES users. Thus, there is
a disagreement among the leagues (and potentially also the unions) on this issue, suggesting further
research is needed.
We further reply to MLB with a clarification and with a disagreement. We understand sports
organizations’ need to discipline players who have violated PES policies. Our recommendation does not
seek the elimination or reduction of discipline for PES violations in any way. Instead, we believe it is
appropriate to consider providing players who have violated the PES Policy with counseling, regardless
of any discipline imposed. This is where we and MLB disagree.
MLB rejects counseling for PES use on the grounds that “[t]here are no established treatment programs
for PEDs.” As discussed above, experts in the field recommend and do provide treatment for PES usage
and its associated problems. Whether these programs are sufficiently “established,” is beyond our
expertise, but it nonetheless is an issue worth further consideration.
V. Compensation
Recommendation 5-A: The NFL and NFLPA should research the consequences and feasibility of
guaranteeing more of players’ compensation as a way to protect player health.
As discussed above, guaranteed compensation in the NFL is a complicated issue. While many people—
and players in particular—have expressed a desire for increased guaranteed compensation, it is not clear
that fully guaranteed compensation would be beneficial to players collectively such that it ought to be
preferred to the status quo.
!
208!
As a preliminary matter, the NFLPA itself has expressed mixed views about the guaranteed contracts. In a
2002 editorial in The Washington Post, then-NFLPA Executive Director Gene Upshaw acknowledged
that the possibility of guaranteed contracts “is severely undermined by the risk of a career-ending injury”
and touted the benefits available to players as an alternative.
1776
Then, in two reports issued by the NFLPA
in or around 2002 and 2007 respectively, the NFLPA asserted that NFL player compensation is, in fact,
largely guaranteed by explaining that more than half of all compensation paid to players is guaranteed.
1777
However, importantly, this statistic does not mean that half of all compensation contracted was
guaranteed—indeed, as discussed above, approximately 44% of all contracted compensation is
guaranteed. Players are often paid guaranteed money (e.g., a signing bonus or roster bonus) in the first or
second year of the contract only to have the base salaries (the unguaranteed portions) in the later years of
the contract go unpaid because the player’s contract was terminated.
With this background in mind, there are several reasons why fully guaranteed compensation might not be
beneficial to players collectively. First, while fully guaranteed contracts might be good for the players
who receive them, it could result in many players not receiving any contract at all. If clubs were forced to
retain a player of diminishing skill because his contract was guaranteed, a younger or less proven player
might never get the opportunity to sign with the club.
1778
Relatedly, clubs might continue to provide
playing opportunities to the players with larger contracts in order to justify those contracts, preventing
younger players from establishing themselves as starting or star players and earning higher salaries. It is
also likely that under a system of guaranteed compensation, player salaries would decrease (at least in the
short-term)—particularly the salaries of the highest paid players and players who are less certain to add
value to a roster—as clubs would be more cautious about taking on the financial liabilities, especially
given the Salary Cap in place in the NFL. Similarly, clubs also may seek to minimize their financial
liabilities by reducing roster sizes, which might cost marginal players their jobs, while again reducing
opportunities for young or unproven players to join a club.
There are also logistical challenges to implementing fully guaranteed contracts. The finances and
operations of the NFL and its clubs are greatly intertwined with the fact that NFL contracts have never
been fully guaranteed. Since 1993, NFL clubs have had to comply with a strict Salary Cap that
necessarily influences the types of contracts clubs are willing to offer, including the possibility of
guaranteed compensation. Fully guaranteed contracts would be a fundamental and monumental alteration
to the current business of the NFL that, at a minimum, would require a gradual phasing in process.
1779
It is possible that a rate of guaranteed contracts less than 100% but more than the current 44% is also
optimal. Given the varying factors to be weighed and considered, it is not clear what percentage of
guaranteed compensation would maximize player health for the most NFL players.
Clearly this is a complex issue, with the potential for substantial unintended consequences. Thus, we
recognize the likely health value of guaranteed contracts, while simultaneously recognizing that it may
not be the right solution for all players. Importantly, as discussed above, players who value a contractual
guarantee over potentially higher but uncertain compensation may negotiate for that protection
individually, as many currently do. Moreover, we expect that other recommendations made in this Report
and, more importantly, our other Report, Protecting and Promoting the Health of NFL Players: Legal and
Ethical Analysis and Recommendations, including key recommendations related to the medical
professionals who care for players,
1780
if adopted, would make great strides toward protecting and
promoting player health such that guaranteed compensation would be less critical for that purpose.
Ultimately, we recommend further research into this question, including player and club perspectives,
economic and actuarial analysis, and comprehensive consideration of the relevant trade-offs,
ramifications, and potential externalities. In the meantime, we note that the trend toward greater use of
contractual guarantees can help promote individual player health and allow individual negotiation by
!
209!
players based on their own goals and priorities.
VI. Eligibility Rules
Recommendation 6-A: The NFL should consider performing or funding research analyzing when a
player might be “ready” for the NFL.
Currently, the NFL’s eligibility rule appears to be the NFL’s best guess as to when players, as a general
rule, are ready to play in the NFL. However, we are unaware of any rigorous body of data to support the
NFL’s eligibility rule as it is currently written. While the NFL’s eligibility rule seems reasonably
protective of player health based on what is currently known, data could substantially buttress the rule—
or prompt changes to it as necessary. For the sake of player health, the NFL should make efforts to gather
this data.
Among the data that might be valuable in this context are: players’ ages when they enter the league;
players’ height and weight; players’ position; players’ professional results; players’ injury histories;
players’ financial health; players’ education; players’ psychological health; and, players’ post-career
activities. This and other data may need to be gathered before, during, and after the player’s career, as
relevant; there may also be questions related to the precise definition of player success for purposes of
this analysis, although certain thresholds on either end of the spectrum will be evident. While some of this
data does currently exist, the ideal comparison would be between players who entered the league under
the current rule and those who entered earlier (or later) on an alternative rule. Because the current
eligibility rule has been in place for decades, direct comparison is difficult. However, it is possible that
the NFL—potentially with the help of others—could learn something from the data that is already
available, for example, comparing the outcomes of players who enter the league at different ages beyond
the eligibility threshold. Of course, this will not answer the question of how individual players might fare
if they could enter the league even earlier than the current rule permits,
1781
but it may nonetheless provide
some helpful information for comparison between players who are younger or older at entry.
Recommendation 6-B: The NFL should reconsider the interplay of its eligibility rules with the NCAA’s
rules as they concern player health and take appropriate action if necessary.
The NFL’s eligibility rule coupled with the realities of the NCAA’s rules cause tremendous pressure on
prospective and future NFL players. While these NCAA rules are not the NFL’s creation, the NFL should
nevertheless acknowledge that the football careers of prospective or future NFL players are substantially
affected by the NCAA’s rules and take steps within its power to address those problems. The combination
of the two organizations’ rules creates situations that many find inequitable and it is thus appropriate for
the NFL to reconsider its eligibility rules’ applicability in those situations and whether anything can be
done to change them.
1782
VII. Conclusion
Final Recommendation 1: The leagues and unions should continue to coordinate on player health
issues and to consider each other’s policies and practices.
Indications are that the leagues do communicate with each other concerning common issues on a regular
basis. Similarly, the unions communicate on common issues. This coordination is assisted by the fact that
many doctors, lawyers, and other professionals are advisors to multiple leagues or unions. It is important
that the leagues and unions continue—and perhaps increase—their level of coordination on player health
issues. As many of the leagues have increased their interest in and funding of research—particularly
medical research—concerning player health issues, valuable data is being created that can help inform
!
210!
other leagues’ policies and practices. We urge the leagues to share this data—not just with each other but
with all researchers. Moreover, by combining resources the leagues might be able to take on broader and
better projects than they can alone. Finally, as leagues continue to make advancements in player health
policies and practices, it is important that the other leagues and unions take note of those advancements,
consider their possible application to their respective organizations, and make the necessary changes to
protect and promote player health. The leagues are tremendously powerful and influential institutions—
by working together, they can maximize their ability to be positive change agents in player health.
Final Recommendation 2: The media, academics, the leagues, and the unions should continue to
police the advancement of player health.
Following this Report, we do not intend to be a passive voice in the process of improving player health. It
is our hope to be able to periodically review progress on the issues discussed in this Report and provide
additional reports. However, in addition to any progress reports from the authors of this Report or the
Football Players Health Study at Harvard University, we urge and trust that others—in particular the
leagues and unions—will heed the message of this Report and hold other stakeholders accountable.
APPENDIX B – COMPILATION OF SUMMARY TABLES
Below, for ease of reference, is a compilation of all of the tables summarizing the leagues’ various
policies and practices at the end of each Chapter of this Report. Note that Chapter 6: Eligibility Rules
does not include a summary table.
Table 1-C: Summary of Club Medical Personnel Policies and Practices
Do the Leagues’ Policies:
NFL
MLB
NBA
NHL
CFL
MLS
Quality of Medical Care
Require retention of doctors?
Yes
Yes
Yes
Yes
No
No
Require retention of athletic trainers?
Yes
Yes
Yes
Yes
Yes
No
Require sports-specific certification for
doctors?
Yes
No
Yes
Yes
No
No
Set forth a standard of care?
Yes
No
1783
No
Yes
No
Yes
Disclosure and Player Autonomy
Require medical staff to disclose
communications with club to player?
Yes
No
No
No
No
No
Require club to pay for second opinion?
Yes
Yes
Yes
Yes
No
Yes
Provide club doctor right to determine a
player’s course of treatment?
No
No
Yes
Yes
No
Yes
Entitle players to surgeon of their choice?
Yes
No
1784
No
Yes
No
No
Entitle players to medical records?
Yes
Yes
Yes
Yes
Yes
Yes
Require players to submit to physicals
upon request?
Yes
Yes
Yes
No
Yes
Yes
Confidentiality
Permit non-medical club personnel to
obtain and disclose player health
information?
No
Yes
Yes
Yes
No
Yes
Require players to inform club of care by
other medical professionals, regardless of
payment source?
No
If
basebal
l-
related
Yes
No
No
No
!
211!
Conflicts of Interest
Insulate club medical staff from influence
by coaches and other club personnel?
No
No
No
No
No
No
Prohibit healthcare providers from paying
for right to provide care?
Yes
Yes
Partiall
y
Unkno
wn
No
No
Table 2-L: Comparison of Leagues’ Regular Season Injury Statistics
1785
Table 2-M: Comparison of Leagues’ Injury Policies
NFL
MLB
NBA
NHL
CFL
1786
UEFA
MLS
1787
Electronic
Tracking
System
Yes
Yes
Yes
Yes
No
N/A
1788
Yes
Mean Injuries
Per Season
1789
1,511.0
1,516.6
369.8
728.0
N/A
N/A
N/A
Rate of
Injuries Per
Player-Season
0.69
0.93
0.88
0.85
N/A
N/A
1790
N/A
Mean
Concussions
Per Season
1791
160.0
18.0
9.0
93.0
57.0
1792
N/A
1793
N/A
1794
Rate of
Concussions
Per Player-
Season
0.073
0.016
0.019
0.108
N/A
1795
N/A
1796
N/A
Concussions
As Percentage
of Injuries
1797
10.5%
1.8%
2.4%
12.8%
N/A
1.9%
N/A
Mean Injuries
Per Game
5.90
0.45
0.16
0.59
N/A
0.53
N/A
Rate of Injury
Per Player-
Game
0.064
0.016
0.016
0.016
N/A
0.038
N/A
Regular
Season Games
Per Player-
Injury
15.60
62.50
62.50
62.50
N/A
N/A
N/A
Most Common
Injury/Injured
Body Part
1798
Concussio
n
Upper leg
(thigh)
Ankle
Sprain
Head
N/A
Thigh
N/A
Concussions
Per Game
0.625
0.007
0.007
0.067
0.704
0.010
N/A
Rate of
Concussion
Per Player-
Game
1799
0.00679
0.00026
0.00035
0.00180
0.00800
0.00072
N/A
Games Per
Concussion
Per Player
147.10
3,846.15
2,857.14
555.56
125.00
1,388.89
N/A
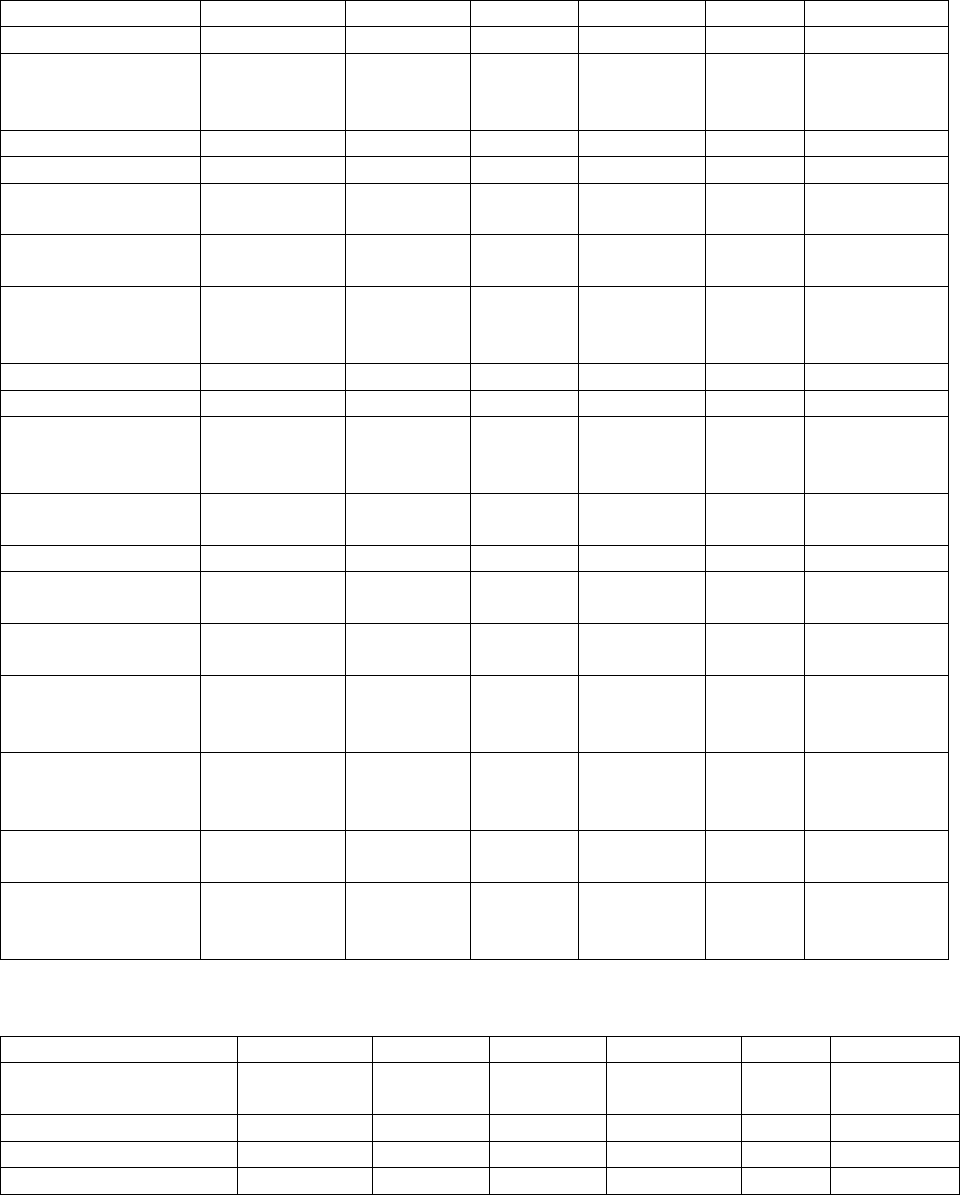
!
212!
Table 3-I: Comparison of Leagues’ Benefits
Benefit
NFL
MLB
NBA
NHL
CFL
MLS
Pension Plan
Yes
Yes
Yes
Yes
Yes
No
Pension Plan
Vesting
Requirement
3 years (post
1992)
1 day
3 years
1 day
9 games
NA
Severance Plan
Yes
No
No
No
No
No
401k Plan
Yes
Yes
Yes
Yes
No
Yes
Other Deferred
Compensation Plan
Yes
No
Yes
No
No
No
Health Insurance
(Current Players)
Yes
Yes
Yes
Yes
Yes
Yes
Health Insurance
(Former Players,
other than COBRA)
5 years
For life
potentially
For life
potentiall
y
For life
potentially
No
No
Life Insurance
Yes
Yes
Yes
Yes
Yes
Yes
Dental Insurance
Yes
Yes
Yes
Yes
Maybe
Yes
Health
Reimbursement
Account
Yes
No
Yes
No
No
No
Long Term Care
Insurance
Yes
No
Potentiall
y
No
No
No
Wellness Benefits
Many
Some
Some
None
None
None
Disability Benefits
(Current Players)
Yes
Yes
Yes
Yes
Maybe
Yes
Disability Benefits
(Former Players)
Yes
Yes
No
No
No
No
Neurocognitive
Disability Benefits
Yes
No
No
Only for
current
players
No
No
Workers’
Compensation
Yes
Partial
Yes
Yes
Prohibit
ed by
law
Yes
Education-Related
Benefits
Yes
No
Yes
Yes
No
For some
players
Joint Health-
Specific
Committee(s)
Yes
Yes
Yes
Yes
Yes
Yes
Table 4-I: Comparison of Leagues’ PES Policies
1800
Feature
NFL
MLB
NBA
NHL
CFL
MLS
Independent
administration
Yes
Yes
Yes
Yes
Yes
Yes
Urine tests permitted
Yes
Yes
Yes
Yes
Yes
Yes
Blood tests permitted
Yes
Yes
Yes
No
Yes
No
Maximum number of
24
No
Nine
No
No
No
!
213!
annual tests for player
without prior violation
maximum
maximum
maxim
um
maximum
Therapeutic Use
Exemptions available
Yes
Yes
Yes
Yes
Yes
No
Treatment available
No
No
Yes
No
Yes
Yes
Safe harbor for self-
referrals
No
No
No
No
Yes
No
Discipline for first
violation
Two–Six
games
80 games
25 games
20 games
Two
games
League
discretion
Discipline for second
violation
Ten games
162 games
55 games
60 games
Nine
games
League
discretion
Discipline for third
violation
Two years
Life
Two years
(subject to
reinstatem
ent)
Two years
One
year
League
discretion
Discipline for fourth
violation
NA
NA
NA
NA
Life
League
discretion
Confidential violations
Until
discipline
Until
discipline
Until
discipline
Until
discipline
Until
discipli
ne
Until
discipline
Neutral appeal rights
In part
Yes
Yes
Yes
Yes
No
Table 4-J: Comparison of Leagues’ Drugs of Abuse Policies
Feature
NFL
MLB
NBA
NHL
CFL
MLS
Independent
administration
Yes
Yes
Yes
Yes
No Policy
Yes
Urine tests permitted
Yes
Yes
Yes
Yes
No Policy
Yes
Blood tests permitted
No
No
No
No
No Policy
No
Maximum number of
annual tests for player
without prior violation
One
No tests
Six
No tests
No Policy
No
maximum
Therapeutic Use
Exemptions available
Yes
Yes
Yes
No
No Policy
No
Treatment available
Yes
Yes
Yes
Yes
No Policy
Yes
Safe harbor for self-
referrals
Yes
Maybe
Yes
Yes
No Policy
Yes
Discipline for first
violation
None
None
No
(Marijuana
); One year
for rookies
only or two
years
(other
drugs)
None
No Policy
Determined
by Program
Professiona
ls
evaluation
Discipline for second
violation
Fine
(Marijuana);
Four games
(other drugs)
15–25
games
$25,000
fine
(Marijuana
); 2 years
for rookies
Suspend
ed
during
treatmen
t
No Policy
League
discretion
!
214!
or self-
referrals
(other
drugs)
Discipline for third
violation
4–6 games
50–75
games
Five games
(Marijuana
)
Minimu
m of six
months
No Policy
League
discretion
Discipline for fourth
violation
10 games
(Marijuana);
One year
(other drugs)
At least
One year
Ten games
(Marijuana
)
Minimu
m of
one year
No Policy
League
discretion
Confidential violations
Yes
Yes
Yes
Yes
No Policy
Until
discipline
Neutral appeal rights
Yes
Yes
Yes
Yes
No Policy
No
Table 5-J: Comparisons of Leagues’ Compensation Statistics and Policies
NFL
MLB
NBA
NHL
CFL
MLS
Mean Annual
Salary
$2.7
million
$4.25
million
$6.9-8
million
$2.89
million
$80,000
$290,246
Mean Career
Length
5.0
years
1801
5.6
years
1802
4.8 years
1803
5.6 years
1804
3.2
years
1805
3.2 years
1806
Minimum
Salary (2016)
$450,000
$507,500
$543,471
$575,000
$52,000
$62,500
Maximum
Salary
No
No
Yes
Yes
No
No
Maximum
Contract Length
No
No
Yes
Yes
No
No
Unrestricted
Free Agency
Rights
After four
seasons
After six
seasons
After five
seasons for
first round
picks
Depends on
age and
experience
Upon
expiration
of rookie
contract
28 years old
and eight
years of
experience
Guaranteed
Compensation
~ 44%
~ 100%
~ 90%
For injury
and one-
third or two-
thirds of the
player’s
salary
Almost
none
For players
24 and older
with 1+
years’
experience
Salary Cap Type
Hard
Luxury
Tax
Soft and
Luxury Tax
Hard
Hard
Soft
Guaranteed
Share of
Revenue
Yes
No
Yes
Yes
No
No
APPENDIX C – GLOSSARY OF TERMS AND RELEVANT PERSONS AND INSTITUTIONS
88 Plan: A program that provides benefits for former NFL players suffering from dementia, ALS, or
Parkinson’s disease.
!
215!
401(k) Savings Plan: A retirement plan available to NBA players who can contribute a portion of their
salary, subject to the maximum amounts permitted by the Internal Revenue Code.
1807
NBA clubs match up
to 140% of players’ allowed contributions.
1808
ACC: See Accountability and Care Committee.
Accountability and Care Committee (“ACC”): A committee consisting of the NFL Commissioner or
his designee; the NFLPA Executive Director or his designee; and six additional members “experienced in
fields relevant to health care for professional athletes,” three appointed by the Commissioner and three by
the NFLPA Executive Director. The ACC is to “provide advice and guidance regarding the provision of
preventive, medical, surgical, and rehabilitative care for players by all clubs.”
1809
Accrued Season: Generally speaking, a season in which an NFL player is on a club’s roster for at least
six games.
AHMS: See Athlete Health Management System.
AMA: See American Medical Association.
American Medical Association (“AMA”): a voluntary professional association for physicians and the
source of the predominant code defining ethical medical practice.
Anti-Drug Program: The NBA-NBPA policy prohibiting players from using PES and drugs of abuse.
Athlete Health Management System (“AHMS”): The NHL’s electronic medical records system.
Big Four: A label sometimes used to collectively describe the NFL, MLB, NBA, and NHL, due to
similarities in their structures and positions in the American sports landscape.
Board of Certification for the Athletic Trainer: The accredited certification program for entry-level
athletic trainers, which sets the standards and codes of conduct for the practice of athletic training.
BOC: See Board of Certification for the Athletic Trainer.
Canadian Athletic Therapists Association (“CATA”): A voluntary professional membership
association for certified athletic trainers across all levels of competition in Canada. CATA’s American
counterpart is NATA.
Canadian Football League (“CFL”): A professional football league consisting of nine member clubs,
all of which are located in Canada. The CFL began play in 1958, has its headquarters in Toronto, and is
currently looking for a new Commissioner. The CFL’s 2015 revenues were an estimated $200 million.
Canadian Football League Players Association (“CFLPA”): A labor organization representing CFL
players. The CFLPA was formed in 1965,
1810
has its headquarters in Stoney Creek, Ontario; and is led by
President Scott Flory, a 15-year CFL veteran.
Canadian Interuniversity Sport: The organization that governs intercollegiate athletics in Canada. CIS’
American counterpart is the NCAA.
CATA: See Canadian Athletic Therapists Association.
CBA: See Collective Bargaining Agreement.
CFL: See Canadian Football League.
!
216!
CFLPA: See Canadian Football League Players Association.
CIS: See Canadian Interuniversity Sport.
Club: A professional sports franchise.
COBRA: See Consolidated Omnibus Budget Reconciliation Act.
Collective Bargaining Agreement (“CBA”): “A contract between an employer and a labor union
regulating employment conditions, wages, benefits, and grievances.”
1811
Each of the sports leagues is
governed by a CBA.
Commissioner: The Chief Executive Officer of a league.
Consolidated Omnibus Budget Reconciliation Act (“COBRA”): A federal law that requires
continuation coverage to be offered to covered employees, their spouses, former spouses, and dependent
children when group health coverage would otherwise be lost due to certain specific events, including, as
would be relevant in the NFL, “the termination (other than by reason of such employee’s gross
misconduct), or reduction of hours, of the covered employee’s employment.”
1812
Credited Season: Generally speaking, a season in which an NFL player is on a club’s roster for at least
three games.
Disability & Neurocognitive Benefit Plan: Provides eligible NFL players with disability benefits,
including benefits based on neurocognitive disability.
Disabled List (“DL”) (MLB): A roster designation for MLB players who are injured and are unable to
play. The MLB has a 60-day, 10-day, and 7-day DL. Players on the Disabled List do not count towards
the club’s 25-man roster.
Disabled List (“DL”) (MLS): A roster designation for MLS players who are injured and are unable to
play. The player must remain on the DL for a minimum of six matches.
DL: See Disabled List.
Draft: A process by which a league’s clubs (or, in the case of MLS, the league itself) select players to
join the league. Players selected are typically college or high school student-athletes, but, in some sports,
can also include international players.
eBIS: See Electronic Baseball Information System.
Electronic Baseball Information System (“eBIS”): An electronic system that MLB clubs use to
complete the Standard Form of Diagnosis for Disabled List applications and which links with players’
electronic medical records.
ESDI: See Exceptional Student-Athlete Disability Insurance Program.
Exceptional Student-Athlete Disability Insurance Program (“ESDI”): An NCAA insurance program
available to collegiate student-athletes who demonstrate that they have the potential to be selected in the
first three rounds of the NHL Draft, the first two rounds of the NFL Draft, or the first round of the NBA,
MLB, or Women’s National Basketball Association Draft, and which pays the student-athletes a lump
sum payment 12 months after determining that the player has suffered permanent total disability.
!
217!
Exclusive Rights Player: A player whose contract has expired but, because he only has a minimal
amount of experience—which varies among the leagues—can only sign a contract with his prior club
provided that club offers him a contract that meets the minimum requirements outlined in the CBA.
Exclusive Rights Players have no leverage and thus generally must accept the contract offered by the
club, which is typically for or near the league minimum.
Extended Injury Protection: An Injury Protection benefit that permits an NFL player to earn 50% of his
salary up to $500,000 for the second season after suffering an injury that prevented the player from
continuing to play. See also Injury Protection.
Fédération Internationale de Médecine du Sport (“FIMS”): The world’s leading sports medicine
organization, comprised of national sports medicine associations across five continents which seeks to
maximize athlete health and performance.
FIMS: See Fédération Internationale de Médecine du Sport.
Former Player Life Improvement Plan: A medical plan that permits qualifying former NFL players
(and in some cases their dependents) not otherwise covered by health insurance to receive reimbursement
for medical costs for “joint replacements, prescription drugs, assisted living, Medicare supplemental
insurance, spinal treatment, and neurological treatment.”
Free Agency: A system by which players are able to sign contracts with new clubs after a certain number
of seasons played, provided their prior contract is expired. See Unrestricted Free Agent and Restricted
Free Agent.
Health and Injury Tracking System (“HITS”): An electronic system linked to MLB players’ electronic
medical records that allows MLB to monitor, study, and analyze injuries in baseball.
HealtheAthlete: An electronic medical record system used by NBA and MLS clubs.
Health Reimbursement Account (NBA): A program that helps to pay out-of-pocket healthcare expenses
after players are no longer employed by an NBA club.
Health Reimbursement Account (NFL): A program that helps to pay out-of-pocket healthcare expenses
after players are no longer employed by an NFL club and after the period of extended medical coverage
under the NFL Player Insurance Plan that is paid by the NFL has ended.
HITS: See Health and Injury Tracking System.
Injured List: A roster designation for CFL players who are injured and are unable to play. The CFL has
either a six-game or one-game Injured List. Players on either Injured List do not count towards the club’s
44-man roster.
Injured Non-Roster List: A roster designation for NHL players who fail the pre-season physical. Players
on the Injured Non-Roster List do not count towards the club’s 23-man roster.
Injured Reserve (“IR”) (NFL): A roster designation for players who are injured and are unable to return
that season, with the exception of one player per season per club who can be placed on the IR but
designated to be able to return. Players on IR do not count towards the club’s 53-man Active/Inactive
List.
Injured Reserve (“IR”) (NHL): A roster designation for players who are injured and are unable to return
for a minimum of seven days. Players on IR do not count towards the club’s 23-man roster.
!
218!
Injury Protection: A benefit available to NFL players where the player has met the following criteria:
(1) “[t]he player must have been physically unable, because of a severe football injury in an NFL game or
practice, to participate in all or part of his club’s last game of the season, as certified by the club physician
following a physical examination after the last game; or the player must have undergone club-authorized
surgery in the off-season following the season of injury; and (2) [t]he player must have undergone
whatever reasonable and customary rehabilitation treatment his club required of him during the off-season
following the season of injury; and (3) [t]he player must have failed the pre-season physical examination
given by the club physician for the season following the season of injury because of such injury and as a
result his club must have terminated his contract for the season following the season of injury.” In 2016,
an NFL player could receive Injury Protection in “an amount equal to 50% of his Paragraph 5 Salary for
the season following the season of injury, up to a maximum payment of” $1,150,000. A player is only
entitled to Injury Protection once in his career.
1813
See also Extended Injury Protection.
Injury Report: Generally, a list of injured players, each injured player’s type or location of injury, and
the injured player’s status for the upcoming game. The detail provided by each league’s Injury Report
varies.
Intervention Program: A program for testing, evaluating, and treating NFL players pursuant to the
Substance Abuse Policy.
IR: See Injured Reserve.
Joint Committee on Player Safety and Welfare (“Joint Committee”): An NFL-NFLPA committee
consisting of three club representatives and three NFLPA representatives which discusses “player safety
and welfare aspects of playing equipment, playing surfaces, stadium facilities, playing rules, player-coach
relationships, and any other relevant subjects.”
1814
The Joint Committee is merely advisory and has no
binding decision-making authority.
Joint Committee on Players’ Safety and Welfare: A CFL-CFLPA committee which discusses player
safety and welfare aspects of playing equipment, playing surfaces, stadium facilities, playing rules,
player-coach relationships, drug abuse prevention programs, and any other relevant subjects.
Joint Drug Prevention and Treatment Program (“Joint Program”): The MLB-MLBPA policy
prohibiting players from using PES and drugs of abuse.
Joint Health and Safety Committee: An NHL-NHLPA committee consisting of five members from
each party, and which is responsible for “mak[ing] recommendations to the NHL and the NHLPA for
consideration and approval regarding all issues related to Player health and regarding the safety of the
playing environment.”
1815
Joint Program: See Joint Drug Prevention and Treatment Program.
Joint Safety Committee: An MLS-MLSPU committee that is responsible for making “recommendations
to the Commissioner concerning safety procedures.”
1816
Legacy Benefit: As part of the 2011 CBA, the NFL contributed $620 million in benefits to players who
played prior to 1993 through credits as part of the Retirement Plan. Players who played before 1975
received a $124-per-month credit and those who played between 1975 and 1992 received a $108-per-
month credit.
Long Term Care Insurance Plan: Provides medical insurance to cover the costs of long-term care for
NFL players (but not their family members).
!
219!
Major League Baseball (“MLB”): The world’s premier professional baseball organization, consisting of
30 member clubs. MLB began play in 1903, has its headquarters in New York City, and is led by
Commissioner Rob Manfred. MLB’s 2015 revenues were an estimated $10 billion.
Major League Baseball Players Association (“MLBPA”): A labor organization representing MLB
players. The MLBPA was formed in 1953,
1817
has its headquarters in New York City and is led by
Executive Director Tony Clark, a 15-year MLB veteran.
Major League Baseball Players Benefit Plan: A comprehensive plan to MLB players and former MLB
players that includes pension, investment, disability, and insurance components.
Major League Soccer (“MLS”): A professional soccer league consisting of 20 clubs. MLS began play in
1996, has its headquarters in New York City, and is led by Commissioner Don Garber. MLS’ 2016
revenues were an estimated $600 million.
Major League Soccer Players Union (“MLSPU”): A labor organization representing MLS players. The
MLSPU was formed in 2003,
1818
has its headquarters in Bethesda, Maryland, and is led by Executive
Director Bob Foose.
MLB: See Major League Baseball.
MLB Team Physicians Association (“MLBTPA”): A voluntary professional membership association
for MLB club doctors. MLBTPA’s “mission is to maintain the earned trust of the athletes and teams of
Major and Minor League Baseball, as well as the public, by providing the highest quality medical care
and services aimed at securing and enhancing their safety, health and well-being.”
1819
MLBTPA: See MLB Team Physicians Association.
MLS Team Physicians Society (“MLSTPS”): A voluntary professional membership association for
MLS club doctors. MLSTPS’ stated mission is “[t]o be a global leader and collaborator in the science of
soccer medicine focused on research, education and athlete care.”
1820
MLS: See Major League Soccer.
MLSTPS: See MLS Team Physicians Society.
NATA: See National Athletic Trainers Association.
National Athletic Trainers Association (“NATA”): A voluntary professional membership association
for certified athletic trainers across all levels of competition. NATA’s stated mission “is to enhance the
quality of health care provided by certified athletic trainers and to advance the athletic training
profession.” NATA’s Canadian counterpart is CATA.
National Basketball Association (“NBA”): The world’s premier professional basketball league,
consisting of 30 member clubs. The NBA began play in 1946, has its headquarters in New York City, and
is led by Commissioner Adam Silver. The NBA’s 2016–17 revenues are projected to be $5.2 billion.
National Basketball Athletic Trainers Association (“NBATA”): A voluntary professional membership
association for NBA club athletic trainers.
National Basketball Players Association (“NBPA”): A labor organization representing NBA players.
The NBPA was formed in 1954,
1821
has its headquarters in New York City, and is led by Executive
Director Michelle Roberts.
!
220!
National Collegiate Athletic Association (“NCAA”): A non-profit unincorporated association
headquartered in Indianapolis through which America’s colleges and universities govern their athletic
programs. The NCAA consists of over 1,200 member institutions, all of which participate in the creation
of NCAA rules and voluntarily submit to its authority.
National Hockey League (“NHL”): The world’s premier professional hockey league, consisting of 30
members clubs. The NHL began play in 1917, has its headquarters in New York City, and is led by
Commissioner Gary Bettman. The NHL’s 2015–16 revenues were an estimated $4.1 billion.
National Hockey League Players Association (“NHLPA”): A labor organization representing NHL
players. The NHLPA was formed in 1957, has its headquarters in Toronto, and is led by Executive
Director Don Fehr, who served as Executive Director of the MLBPA from 1985–2009.
National Football League (“NFL”): The world’s premier professional football league, consisting of 32
member clubs. The NFL began play in 1920, has its headquarters in New York City, and is led by
Commissioner Roger Goodell. The NFL’s 2017 revenues are estimated to reach $14 billion.
National Football League Players Association (“NFLPA”): A labor organization representing NFL
players. The NFLPA was formed in 1956,
1822
has its headquarters in Washington, DC, and is led by
Executive Director DeMaurice Smith.
National Labor Relations Act (“NLRA”): A federal labor law statute which governs labor relations
between employees and employers in the private sector and obligates both sides to negotiate in good faith
concerning the wages, hours, and other terms and conditions of employment.
National Labor Relations Board (“NLRB”): An independent agency of the United States government
responsible for administering and enforcing the provisions of the NLRA, including investigating and
remedying unfair labor practices.
NBA: See National Basketball Association.
NBATA: See National Basketball Athletic Trainers Association.
NBA Team Physicians Society (“NBATPS”): A voluntary professional membership association for
NBA club doctors.
NBATPS: See NBA Team Physicians Society.
NCAA: See National Collegiate Athletic Association.
NFL: See National Football League.
NFL Injury Surveillance System (“NFLISS”): The standardized system, created in 1980, used by the
NFL and NFL clubs to track and analyze NFL injuries and to provide data for medical research. Injury
information is entered by club athletic trainers. Since 2011, the NFLISS is managed by the international
biopharmaceutical services firm Quintiles.
NFLISS: See NFL Injury Surveillance System.
NFLPA: See National Football League Players Association.
NFL Physicians Society (“NFLPS”): A voluntary professional membership association for NFL club
doctors. NFLPS’ mission is “to provide excellence in the medical and surgical care of the athletes in the
!
221!
National Football League and to provide direction and support for the athletic trainers in charge of the
care for these athletes.”
NFLPS: See NFL Physicians Society.
NHL: See National Hockey League.
NHL Team Physicians Society (“NHLTPS”): A voluntary professional membership association for
NHL club doctors.
NHLTPS: See NHL Team Physicians Society.
NLRA: See National Labor Relations Act.
NLRB: See National Labor Relations Board.
Paragraph 5 Salary: An NFL player’s base salary. Paragraph 5 salaries are typically non-guaranteed,
except for better players and even then only for some seasons of the player’s contract.
PBATS: See Professional Baseball Athletic Trainers Society.
PED: See Performance-Enhancing Substance(s).
PES: See Performance-Enhancing Substance(s).
PES Policy: See Policy on Performance-Enhancing Substances.
Performance-Enhancing Substance(s) (“PES”): Substances that have the potential to enhance a
player’s performance in ways that the league, sports, and/or medical community has determined to be
unfair, unnatural, and/or unsafe. Also sometimes referred to as “Performance-Enhancing Drugs.”
PFATS: See Professional Football Athletic Trainers Society.
PHATS: See Professional Hockey Athletic Trainers Society.
Physically Unable to Perform (“PUP”) List: A roster designation for NFL players who have failed the
pre-season physical and are unable to participate in training camp but are expected to be able to play later
in the season. A player on the PUP List cannot practice or play until after the sixth game of the regular
season and does not count towards the club’s 53-man Active/Inactive List during that time.
Player Annuity Program: An NFL plan that provides deferred compensation to players.
Player Insurance Plan: An NFL player insurance plan that provides players and their family with life
insurance, accidental death and dismemberment insurance, medical coverage, dental coverage, and
wellness benefits. The wellness benefits include access to clinicians for mental health, alcoholism, and
substance abuse; child and parenting support services; elder care support services; pet care services; legal
services; and, identity theft services.
Players’ Pension Plan: A plan that provides pension benefits to NBA players who have at least three
years of service in the league.
Policy and Program on Substances of Abuse (“Substance Abuse Policy”): The NFL-NFLPA policy
prohibiting players from using common street drugs, such as cocaine, marijuana, amphetamines, opiates,
!
222!
opioids, PCP, and MDMA (ecstasy). The Substance Policy includes treatment and disciplinary
provisions.
Policy on Performance-Enhancing Substances (“PES Policy”): The NFL-NFLPA policy prohibiting
players from using PES. The PES Policy includes disciplinary but not treatment provisions.
Post-Career Income Plan: A retirement plan that purchases annuities for NBA players to provide a
source of post-employment income.
Professional Baseball Athletic Trainers Society (“PBATS”): A voluntary professional membership
association for MLB club athletic trainers. “PBATS mission is to serve as an educational resource for the
Major League and Minor League Baseball athletic trainers. PBATS serves its members by providing for
the continued education of the athletic trainer as it relates to the profession, helping to improve his
understanding of sports medicine so as to better promote the health of his constituency—professional
baseball players.”
1823
Professional Football Athletic Trainers Society (“PFATS”): A voluntary professional membership
association for NFL club athletic trainers.
Professional Hockey Athletic Trainers Society (“PHATS”): A voluntary professional membership
association for NHL club athletic trainers.
Professional Soccer Athletic Trainers Society (“PSATS”): A voluntary professional membership
association for MLS club athletic trainers.
Prohibited Substances Committee: A committee consisting of one NBA representative, one NBPA
representative, and three jointly selected representatives who advise the NBA and NBPA on its anti-drug
policy.
PSATS: See Professional Soccer Athletic Trainers Society.
Restricted Free Agent: A player whose contract has expired and who can sign a contract with any club.
However, because the player has only a certain (but more than minimal) amount of experience (which
varies among the leagues), the player’s prior club is entitled to a right of first refusal on a contract offered
by another club. But, the prior club only retains the right of first refusal if it had already made an offer
meeting certain minimal criteria outlined in the CBA (“Qualifying Offer”). Additionally, if the player
signs with a new club, his prior club will be entitled to some form of compensation, typically draft picks.
Restricted Free Agents have minimal leverage as clubs generally prefer not to pay the required
compensation to the prior club. See also Unrestricted Free Agent.
Retiree Medical Plan: An NBA plan that provides health insurance to former NBA players.
Retirement Plan (NFL): An NFL retirement plan that provides eligible players with retirement benefits,
and offers survivor benefits for players’ wives and family.
Retirement Plan (NHL): An NHL retirement plan that provides eligible players with retirement and
disability benefits.
Safety and Health Advisory Committee (“SHAC”): A committee comprised of representatives of MLB
clubs and the MLBPA, formed to “deal with emergency safety and health problems” and to review player
working conditions.
1824
!
223!
Salary Cap: Generally, the maximum amount of money that a club can spend on its players’ salaries
collectively in a season. In MLB, the “salary cap” is called the Tax Threshold.
Second Career Savings Plan: A 401(k) plan that helps NFL players save for retirement in a tax-favored
manner. All NFL players are eligible for the Plan, regardless of the number of Credited Seasons.
Severance Pay: A benefit available to NFL players as severance for each Credited Season.
Substance Abuse Policy: See Policy and Program on Substances of Abuse.
Termination Pay: An NFL player benefit whereby a player who has at least four years of credited
service under the Retirement Plan is eligible to receive the unpaid balance of his Paragraph 5 Salary for a
season after having had his contract terminated during that season, provided he was on the club’s
Active/Inactive List for at least one game that season. A player is entitled to Termination Pay only once
during his career.
Therapeutic Use Exemption (“TUE”): A policy that permits an athlete to use a banned substance
without violating a drug policy for the treatment of a diagnosed medical condition.
TUE: See Therapeutic Use Exemption.
Tuition Assistance Plan: A benefit that entitles qualifying current and former NFL players to
reimbursement for tuition, fees, and books from attending an eligible education institution.
UEFA: See Union of European Football Associations.
Union of European Football Associations (“UEFA”): A European soccer organization whose members
generally include the best soccer clubs in the world and who play in some of the best soccer leagues in the
world (such as the English Premier League and Spain’s La Liga).
Unrestricted Free Agent: A player whose contract has expired and, because he has a higher level of
experience (defined variously across the leagues), can sign a contract with any club without his prior club
retaining any rights concerning the player. Unrestricted Free Agents have far more leverage and options
as compared to Exclusive Rights Players or Restricted Free Agents. Becoming an Unrestricted Free Agent
is an important opportunity that allows players to offer their services to any and all clubs at the highest
price the market will bear (within the confines of the CBA). See also Free Agency and Restricted Free
Agent.
VEBA: See Voluntary Employees’ Beneficiary Association.
Voluntary Employees’ Beneficiary Association (“VEBA”): Provides employees with benefits as
permitted under Section 501(c)(9) of the Internal Revenue Code, such as “life, sick, accident, or similar
benefits [for] members or their dependents, or designated beneficiaries.”
1825
WADA: See World Anti-Doping Agency.
World Anti-Doping Agency: An international agency funded by sports organizations and governments
with its principal focus on eliminating the use of PES in sports. WADA publishes annually a “Prohibited
List” that lists prohibited substances. The WADA Code and the Prohibited List are the governing anti-
doping documents of all Olympic sports organizations and most sports organizations worldwide.

!
224!
Workers’ Compensation: A state-based system which provides workers injured during the course of
their employment with wages and medical benefits and which, as a tradeoff, generally bars employees
from suing their employers and co-employees for negligence.
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1
The applicable contract language provides that the NFLPA is permitted to review publications 30 days in advance
“for the sole purpose of identifying any unauthorized use of Confidential Information.”
2
Other Law and Ethics projects include: (1) our Report, Protecting and Promoting the Health of NFL Players: Legal
and Ethical Analysis and Recommendations (2016); (2) our Report, NFL Player Health: The Role of Club Doctors, 46
Hastings Center Rep. 2 (2016); (3) our law review article, Evaluating NFL Player Health and Performance: Legal and
Ethical Issues, 165 Univ. Penn. L. Rev. 227 (2017); and, (4) a qualitative interview study (“listening tour”) with players
and their families to better understand their legal and ethical concerns related to health and well-being.
3
This Report is part of Law and Ethics Initiative of the Football Players Health Study at Harvard University. The 2011
Collective Bargaining Agreement (CBA) between the NFL and NFLPA allocated funds for research, and in 2014, the
NFLPA and Harvard University entered into an agreement to create and support The Football Players Health Study
using a portion of these funds. The contract governing this project protects our academic integrity as researchers; no
external party has any editorial control over our work. A version of this Report was shared with the NFLPA prior to
publication. We also invited the NFL and the other leagues and unions discussed in this Report to review the Report
prior to its publication and to provide comments. As detailed in the Report, some of the leagues and unions accepted
our invitation while others did not. The NFLPA was treated the same as other stakeholders, with the exception of a
contractually guaranteed 30-day review to ensure that we did not use any confidential information. We considered all
feedback provided to us from all stakeholders but retained final editorial control. The content is solely the
responsibility of the authors and does not necessarily represent the official views of the NFLPA or Harvard University.
4
As discussed in the full Report, there was no publicly available data on CFL injuries.
5
As discussed in the full Report, there is no recent data concerning player injuries in MLS. However, there is injury
data from the Union of European Football Associations (“UEFA”), a European soccer organization whose members
generally include the best soccer clubs in the world. While UEFA and MLS are different soccer organizations, we
nonetheless believe that data from UEFA, an elite soccer organization like the MLS, can be instructive of the injury
rates in MLS. Indeed unless and until MLS makes its own data public, we think the UEFA data provides the best
proxy estimate of the underlying injury rate in that league.
6
We emphasize that this statistic is a mean of all player positions. As discussed in the full Report, we know that
rates vary depending on a player’s position. Unfortunately, we do not have sufficient data to do position-by-position
analysis. Nevertheless, even in the absence of that data we think the comparison of means is useful.
7
While NFL clubs do provide workers’ compensation benefits, as discussed in the full Report, the NFL and its clubs
have sponsored legislation in several states to restrict players’ workers’ compensation benefits.
8
2011 CBA, Art. 12, § 5.
9
Nat’l Football League Players Ass’n, Request for Proposals Advancing the Frontiers of Research in Professional
Football (2012), § 1(a).
10
Other Law and Ethics projects include: (1) our Report, Protecting and Promoting the Health of NFL Players: Legal
and Ethical Analysis and Recommendations (2016); (2) our Report, NFL Player Health: The Role of Club Doctors, 46
Hastings Center Rep. 2 (2016); (3) our law review article, Evaluating NFL Player Health and Performance: Legal and
Ethical Issues, 165 Univ. Penn. L. Rev. 227 (2017); and, (4) a qualitative interview study (“listening tour”) with players
and their families to better understand their legal and ethical concerns related to health and well-being.
11
The players’ share of NFL revenues is referred to as the Player Cost Amount. 2011 CBA, Art. 12, § 6(c)(i). The
Football Players Health Study is funded from a pool of money known as the Joint Contribution Amount. See 2011
CBA, Art. 12, § 5. If the NFL generates new revenue streams, the players are entitled to 50% of the net revenues
from those new ventures less 47.5% of the Joint Contribution Amount. 2011 CBA, Art. 12, § 6(c)(ii). Thus, if the NFL
generates new revenue streams, the amount that is passed on to the players is reduced by 47.5% of the Joint
Contribution Amount, which includes the Football Players Health Study.
12
Alvaro Pascual-Leone and Lee M. Nadler, Let’s not kill football yet, Pitt. Post. Gazette, May 10, 2015,
http://www.post-gazette.com/opinion/Op-Ed/2015/05/10/Let-s-not-kill-football-yet-Yes-players-get-injured-but-the-
scope-of-the-problem-is-far-from-clear/stories/201505100034, archived at http://perma.cc/V3DN-Z2F3.
13
Mike Florio, NFL will reach $14 billion in 2017 revenue, ProFootballTalk (Mar. 6, 2017, 11:29 AM),
http://profootballtalk.nbcsports.com/2017/03/06/nfl-will-reach-14-billion-in-2017-revenue/, archived at
https://perma.cc/X57A-VRXU.
Mark Leibovich, Roger Goodell’s Unstoppable Football Machine, N.Y. Times, Feb. 3, 2016,
http://www.nytimes.com/2016/02/07/magazine/roger-goodells-unstoppable-football-machine.html?_r=0, archived at
https://perma.cc/Y7L5-A99L.

!
225!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
14
MLB consists of the National League and American League. The National League began play in 1876 and the
American League in 1901. The leagues merged to create Major League Baseball in 1903. See History of baseball in
the United States, BASEBALL-REFERENCE.COM, http://www.baseball-
reference.com/bullpen/History_of_baseball_in_the_United_States (last visited Mar. 10, 2016), archived at
https://perma.cc/DSK5-6VRN.
15
Maury Brown, MLB Sees Record Revenues Approaching $10 Billion for 2016, Forbes (Dec. 5, 2016, 3:22 PM),
http://www.forbes.com/sites/maurybrown/2016/12/05/mlb-sees-record-revenues-approaching-10-billion-for-
2016/#7704e2e21845, archived at https://perma.cc/775E-WE9A.
16
Dan Feldman, Report: NBA Revenue Projected to Reach $8 Billion Next Season, Pro Basketball Talk (Sep. 16,
2016, 10:05 AM), http://nba.nbcsports.com/2016/09/16/report-nba-revenue-projected-to-reach-8-billion-next-season/,
archived at https://perma.cc/73NP-QRJN.
17
See The Business of Hockey, Forbes (Nov. 30, 2016), http://www.forbes.com/nhl-valuations/list/, archived at
https://perma.cc/545K-NQBV (listing NHL clubs’ estimated revenues).
18
Andrew Bucholtz, What percentage of league-wide revenues did CFL players get in 2013 under the old CBA?,
Yahoo! Sports Can. (June 9, 2014, 6:49 PM), https://ca.sports.yahoo.com/blogs/cfl-55-yard-line/percentage-league-
wide-revenues-did-cfl-players-2013-224954281.html, archived at http://perma.cc/F5NU-FWE3.
19
See Fraser v. Major League Soccer, L.L.C., 284 F.3d 47, 53-55 (1st Cir. 2002) (discussing MLS’ structure and
operations).
20
See Chris Smith, Major League Soccer’s Most Valuable Teams 2016, Forbes (Sep. 7, 2016, 10:32 AM),
http://www.forbes.com/sites/chrissmith/2016/09/07/major-league-soccers-most-valuable-teams-2016-new-york-
orlando-thrive-in-first-seasons/, archived at https://perma.cc/K7B6-DJ86.
21
See Michael A. McCann, The NBA and the Single Entity Defense: A Better Case? 1 Harv. J. Sports & Ent. L. 39,
40 (2010) (referring to the NFL, MLB, NBA and NHL as the “Big Four“); Marc Edelman, How to Curb Professional
Sports Bargaining Power Vis-à-Vis the American City, 2 Va. Sports & Ent. L.J. 280, 291 (2003).
22
Boxing, in which fighters are subjected to repeated hits to the head, draws obvious comparisons to playing in the
NFL. Of note, the Muhammad Ali Boxing Reform Act provides for certain safety standards for professional boxing
matches. 15 U.S.C. § 6304.
23
To avail themselves of federal labor laws, the unions must be certified by the National Labor Relations Board
(“NLRB”). Here, we provide the dates the players associations were formed and began working on behalf of the
players, which were generally several years before they gained official recognition from the NLRB.
24
History, Nat’l Football League Players Ass’n, https://www.nflpa.com/about/history (last visited Aug. 7, 2015),
archived at https://perma.cc/3D2R-8EQG?type=pdf [hereinafter “NFLPA History”].
25
See Glenn M. Wong, Essentials of Sports Law, § 11.3 (4th ed. 2010) (providing history of the unions in the Big
Four sports leagues).
26
Id.
27
Id.
28
Id.
29
Id.
30
A “bargaining unit” is the group of employees sufficiently similar to be represented by the union. See 29 U.S.C. §
159(b) (describing the factors for determining whether a bargaining unit is appropriate for collective bargaining).
31
29 U.S.C. § 159(a). Similarly, Canada’s Labour Code declares that unions certified by the Canada Industrial
Relations Board “has exclusive authority to bargain collectively on behalf of the employees in the bargaining unit[.]”
Canada Labour Code, § 36(1)(a).
32
See, e.g., A. Jason Huebinger, 16 Sports Law. J. 279, 281-82 (2009); Matthew Levine, Despite His Antics, T.O.
Has a Valid Point: Why NFL Players Deserve a Bigger Piece of the Pie, 13 Vill. Sports & Ent. L.J. 425, 435-36 (2006);
Mark Bradley, NFL players may hate Roger Goodell, but he’s their biggest ally, Atl. J.-Const., Jun. 4, 2012, available
at 2012 WLNR 28612021; Larry Brooks, Head-Less Iceman Lead to the Slaughter, N.Y. Post, Aug. 15, 2010,
available at 2010 WLNR 16396767 Jon Saraceno, Mawae’s labor of love: Fighting for players, USA Today, Oct. 21,
2010, available at 2010 WLNR 21102155.
33
Indeed, DeMaurice Smith, Executive Director of the NFLPA, has effectively admitted as much. At a public event in
2017, Smith stated that he “aspire[s] for our union to be as strong as the baseball union.” See University of Houston,
Health Law & Policy Institute, Medical and Legal Ethics in the NFL and Sports (Jan. 31, 2017),
http://www.uh.edu/infotech/services/streaming-media/events/hlpi/ (last visited Feb. 1, 2017), archived at
https://perma.cc/K7JK-DKG5.
34
Throughout this Report, we will refer to the CBAs by years, such as the 1968 CBA, 1993 CBA, or 2011 CBA. The
years reference the dates the CBAs became effective, which is usually, but not always, the year in which the CBA
was agreed to, i.e., some CBAs had retroactive application.
35
!Bill!Baer,!Report:(Owners,(Union(Agree(on(New(Collective(Bargaining(Agreement,!Hard ball!Talk!(Nov.!30 ,!2016,!
8:51! PM! EDT),! http://mlb.nbcsports.com/2016/11/30/report-owners-union-agree-on-new-collective-bargaining-
agreement/, archived at https://perma.cc/3JRF-PTYF.

!
226!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
36
MLBPA, MLB Announce Details of New Labor Agreement, MLBPA (Dec. 2, 2016),
http://www.mlbplayers.com/ViewArticle.dbml?DB_OEM_ID=34000&ATCLID=211336390, archived at
https://perma.cc/4XUA-2DAW.
37
Craig Calcaterra, Owners, Players Ratify New Collective Bargaining Agreement, Hardball Talk (Dec. 14, 2016, 5:16
AM EDT), http://mlb.nbcsports.com/2016/12/14/owners-ratify-new-collective-bargaining-agreement-29-1/, archived at
https://perma.cc/YYK2-GLSR.!
38
Email from Julie Grand, NHL, Deputy General Counsel, to authors (Nov. 1, 2016).
39
During the course of our research, both the NHL and CFL were defending themselves in lawsuits brought by former
players alleging that the leagues had acted negligently concerning player concussions. Nevertheless, we do not
believe our requests concerned issues relevant to those cases nor did either league indicate the ongoing litigation
was the reason for their decisions not to cooperate. Additionally, the NFL was and is the subject of more litigation
than either the NHL or CFL, but it substantially cooperated with our requests related to this Report.
40
The 2011 NFL CBA expires in March 2021.
41
Social Determinants of Health, World Health Org., http://www.who.int/social_determinants/sdh_definition/en/ (last
visited Aug. 2, 2016), archived at http://perma.cc/USS7-8C9J; see also Michael Marmot & Richard G. Wilkinson,
Social Determinants of Health (2d ed. 2005); For discussions of the relationship between these social determinants
and ethics and political philosophy, see, e.g., Sridhar Venkatapuram, Health Justice: An Argument from the
Capabilities Approach (2011); Norman Daniels, Just Health: Meeting Health Needs Fairly (2007); Madison Powers &
Ruth Faden, Social Justice: The Moral Foundations of Public Health and Health Policy (2006).
42
See NFL Total Wellness, NFL Player Engagement.com, https://www.nflplayerengagement.com/total-wellness/ (last
visited Aug. 7, 2015), archived at https://perma.cc/Z368-BBV4.
43
The AMA’s Code of Medical Ethics can be found on its website at http://www.ama-assn.org/ama/pub/physician-
resources/medical-ethics/code-medical-ethics.page (last visited Aug. 22, 2016), archived at http://perma.cc/8JJ4-
MYJX.
44
FIMS’ Code of Ethics is available from its website at http://www.fims.org/en/general/code-of-ethics. FIMS also
published a Team Physician Manual which is one of the preeminent manuals for sports injuries and also covers the
same ethical considerations espoused in its Code of Ethics.
45
See NATA Code of Ethics, Nat’l Athletic Trainers Ass’n, Sept. 28, 2005, http://www.nata.org/codeofethics, archived
at http://perma.cc/7ZXQ-KP5U.
46
See, e.g., John Lantos, Ann Marie Matlock, David Wendler, Clinician Integrity and Limits to Patient Autonomy, 305
J. Am. Med. Ass’n 495-9 (Feb. 2, 2011) (“Respect for patient autonomy plays a central role in modern clinical ethics”);
Simon N. Whitney, Amy L. McGuire, Laurence B. McCullough, A Typology of Shared Decision Making, Informed
Consent, and Simple Consent, 140 Ann. Intern. Med 54-59 (2003) (“Enhancing patient choice is a central theme of
medical ethics and law.”); Cathy Charles, Amiram Gafni, Tim Whelan, Decision-making in the physician-patient
encounter: revisiting the shared treatment decision-making model, 49 Social Science & Medicine 651–61 (1999)
(emphasizing the need to respect differences in patient preferences). See also Stedman’s Medical Dictionary (28th
ed. 2006) (defining “autonomy” as “[t]he condition or state of being autonomous, able to make decisions unaided by
others.”); Black’s Law Dictionary (9th ed. 2009) (defining “autonomy” as: “the right of self-government”; “an
individual’s capacity for self-determination.”)
47
Indeed, as part of our prior Report, Protecting and Promoting the Health of NFL Players: Legal and Ethical Analysis
and Recommendations, we included a Patient Bill of Rights for NFL Players, modeled on the Patient’s Bill of Rights
common in hospitals and other healthcare settings.
48
See Mark A. Hall, et al., Health Care Law and Ethics 168–69 (2003) (collecting cases and statutes discussing
doctors’ obligations to keep patient information confidential); AMA Code, Fourth Principle (“A physician shall respect
the rights of patients, colleagues, and other health professionals, and shall safeguard patient confidences and privacy
within the constraints of the law.”)
49
See Alexander Cornwell, Trapped: Missouri Legislature Seeks to Close Workers’ Compensation Loophole with
Some Co-Employees Still Inside, 77 Mo. L. Rev. 235, 235 (2012); David J. Krco, Case Note: Torts – Narrowing the
Window: Refining the Personal Duty Requirement for Coemployee Liability Under Minnesota’s Workers’
Compensation System – Stringer v. Minnesota Vikings Football Club, LLC, 33 Wm. Mitchell L. Rev. 739, 739 (2007);
John T. Burnett, The Enigma of Workers’ Compensation Immunity: A Call to the Legislature for a Statutorily Defined
Intentional Tort Exception, 28 Fla. St. U. L. Rev. 491, 497 (2001).
50
See Lotysz v. Montgomery, 309 A.D.2d 628 (N.Y.App. 2003) (NFL player’s medical malpractice claim against club
doctor barred by state workers’ compensation statute); Daniels v. Seattle Seahawks, 92 Wash.App. 576 (Wash.App.
1998) (same); Hendy v. Losse, 54 Cal.3d 723 (Cal. 1991) (same); Rivers v. New York Jets, 460 F.Supp. 1233
(E.D.Mo. 1978) (NFL player’s claim that club wrongfully concealed the true nature of player’s condition barred by
workers’ compensation statute); Brinkman v. Buffalo Bills Football Club Division of Highwood Service, Inc., 433
F.Supp. 699 (W.D.N.Y. 1977) (NFL player’s claim that club failed to provide adequate medical care barred by
workers’ compensation law). See also Bryant v. Fox, 162 Ill.App.3d 46 (Ill.App. 1987) (NFL player’s medical
malpractice claim against club doctor not barred by workers’ compensation statute where evidence established that
doctor was an independent contractor); Pam Louwagie and Kevin Seifert, Stringer claims against Vikings dismissed,

!
227!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
Newspaper of the Twin Cities (Minneapolis, MN), Apr. 26, 2003, available at 2003 WLNR 14250471 (medical
malpractice claims against club doctors barred by workers’ compensation statute). Martin v. Casagrande, 159 A.D.2d
26 (N.Y.App. 1990) (NHL player’s claim that club doctor and general manager conspired to withhold information
about player’s medical condition barred by workers’ compensation statute); Bayless v. Philadelphia National League
Club, 472 F.Supp. 625 (E.D.Pa. 1979) (former MLB player’s claim that club negligently administered pain-killing drugs
barred by workers’ compensation statute).
51
See Stringer v. Minnesota Vikings Football Club, LLC, 705 N.W.2d 746 (Minn. 2005) (estate of former NFL player
against athletic trainers barred by workers’ compensation statute); McLeod v. Blase, 290 Ga.App. 337 (Ga.App.
2008) (former NBA player’s claim against athletic trainer for alleged negligent treated barred by workers’
compensation statute).
52
See Memorandum and Order, Stringer v. Minnesota Vikings Football Club, LLC, No. 02-415, at 11-14
(Minn.Dist.Ct. Apr. 25, 2003) (denying club doctor’s motion to dismiss certain claims on ground that doctor was
independent contractor); Bryant v. Fox, 162 Ill.App.3d 46 (Ill.App. 1987) (NFL player’s medical malpractice claim
against club doctor not barred by workers’ compensation statute where evidence established that doctor was an
independent contractor).
53
Lawsuits against clubs are difficult to pursue. The CBAs present the biggest obstacle against any such claim.
Common law claims such as negligence are generally preempted by the Labor Management Relations Act (“LMRA”).
29 U.S.C. § 185. The LMRA bars or “preempts” state law claims where the claim is “substantially dependent upon
analysis of the terms” of a CBA, i.e., where the claim is “inextricably intertwined with consideration of the terms of the”
CBA. Allis-Chambers Corp. v. Lueck, 471 U.S. 202, 213, 220 (1985). In order to assess a club’s health-related duties
to a player – an essential element of a negligence claim – a Court would likely have to refer to and analyze the terms
of the CBA, resulting in the claim’s preemption. See, e.g., Givens v. Tennessee Football, Inc., 684 F.Supp.2d 985
(M.D.Tenn. 2010) (player’s tort claims against club arising out of medical treatment preempted); Williams v. Nat’l
Football League, 582 F.3d 863 (8th Cir. 2009) (players’ tort claims arising out of drug test preempted).
54
Jon R. Johnson, Session 8: Canada and U.S. Approaches to Health Care: How the Canadian and U.S. Political,
Regulatory, and Legal Systems Impact Health Care, 31 Can.-U.S. L.J. 251, 254 (2005).
55
Id. at 257.
56
Id. Under the 1966 Medicare Act, the federal government covered one half of the cost of eligible provincial plans
covering physician services, but the government has since shifted to a “block-funding system” where it pays the
provinces a lump sum for healthcare that covers about 15-20% of the cost of the plans. Id. at 257, 262–63.
57
Id. at 258–59.
58
Id. at 255, 260.
59
Id. at 264. See also Roy Romanow, Directions in Canadian Health Care After the Romanow Report, 67 Sask. L.
Rev. 1, 3 (2004) (“And most doctors [in Canada] are effectively independent contractors paid according to fee
schedules.”); Colleen M. Flood & Bryan Thomas, Canadian Medical Malpractice Law in 2011: Missing the Mark on
Patient Safety, 86 Chi. Kent L. Rev. 1053, 1056–57 (2011) (“In general, the provinces supply publicly funded health
services by contracting with physicians—who are private, for-profit contractors—through provincial medical
associations. The dominant method of payment for these private physicians has been a fee-for-service system,
although this is slowly changing.”); Daniel W. Srsic, Collective Bargaining by Physicians in the United States and
Canada, 15 Comp. Lab. L.J. 89, 9192 (1993) (“In Canada, doctors continue to work almost exclusively in private
practice, while in the United States an increasing number of doctors are working as employees of hospitals and
HMOs.”). Most hospitals, meanwhile, are non-profit and publicly funded, although they are not government owned.
Johnson, supra note 54 at 263. Also, for-profit clinics may contract with a province to provide “insured services” to
patients without violating the Canada Health Act, so long as patients do not have to pay for those services. Id. at 264
n.62.
60
Id. at 264.
61
See, e.g., Lonny Balbi, The Liability of Professional Team Sports Physicians, 22 Alberta L. Rev. 247, 249 (1984);
Wilson v. Vancouver Hockey Club, (1983) 5 D.L.R. 4th 282, para. 7 (Can. B.C.S.C.) (“He explained that the reference
to ‘bill 0113’ was a general practitioner billing code number that would have to be sent to the Medical Services Plan in
order that Dr. Peers would be paid.”); Robitaille, 19 B.C.L.R. at para. 57 (“The doctors rendered accounts to the
medical services association for the account of the player for office consultations and other ‘non-dressing room’
services.”).
62
See Roy Romanow, Directions in Canadian Health Care After the Romanow Report, 67 Saskatchewan L. Rev. 1,
3–4 (2004). Physicians providing these services include, for example, dentists, dental surgeons, ophthalmologists,
psychologists, chiropractors, physiotherapists, osteopaths, and naturopaths. Id.
63
The CBA does not define “retain” or otherwise dictate the requisite scope of involvement by the various doctors.
64
2011 NFL CBA, Art. 39, § 1.
65
2011 NFL CBA, Art. 39, § 1(e).
66
The Concussion Protocol refers to the NFL Head, Neck and Spine Committee‘s Protocols Regarding Diagnosis
and Management of Concussion.

!
228!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
67
NFL Physicians Society Mission Statement, Nat’l Football League Physicians Soc’y, http://nflps.org/about/ (last
visited Aug. 7, 2015), archived at http://perma.cc/928Z-LVZ4.
68
See Dave Siebert, What Is Medical Care Like on an NFL Sideline?, Bleacher Report (Nov. 15, 2013),
http://bleacherreport.com/articles/1850732-what-is-medical-care-like-on-an-nfl-sideline, archived at
http://perma.cc/7JR4-HR3G (quoting then-NFLPS President Matthew Matava describing the “about 177 NFL team
physicians”); Team Physicians, Nat’l Football League Physicians Society, http://nflps.org/team-physicians/ (last
visited Feb. 24, 2016), archived at https://perma.cc/HK8A-QJ9L (listing 153 club doctors as members of the NFLPS).
69
See Frequently Asked Questions - How Often Do All NFLPS Members Meet?, Nat’l Football League Physician’s
Soc’y, http://nflps.org/faqs/how-often-do-all-nflps-members-meet/ (last visited Aug. 7, 2015), archived at
http://perma.cc/76P5-DRQX; Frequently Asked Questions - What Are Typical Topics at Members Meetings?, Nat’l
Football League Physician’s Soc’y, http://nflps.org/faqs/what-are-typical-topics-at-members-meetings/ (last visited
Aug. 7, 2015), archived at http://perma.cc/LR79-9AN3 (“The topics at these meetings vary and address any or all of
the potential injuries that an NFL player may experience. This can include orthopaedic injuries such as ACL tears,
meniscus tears, cartilage injuries to the knee, multiligamentous injuries to the knee, high ankle sprains, fractures,
dislocations, foot injuries, surgical techniques, rehabilitation, hip injuries, arthroscopy of the hip, sports hernia
challenges, shoulder injuries such as dislocations or labral tears, rotator cuff problems, elbow dislocation, biceps or
triceps injuries, wrist injuries, and hand and finger injuries or dislocations. From a medical standpoint, there has been
a recent emphasis on heat-related illnesses, cardiac conditions, MRSA infections, sickle cell traits, concussions and
the management of acute blunt trauma to the chest or abdomen.”).
70
This information was provided by NFLPS.
71
This information was provided by the NFLPS. In Recommendation 2:1-B of our Report Protecting and Promoting
the Health of NFL Players: Legal and Ethical Analysis and Recommendations, we recommend the NFLPS adopt a
code of ethics.
72
2011 NFL CBA, Art. 39, § 2. The CBA’s requirement that athletic trainers be certified by NATA is actually in error
and a requirement with which athletic trainers cannot comply. NATA is a voluntary professional association but does
not certify athletic trainers. Athletic trainers are certified by the Board of Certification for the Athletic Trainer (“BOC”).
Nevertheless, all NFL athletic trainers are certified by the BOC.
73
This information was provided by PFATS.
74
These figures were determined by compiling the data available on the Professional Football Athletic Trainers
Society website. See Member Directory, Prof. Football Athletic Trainers Soc’y, http://www.pfats.com/directory/ (last
visited Aug. 7, 2015), archived at http://perma.cc/PG2S-C2KH.
75
Mission, Prof. Football Athletic Trainers Soc’y, http://www.pfats.com/about/mission (last visited May 31, 2016),
https://perma.cc/SV92-L2FC.
76
History, Prof. Football Athletic Trainers Soc’y, http://www.pfats.com/about/history (last visited Aug. 7, 2015),
archived at http://perma.cc/6P8N-PZTV.
77
Mission, Prof. Football Athletic Trainers Soc’y, supra note 75.
78
See Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations, Ch. 3 (2016).
79
2011 NFL CBA, Art. 39, § 3(e).
80
2011 NFL CBA, Art. 39, § 1(c).
81
For more on this issue, see our Report, Protecting and Promoting the Health of NFL Players: Legal and Ethical
Analysis and Recommendations. A copy of the waiver at issue is included as Appendix L to that Report.
82
This information was provided by the NFLPA.
83
NFL Comments and Corrections (June 24, 2016).
84
2011 NFL CBA, Art. 39, § 1(c).
85
2011 NFL CBA, Art. 40, § 2(a).
86
2011 NFL CBA, Art. 39, § 6.
87
2011 NFL CBA, App. A, § 8.
88
2011 NFL CBA, Art. 42, § 1(a)(iii).
89
2011 NFL CBA, Art. 39, §§ 4–5.
90
2011 NFL CBA, Art. 39, § 4.
91
How does a physician become an NFL team physician? NFL Physicians Soc’y, http://nflps.org/faqs/how-does-a-
physician-become-an-nfl-team-physician/ (last visited Aug. 25, 2015), archived at http://perma.cc/72XA-N2KW.
92
see Synernet Staff Visits NFL Headquarters, Synernet (Feb. 11, 2015), http://www.synernet.net/news/news.aspx,
archived at https://perma.cc/E4UC-WNWP.
93
Telephone Interview with Larry Ferazani, NFL, Vice President, Labor Litigation & Policy (Oct. 6, 2014).
94
In 2001, the Minnesota Vikings paid their three club doctors $4,000, $19,600, and $47,500 per year, respectively.
The amounts varied based on the extent of the doctors’ obligations. See Memorandum and Order, Stringer v. Minn.
Vikings Football Club, No. 02-415, 20–23 (Minn. Dist. Ct. Apr. 25, 2003).
95
NFL Comments and Corrections (June 24, 2016).

!
229!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
96
See Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations, § 3(D) (2016).
97
These waivers are included as Appendices L and M in our Report, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations.
98
Telephone Interview with Larry Ferazani, NFL, Vice President, Labor Litigation & Policy (Oct. 6, 2014).
99
For a complete history of the NFL’s Medical Sponsorship Policy, see Christopher R. Deubert, I. Glenn Cohen, Holly
Fernandez Lynch, Protecting and Promoting the Health of NFL Players: Legal and Ethical Analysis and
Recommendations, § 2(A) (2016).
100
The 2014 Medical Sponsorship Policy defines “Sponsorship Agreements” as “agreements with MSPs involving the
sale or license by the club of commercial assets such as naming rights, stadium signage, advertising inventory within
club-controlled media, promotional inventory (e.g., day-of-game promotions), hospitality, and rights to use club
trademarks for marketing and promotional purposes.”
101
According to the Policy, MSPs include “hospitals, universities, medical practice groups, rehabilitation facilities,
laboratories, imaging centers and other entities that provide medical care and related services.” Although doctors are
not specifically included in the definition of MSPs, the NFL includes doctors as MSPs for purposes of the Policy.
Email with Larry Ferazani, Vice President, Labor Litigation & Policy, Nat’l Football League (Apr. 15, 2015) (on file with
author).
102
Id.
103
Id.
104
Bill Pennington, Sports Turnaround: The Team Doctors Now Pay the Team, The New York Times, May 18, 2004,
http://www.nytimes.com/2004/05/18/sports/sports-medicine-sports-turnaround-the-team-doctors-now-pay-the-
team.html?pagewanted=1, archived at https://perma.cc/BDU2-ETSM.
105
See Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations, § 2(A) (2016).
106
NFL Comments and Corrections (June 24, 2016).
107
In a written response to our Report, the NFL again disagreed with us, stating: “Despite the clear language in the
policy prohibiting the exchange of medical services for sponsorship, the initial draft of the Report asserted,
‘[a]dditionally the Medical Sponsorship Policy does not prohibit medical service providers from paying for the right to
provide medical services to players.’ The NFL identified this inaccurate statement, and advised the authors that,
‘[t]he Policy on Medical Services Agreements and Sponsorships does [prohibit a physician from paying for the right to
provide medical care to NFL Players].’ Incredibly, the Report rejected the NFL’s interpretation of the language in its
own policy, which we enforce, by asserting the interpretation of the language was unclear to the authors, and as
result refused to remove this reference from the Report. The Report cites no example where the policy has not been
followed.” For the reasons stated above, we continue to disagree with the NFL’s interpretation and recommend that it
be clarified.
108
In reviewing our Report Protecting and Promoting the Health of NFL Players: Legal and Ethical Analysis and
Recommendations, the National Athletic Trainers Association stated that “[p]hysician practices paying Clubs to serve
as team physicians may result in significant conflicts of interest (COI) in the care of the NFL athlete. Health care
should be based on best practices.”
109
!Memorandum!from!Dan!Halem!to!All!Major!League!Clubs!(Dec.!1,!2015).!
110
!Id.(
111
Memorandum from Dan Halem to MLB General Managers and Medical Personnel (Nov. 7, 2012).
112
Id.
113
!Memorandum!from!Dan!Halem!to!All!Major!League!Clubs!(Dec.!1,!2015).!
114
!See(2012!MLB!CBA,!Art. XIII, Attachments 5, 6, 18, 35 and 36, and Schedule A.!
115
2011 NFL CBA, Art. 39, § 1.
116
Home, Major League Baseball Team Physicians Ass’n, http://mlbtpa.org/ (last visited Aug. 25, 2015), archived at
http://perma.cc/2JTM-XMJ5.
117
!!MLBPA, MLB Announce Details of New Labor Agreement, MLBPA (Dec. 2, 2016),
http://www.mlbplayers.com/ViewArticle.dbml?DB_OEM_ID=34000&ATCLID=211336390, archived at
https://perma.cc/4XUA-2DAW (announcing replacement of 15-day DL with 10-day DL).!
118
!Id.!
119
2012 MLB CBA, Art. XIII, § E.
120
The MLB CBA’s requirement that athletic trainers be certified by NATA or CATA is actually in error and a
requirement with which athletic trainers cannot comply. NATA and CATA are voluntary professional associations but
do not certify athletic trainers. Athletic trainers are certified by the Board of Certification for the Athletic Trainer
(“BOC”). The NFL CBA also erroneously requires athletic trainers to be certified by NATA.
121
About, Professional Baseball Athletic Trainers Soc’y, http://pbats.com/about/ (last visited Aug. 25, 2015), archived
at http://perma.cc/G9FP-42CS.

!
230!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
122
In reviewing a draft of this Report a second time, MLB stated that “MLB maintains our position regarding a code of
ethics, and do not find it appropriate to ask physicians to comply with a code of ethics that differs from the Hippocratic
Oath or other professional/ethical oaths they took as a physician.” To be clear, we do not recommend the addition of
codes of ethics that differ from or conflict with existing codes. Instead, we believe it is appropriate that additional
codes of ethics tailored for the specific circumstances of professional sports supplement existing codes. For more
discussion on the challenges of the sports healthcare environment, see our Special Report, NFL Player Health: The
Role of Club Doctors, 46 HASTINGS CENTER REP. 2 (2016).
123
In addition to those obligations listed here, club doctors are also involved in determining whether a player’s injury
will prevent him from playing in the All-Star Game. 2012 MLB CBA, Art. XV, § O.
124
2012 MLB CBA, Art. XIII, § G.
125
See AMA Code Opinion 3.1.5 – Professionalism in Relationships with Media: To safeguard patient interests when
working with representatives of the media, all physicians should: (a) Obtain consent from the patient or the patient’s
authorized representative before releasing information; (b) Release only information specifically authorized by the
patient or patient’s representative or that is part of the public record; (c) Ensure that no statement regarding diagnosis
or prognosis is made except by or on behalf of the attending physician; and, (d) Refer any questions regarding
criminal activities or other police matters to the proper authorities. Opinion 3.1.5 – Professionalism in Relationships
with Media, Am. Med. Ass’n, available at http://www.ama-assn.org/ama/pub/physician-resources/medical-
ethics/code-medical-ethics.page (last visited Aug. 1, 2016), archived at https://perma.cc/ZR8K-FC93.
126
2012 MLB CBA, Art. XIII, § G(6).
127
2012 MLB CBA, Art. XIII, § G(7)(a).
128
2012 MLB CBA, Art. XIII, § I.
129
2012 MLB CBA, Art. XIII, § C.
130
2012 MLB CBA, Attachment 36.
131
Id.
132
! In our Report Protecting and Promoting the Health of NFL Players: Legal and Ethical Analysis and
Recommendations we set forth a comprehensive recommendation to address this issue. We propose restructuring
NFL club medical staff in such a way that the doctor treating the players has as his or her only concern the well-being
of the player-patient and has no advisory role to the club.!
133
Id.
134
Id. at Concussion Return to Play Form.
135
Memorandum from Dan Halem to MLB General Managers and Medical Personnel (Nov. 7, 2012).
136
MLB Uniform Player Contract, at REGULATIONS ¶ 2.
137
2012 MLB CBA, Art. XIII, § D.
138
2012 MLB CBA, Art. XIII, § D.
139
2012 MLB CBA, Art. XIII, § G.
140
Id.
141
Id.
142
Email from Jon Coyles, MLB Labor Counsel, to Chris Deubert (Oct. 6, 2014, 15:13 EST) (on file with author).
143
Id. MLB is not aware of any field managers that have the authority to hire or terminate medical personnel. Id.
144
Id.
145
Bill King, Team Doctors Rattled by Threat of Malpractice Suits, SportsBusinessDaily.com (June 21, 2004),
http://www.sportsbusinessdaily.com/Journal/Issues/2004/06/20040621/SBJ-In-Depth/Team-Doctors-Rattled-By-
Threat-Of-Malpractice-Suits.aspx, archived at http://perma.cc/5E7V-QMXX; See generally Dennis Durao, An
Endangered Species: Professional Sports Team Physicians, 15 Quinnipiac Health L.J. 33 (2011) (detailing increases
in insurance premiums for physicians treating professional athletes).
146
Email from Jon Coyles, supra note 142.
147
2012 MLB CBA, Attachment 35.
148
2012 MLB CBA, Attachment 18 at ¶¶ 2–3.
149
Id. at ¶ 8.
150
MLB Uniform Player Contract, ¶ 6(b)(1), included as Schedule A to the 2012 MLB CBA.
151
Id. at ¶ 6(b)(2). The receiving club must return all of the records within 30 days. Id.
152
Tom Haudricourt, Milwaukee Journal Sentinel Tom Haudricourt column, Milwaukee J. Sentinel, Apr. 6, 2008,
available at 2008 WLNR 6507711; Alyson Footer, Clearing up the term ‘athletic trainer’, MLB News, Mar. 25, 2008,
http://m.mlb.com/news/article/2444052/, archived at http://perma.cc/S2CD-RXDE; see also
Alison Gardiner-Shires, Scott C.Marley, John C. Barnes, Mark E. Shires, Professional baseball athletic trainers’
perceptions of preparation for job-specific duties, 47 J. of Athletic Training 704 (2012).
153
Tim Johnson and Dr. Eric Berkson, Life As a Red Sox Team Physician, Mass. Gen. Hospital (Apr. 13, 2010),
http://www.massgeneral.org/about/newsarticle.aspx?id=2165, archived at http://perma.cc/DAG9-X9AZ.
154
Id.
155
Memorandum from Dan Halem to MLB General Managers and Medical Personnel (Nov. 7, 2012).

!
231!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
156
Memorandum from MLB Commissioner Selig to All Major League Owners, President and General Managers re:
Medical Service Provider Sponsorships (Nov. 17, 2004) (on file with author). Before this policy, some sponsorship
arrangements involved payments from the sponsoring provider to the club, coupled with agreements to provide free
healthcare to players and their families in exchange for advertising space in the club’s stadium. Healthy: Rangers Ink
Deal With Medical Center of Arlington, SportsBusinessDaily.com (Feb. 25, 2004),
http://www.sportsbusinessdaily.com/Daily/Issues/2004/02/Issue-108/Sponsorships-Advertising-Marketing/Healthy-
Rangers-Ink-Deal-With-Medical-Center-Of-Arlington.aspx, archived at http://perma.cc/3MQK-4DKP.
157
Memorandum from Daniel R. Halem to All Major League Club Presidents, General Managers, Assistant General
Managers, Club Counsel, Team Physicians and Certified Athletic Trainers re: Medical Service Provider Sponsorships
(Feb. 18, 2014) (on file with author).
158
Email from Jon Coyles, MLB Labor Counsel, to Chris Deubert (Oct. 6, 2014, 15:13 EST) (on file with author).
159
Id.
160
Memorandum from Daniel R. Halem to All Major League Club Presidents, General Managers, Assistant General
Managers, Club Counsel, Team Physicians, and Certified Athletic Trainers re: Medical Service Provider
Sponsorships (Feb. 18, 2014) (on file with author).
161
See, e.g., Oliver Millerchip, Kaiser Permanente Backs MLB’s Nationals, SportsProMedia.com (May 7, 2014),
http://www.sportspromedia.com/news/kaiser_permanente_backs_mlbs_nationals, archived at http://perma.cc/XMQ3-
TG2X (noting a managed care consortium’s sponsorship of the Washington Nationals); Pirates Announce Affiliation
Renewals With Team Partners, MLB.com (May 6, 2013, 9:23 am), http://m.mlb.com/news/article/46753608/pirates-
announce-affiliation-renewals-with-team-partners, archived at https://perma.cc/U358-X9KR (noting a multiyear
agreement for Highmark to be the “Official Healthcare Provider of the Pittsburgh Pirates”).
162
2017 NBA CBA, Art. XXII, § 1(a).
163
2017 NBA CBA, Art. XXII, § 6.
164
The NBAPA’s website is password-protected and thus additional information is not available.
165
2017 NBA CBA, Art. XXII, § 3.
166
The NBA CBA’s requirement that athletic trainers be certified by NATA or CATA is actually in error and a
requirement with which athletic trainers cannot comply. NATA and CATA are voluntary professional associations but
do not certify athletic trainers. Athletic trainers are certified by the Board of Certification for the Athletic Trainer
(“BOC”). The NFL CBA also erroneously requires athletic trainers to be certified by NATA.
167
2017 NBA CBA, Art. XXII, § 1(b).
168
About, Nat’l Basketball Athletic Trainers Ass’n, http://nbata.com/about-us/ (last visited Aug. 25, 2015), archived at
https://perma.cc/AT3Z-N7TT.
169
Id.
170
See Travis Tate, A Day in the Life of - Athletic Trainer, NBA.com,
http://www.nba.com/jazz/news/day_in_the_life_athletic_trainer.html (last visited Aug. 25, 2015), archived at
http://perma.cc/V7CV-SFVW (describing duties of Utah Jazz athletic trainer); Jaimie Siegle, Behind the Scenes at
Philips Arena with NBA Head AT Wally Blase, Nat’l Athletic Trainers Ass’n (May 22, 2014), http://www.nata.org/nata-
news-blog/behind-scenes-philips-arena-nba-head-wally-blase, archived at http://perma.cc/BBF2-TE4G (describing
duties of Atlanta Hawks athletic trainer); Fred Kerber, Train of Thought – Walsh Keeps Nets in Working Order, N.Y.
Post, Nov. 15, 2008, available at 2008 WLNR 21933024 (describing duties of New Jersey Nets athletic trainer).
171
In reviewing a draft of this Report, the NBA stated “[t]here are other terms governing obligations of medical
personnel, including additional provisions regarding furnishing relevant information, not making public certain medical
information, conducting certain health screenings, etc.” Information concerning confidential player health information
is discussed below. Otherwise, while other provisions of the CBA reference club doctors, they do not necessarily
create obligations for them and thus we do not discuss them here.
172
2017 NBA CBA, Art. XXII, § 2.
173
2017 NBA CBA, Art. XXII, § 4(f).
174
2011 NFL CBA, Art. 40, § 2(a).
175
2017 NBA CBA, Art. XXII, § 11(c).
176
2017 NBA CBA, Art. XXII, § 11(b).
177
2017 NBA CBA, Art. XXII, § 11(a).
178
The creation of a committee of medical experts with members selected by the league, the union, and the members
of the committee matches the composition of the Medical Committee we proposed for the NFL in our report,
Protecting and Promoting the Health of NFL Players: Legal and Ethical Analysis and Recommendations. We
proposed a neutral Medical Committee be responsible for the hiring, compensation levels, review and possible
termination of doctors treating NFL players as part of a process to remove the structural conflict of interest inherent in
having doctors that both treat players and provide services to the club. Additional details and explanation can be
found in our report.
179
2017 NBA CBA, Art. XXII, § 11(d)(2).
180
2017 NBA CBA, Art. XXII, § 11(d)(3).
181
2017 NBA CBA, Art. XXII, § 11(d)(3).

!
232!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
182
2017 NBA CBA, Art. XXII, § 11(g).
183
Id. The contract amendment possibility existed in CBAs prior to 2017 and thus is not limited to the Fitness-to-Play
determinations. When a club doctor believes a player is not sufficiently fit to play (which would include general fitness
as well as medical determinations), a player’s contract can be amended to provide that the club can suspend the
player for successive one-week periods until the club believes the player can play. See id.; 2017 NBA CBA, Art. II, §
3(l); NBA Uniform Player Contract, Ex. 7. After each one-week suspension, the player has the right to be examined
by a doctor selected by the President or a Vice President of the American Society of Orthopedic Surgeons (the
“Reviewing Physician”). NBA Uniform Player Contract, Ex. 7. The Reviewing Physician’s determination “concerning
the physical condition of the Player to play skilled basketball” is binding on the club and the player. Id. If the
Reviewing Physician determines that the player “is in physical condition sufficient to play skilled basketball,” then the
club can no longer suspend the player. Id. At this point, as a practical matter, the player would be allowed to suit up
and presumably practice, but the club would still have the discretion not to play the player. Nevertheless, if the club is
unwilling to play the player, the player is of no value to the club. Consequently, the club would likely play the player,
trade him to another club, or release him. According to the NBA, this provision generally concerns players’ physical
fitness at the beginning of each season. Nevertheless, it has the potential to be applied to the Fitness-to-Play
determinations as well.
184
Chris Bosh fails Heat physical with blood clotting, no timetable for return, Sports Illustrated (Sep. 23, 2016),
http://www.si.com/nba/2016/09/23/chris-bosh-miami-heat-blood-clotting, archived at https://perma.cc/25X4-UYU3.
185
Id.
186
Howard Beck, Stuck in Standoff Over Chris Bosh’s Future, NBA to Create New Medical Panels, Bleacher Rep.
(Dec. 21, 2016), http://bleacherreport.com/articles/2683133-stuck-in-standoff-over-chris-bosh-future-nba-to-create-
new-medical-panels?utm_source=facebook.com&utm_medium=share&utm_campaign=web-des-art-top-188,
archived at https://perma.cc/GB52-PBHY.
187
Id.
188
2017 NBA CBA, Art. XXII, § 10(b).
189
2017 NBA CBA, Art. XXII, § 10(c).
190
2017 NBA CBA, Art. XXII, § 10(g).
191
NBA Uniform Player Contract, § 7(a).
192
NBA Uniform Player Contract, § 7(d).
193
NBA Uniform Player Contract, § 7(e).
194
NBA Uniform Player Contract, § 7(f).
195
2017 NBA CBA, Art. XXII, § 7.
196
NBA Uniform Player Contract, § 7(f).
197
NBA Uniform Player Contract, § 7(g).
198
2017 NBA CBA, Art. II, § 13(i).
199
NBA Uniform Player Contract, § 7(h)(i).
200
NBA Uniform Player Contract, § 7(h)(ii).
201
“This notice requirement [does] not apply to workouts or training that exclusively involve jogging, road bicycling,
swimming, yoga, Pilates and/or dance.” NBA Uniform Player Contract, § 7(h)(ii).
202
NBA Uniform Player Contract, § 7(i).
203
Email from David Weiss, Associate Vice President and Assistant General Counsel, NBA, to author (Sept. 30,
2014).
204
2017 NBA CBA, Art. XXII, § 4(a). However, a “player or his immediate family (where appropriate) shall have the
right to approve the terms and timing of any public release of medical information relating to any injuries or illnesses
suffered by that player that are potentially life- or career-threatening, or that do not arise from the player’s
participation in NBA games or practices.” 2017 NBA CBA, Art. XXII, § 4(e).
205
A club is then permitted to “make public information relating to the players in its employ, provided that such
information relates solely to the reasons why any such player has not been or is not rendering services as a player.”
2017 NBA CBA, Art. XXII, § 4(d). In the NFL, players similarly sign waivers permitting the public disclosure of such
information.
206
2017 NBA CBA, Art. XXII, § 4(b).
207
2017 NBA CBA, Art. XXII, § 6.
208
See, e.g., Sacramento Kings Announce Kaiser Permanente as Team’s New Medical Provider, Nat’l Basketball
Ass’n, Oct. 3, 2013, http://www.nba.com/kings/news/sacramento-kings-announce-kaiser-permanente-teams-new-
medical-provider, archived at http://perma.cc/FB55-RK6F; DMC Sports Medicine – New Home, Detroit Med. Center,
http://www.dmc.org/detroit-medical-center-sports-medicine-new-home.html (last visited Aug. 25, 2015), archived at
http://perma.cc/DEU3-G74H.
209
2013 NHL CBA, § 34.2(a).
210
20113 NHL CBA, § 34.2(a). Similarly, when the 2011 NFL CBA added a requirement that all club doctors have a
Certificate of Added Qualification in Sports Medicine, the existing club doctors were not required to obtain the
Certificate.

!
233!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
211
For the reasons described in the Introduction, Section E: Goals and Process, we did not seek to survey NHL
medical club personnel. Nevertheless, in response to our report, Protecting and Promoting the Health of NFL Players:
Legal and Ethical Analysis and Recommendations, one NHL club athletic trainer reached out to us and provided us
information via email and telephone. At the athletic trainer’s request, we do not identify him or the club for which he
works. It is important to recognize that the opinions of the athletic trainer are only that of one individual and cannot be
considered representative of the viewpoints of all NHL club athletic trainers or medical staff. Nevertheless, we believe
the athletic trainer’s personal experiences are informative and thus include them here.
212
The NHL’s concussion protocol does not require the use of an independent neurologist. In contrast, the NFL’s
concussion protocol requires that, during games, any player suspected of having suffered a concussion be examined
by an unaffiliated neurotrauma consultant. The difference in policies might result at least in part for practical reasons.
There are 256 regular season NFL games versus 1,312 regular season NHL games.
213
2013 NHL CBA, § 34.2(b)(i).
214
Mission Statement, Prof. Hockey Athletic Trainers Soc’y, http://www.phats-sphem.com/mission (last visited Aug.
26, 2015), archived at http://perma.cc/74ZD-J2Z7.
215
See FrankD, An interview with Tampa Bay Lightning Head Athletic Trainer Tommy Mulligan, SB Nation (Feb. 9,
2010, 6:00 AM), http://fromtherink.sbnprivate.com/2010/2/9/1299657/an-interview-with-tampa-bay archived at
http://perma.cc/BRC2-6A86 (discussing duties of Tampa Bay Lightning athletic trainer).
216
2013 NHL CBA, § 34.1(a).
217
2013 NHL CBA, § 34.1(b).
218
The NHL club athletic trainer who contacted us believes the club for which he works treats players “poorly.” The
athletic trainer believes there is an “inherent conflict of interest” where club doctors treat players while also reporting
to the club. As a result, the athletic trainer believes club doctors often place the interests of the club ahead of those of
the player. Although the athletic trainer believes there is “widespread” agreement in the NHL medical community
about these problems, we remind the reader that the opinions of this particular athletic trainer should not be
considered representative of all NHL club athletic trainers.
219
2013 NHL CBA, § 34.3(b)(ii).
220
2013 NHL CBA, § 34.8.
221
Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations, § 2(I) (2016).
222
2013 NHL CBA, § 34.4(a).
223
The athletic trainer who contacted us expressed his belief that this process does not adequately protect player
health. As an initial matter, the athletic trainer believes club doctors often try to dissuade players from receiving a
second medical opinion, including by telling players that the club doctor has already consulted with other club
doctors. Second, the athletic trainer expressed his belief that many of the second opinion consultations are with
doctors from other clubs, who are unlikely to render an opinion that disagrees with the initial club doctor’s opinion.
224
Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations, § 4(D) (2016).
225
2013 NHL CBA, § 23.10.
226
Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations, § 3(A) (2016).
227
NHL players are also entitled a second medical opinion where a club doctor has determined the player is
physically unable to perform his duties as a hockey player. 2013 NHL CBA, § 17.7. The player is responsible for the
costs of this consultation. If no consensus is reached between the club doctor and the player’s second opinion doctor
in the fitness for play context, a third physician chosen by them decides the matter. Id. The club and player share the
costs for the third physician’s opinion. Id.
228
2013 NHL CBA, § 34.4(c)(i).
229
2013 NHL CBA, § 34.4(c)(ii).
230
2013 NHL CBA, § 34.4(c)(iii).
231
2013 NHL CBA, § 34.4(d).
232
2013 NHL CBA, § 34.4(e).
233
2013 NHL CBA, § 34.5(a).
234
Standard Player Contract, § 2, included as Exhibit 1 to the 2013 NHL CBA.
235
If there is a question as to whether the player is disabled or unable to perform his duties, the Standard Player
Contract sets forth a process by which that determination is made by an independent doctor. See Standard Player
Contract, § 5, included as Exhibit 1 to the 2013 NHL CBA. If the player is found to be physically able to play and
refuses to do so, he can be immediately suspended without pay. Id. at § 5(j).
236
2013 NHL CBA, § 34.5(a).
237
2013 NHL CBA, § 34.5(b).
238
2013 NHL CBA, § 34.6.
239
2013 NHL CBA, § 34.6(d).

!
234!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
240
In a pair of cases from the early 1980s, Canadian courts were split about whether club doctors are employees or
independent contractors. See Robitaille v. Vancouver Hockey Club, Ltd., (1981) 124 D.L.R. 3d 228 (Can. B.C.C.A.),
available at https://www.canlii.org/en/bc/bcca/doc/1981/1981canlii532/1981canlii532.html, archived at
https://perma.cc/Q4N9-HGP4 (finding that the three club doctors were employees of the defendant club and holding
the club vicariously liable); Wilson v. Vancouver Hockey Club, (1983) 5 D.L.R. 4th 282 (Can. B.C.S.C.), available at
https://www.canlii.org/en/bc/bcsc/doc/1983/1983canlii340/1983canlii340.html, archived at https://perma.cc/JNG5-
X593 (finding that the club doctor was an independent contractor and the defendant club was not vicariously liable for
his negligence). See also Martin v. Casagrande, 559 N.Y.S.2d 68, 69 (N.Y.App.Div. 1990) (NHL player’s recovery
under workers’ compensation laws barred player’s lawsuit against club and club doctor); Frank Fitzpatrick, Jury Starts
Deliberations in Babych’s Lawsuit, Philly.com (Oct. 31, 2002), http://articles.philly.com/2002-10-
31/sports/25352880_1_dave-babych-flyers-physician-deliberations, archived at http://perma.cc/5TE5-7TUU; Dave
Babych Wins Injury Lawsuit, CBCSports (Nov. 1, 2002, 1:31 a.m.), http://www.cbc.ca/sports/hockey/dave-babych-
wins-injury-lawsuit-1.304723, archived at http://perma.cc/C29K-ZK5T (former player awarded $1.37 million in
damages against club doctor for alleged improper treatment of broken foot after court determined that club doctor
was an independent contractor).
241
2013 NHL CBA, § 34.3(a).
242
“‘Club Personnel’ means a Club’s coaching staff, owners, presidents, executives, hockey operations staff, general
managers, assistant general managers, human resources personnel, and Club Health Professionals.” 2013 NHL
CBA, Art. 1.
243
2013 NHL CBA, 34.3(c)(x).
244
2013 NHL CBA, § 34.3(c).
245
Sean Gordon & David Shoalts, Diagnosing Sports Injuries Never an Exact Science, Globe & Mail, Feb. 7, 2012,
http://www.theglobeandmail.com/sports/hockey/diagnosing-sports-injuries-never-an-exact-science/article544490/,
archived at http://perma.cc/N26D-Q7WL. NHL spokespersons have been cagey about the number of teams with such
deals in the past. See Tom Farrey, A Snapshot of Sports’ Medical Dilemma, ESPN, Sept. 12, 2002,
http://espn.go.com/gen/s/2002/0912/1430969.html, archived at http://perma.cc/N26D-Q7WL (“Spokespersons for the
NHL and Major League Baseball say they don’t know how many of their teams have such deals.”).
246
Gordon & Shoalts, supra note 245. Accepting payment from medical groups is “frowned upon” in Canada. Id.
247
See Bill King, Team Doctors Rattled by Threat of Malpractice Suits, SportsBusinessDaily.com (June 21, 2004),
http://www.sportsbusinessdaily.com/Journal/Issues/2004/06/20040621/SBJ-In-Depth/Team-Doctors-Rattled-By-
Threat-Of-Malpractice-Suits.aspx, archived at http://perma.cc/5E7V-QMXX.
248
2014 CFL CBA, § 34.18.
249
See Administration, Edmonton Eskimos, http://www.esks.com/page/administration (last visited Aug. 26, 2016),
archived at https://perma.cc/6JNY-Y6U8 (listing nine doctors affiliated with Edmonton); Football Op, Montreal
Alouettes, http://en.montrealalouettes.com/football-operations/ (last visited Aug. 26, 2016), archived at
https://perma.cc/DC3G-LMAJ (listing nine doctors affiliated with Montreal Alouettes); Front Office & Football
Operations, Toronto Argonauts, http://www.argonauts.ca/coaching-staff-football-operations/ (last visited Aug. 22,
2016), archived at https://perma.cc/P3C8-HDT7 (listing seven doctors affiliated with Toronto Argonauts).
250
Id.
251
Id.
252
2014 CFL CBA, § 34.03.
253
CFL Standard Player Contract, ¶ 6.
254
2011 NFL CBA, App. A, § 8.
255
Telephone interview by Chris Deubert with Michael Copeland, President and Chief Operating Officer, CFL (July
24, 2014).
256
See Robitaille v. Vancouver Hockey Club, Ltd., (1981) 124 D.L.R. 3d 228 (Can. B.C.C.A.), available at
https://www.canlii.org/en/bc/bcca/doc/1981/1981canlii532/1981canlii532.html, archived at https://perma.cc/Q4N9-
HGP4 (finding that the three club doctors were employees of the defendant club and holding the club vicariously
liable); Wilson v. Vancouver Hockey Club, (1983) 5 D.L.R. 4th 282 (Can. B.C.S.C.), available at
https://www.canlii.org/en/bc/bcsc/doc/1983/1983canlii340/1983canlii340.html, archived at https://perma.cc/JNG5-
X593 (finding that the club doctor was an independent contractor and the defendant club was not vicariously liable for
his negligence).
257
2014 CFL CBA, § 24.09.
258
2014 CFL CBA, § 24.08.
259
Dr. Robert McDougall and the Saskatchewan Roughriders, 17 J. Can. Rheumatology Ass’n (2007),
http://www.stacommunications.com/customcomm/Back-issue_pages/CRAJ/crajPDFs/2007/fall2007/english/04.pdf,
archived at http://perma.cc/VAP5-8P59.
260
An Athlete’s Perspective: An Interview with CFL All-star Chris Walby, 17 J. Can. Rheumatology Ass’n (2007),
http://www.stacommunications.com/customcomm/Back-issue_pages/CRAJ/crajPDFs/2007/fall2007/english/04.pdf,
archived at http://perma.cc/VAP5-8P59.
261
Id.

!
235!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
262
Telephone interview by Chris Deubert with Michael Copeland, President and Chief Operating Officer, Can.
Football League (July 24, 2014).
263
Sean Gordon and David Shoalts, Diagnosing Sports Injuries Never an Exact Science, Globe & Mail, Feb. 7, 2012,
http://www.theglobeandmail.com/sports/hockey/diagnosing-sports-injuries-never-an-exact-science/article544490/,
archived at http://perma.cc/N26D-Q7WL.
264
The MLS Medical Manual states that “Club Physicians and Athletic Trainers are required to comply with the
policies and procedures set forth in this manual.” MLS Medical Policies & Procedures Manual § I (2015).
265
MLS Medical Policies & Procedures Manual § III.5 (2015).
266
2015 MLS CBA, § 9.8.
267
MLS Medical Policies & Procedures Manual Introduction (2015).
268
Home, MLS Team Physician Soc’y, http://www.mlsteamdocs.com/ (last visited Aug. 26, 2015), archived at
http://perma.cc/QJ7E-82SN.
269
About, Prof. Soccer Athletic Trainers’ Soc’y, http://www.psats.net/#!psats-members-/cigi (last visited Aug. 26,
2015), archived at http://perma.cc/D22U-5SP7.
270
MLS Medical Policies & Procedures Manual § V.2 (2015).
271
Interview with MaryBeth Horodyski, Vice President, NATA, and Jim Thornton, President, NATA (Aug. 20, 2014).
272
See BOC Vision & Mission, Board of Cert. for Athletic Trainers, http://bocatc.org/about-us/boc-vision-mission (last
visited Aug. 7, 2015), archived at http://perma.cc/3J98-WU2T.
273
See An In Depth Look with an Athletic Trainer in Major League Soccer, Board of Cert. for the Athletic Trainer,
http://www.bocatc.org/blog/uncategorized/an-in-depth-look-with-an-athletic-trainer-in-major-league-soccer/ (last
visited Aug. 26, 2015), archived at http://perma.cc/W86J-FAHW (interview with Houston Dynamo athletic trainer
describing his duties); Luke Lohr, Plight of the MLS Athletic Trainer, The MLS Reserves, Apr. 4, 2012,
www.mlsreserves.com/2012/04/plight-of-mls-athletic-trainer.html, archived at http://perma.cc/PZ6S-Z89R (interview
with FC Dallas athletic trainer describing his duties).
274
Id.
275
Id.
276
2015 MLS CBA, § 9.7.
277
Id.
278
MLS Medical Policies & Procedures Manual § I (2015). See also id. § IV.5 (“Club Physicians will always provide
medical services based on their best medical judgment.”); id. § X.A (“Club Physicians and Athletic Trainers will at all
times comply with the highest standard of care when treating any injury or other medical problem.”)
279
2015 MLS CBA, § 9.1(v).
280
MLS Standard Player Agreement, ¶ 7(g).
281
2011 NFL CBA, App. A, ¶ 8.
282
MLS Standard Player Agreement, ¶ 4(b).
283
2011 NFL CBA, App. A, ¶ 8.
284
2015 MLS CBA, § 9.5.
285
2015 MLS CBA, § 9.1(i).
286
2015 MLS CBA, § 9.1(iii).
287
2015 MLS CBA, § 9.1(iv).
288
2015 MLS CBA, § 9.3(i)(a).
289
2015 MLS CBA, § 9.3(i).
290
2015 MLS CBA, § 9.4.
291
Id.
292
NFL Player Contract, § 8, included as Appendix A to the 2011 NFL CBA.
293
MLS Medical Policies & Procedures Manual § III.1, § V.2 (2015).
294
MLS Medical Policies & Procedures Manual § V.3 (2015).
295
Email from Bob Foose, Executive Director, MLS Players Union, to author (Aug. 29, 2014).
296
See Docket, D.C. Soccer LLC, et al. v. Commonwealth Orthopaedics & Rehabilitation, P.C., et al., 2012-CA-
007050 (D.C. Sup. Ct.), available by searching the District of Columbia courts website at
https://www.dccourts.gov/cco/maincase.jsf.
297
See Complaint, Namoff v. D.C. Soccer LLC (D.C. Sup. Ct. Aug. 29, 2012).
298
Order, Namoff v. D.C. Soccer LLC, No. 2012-CA-7050 (D.C. Sup. Ct. May 8, 2014); Steven Goff, Namoff’s lawsuit
was dismissed, Wash. Post, Jan 14, 2015, https://www.washingtonpost.com/news/soccer-
insider/wp/2015/01/14/namoffs-lawsuit-was-dismissed//, archived at https://perma.cc/5JEK-EZCE.
299
Order, Namoff v. D.C. Soccer LLC, No. 2012-CA-7050, *2 (D.C. Sup. Ct. May 8, 2014).
300
Id. at 8.
301
See Order, Namoff v. Annunziata, No. 2012-CA-008981 (D.C. Sup. Ct. Aug. 12, 2014).
302
Id. at 7.
303
Id. at 9.
304
Id. at 6.

!
236!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
305
Id.
306
The authorization’s breadth stands in contrast to the MLS Medical Manual’s multiple provisions requiring that
“[c]onfidentiality regarding a Player’s medical condition will be maintained at all times.” MLS Medical Policies &
Procedures Manual § I (2015). See also id. § IV.4; id. § IX.A.1.
307
2015 MLS CBA, Ex. 2.
308
New York Red Bulls and Hospital for Special Surgery Announce Partnership, Hospital for Special Surgery (Mar.
21, 2007), http://www.hss.edu/newsroom_hss-partnership-new-york-red-bulls-soccer-team-sports-medicine.asp,
archived at http://perma.cc/UR8C-JAFC.
309
See Technical Staff, N.Y. Red Bulls, http://www.newyorkredbulls.com/technicalstaff (last visited Aug. 26, 2015),
archived at http://perma.cc/88X2-LF4A.
310
Orlando City SC and Orlando Health Unveil Inaugural MLS Home Jersey, Orlando City Soccer Club (Nov. 5,
2014), available at http://www.orlandocitysc.com/post/2014/11/05/orlando-city-sc-and-orlando-health-unveil-
inaugural-mls-home-jersey, archived at http://perma.cc/RL3N-6VJY.
311
See Daryl Christopher Oshbar, Orlando Health, http://www.orlandohealth.com/physician-finder/daryl-christopher-
osbahr-md?hcmacid=a0bi000000HyCQ3AAN (last visited Aug. 22, 2016), archived at https://perma.cc/66C5-6U7X.
312
MLS Medical Policies & Procedures Manual § X.B.2.d (2015).
313
As discussed above, when asked specifically about this issue, MLB directed us to its minimum game day
standards and the MLBTPA mission statement, both of which were discussed above. However, neither the game day
standards nor the mission statement sets forth a standard of care for club doctors specific to MLB club doctors or that
goes beyond what is already required by codes of ethics and relevant law applicable to all doctors. By comparison,
the NFL, NHL and MLS CBAs all set forth standards of care for their club doctors which, in particular, attempt to
address the conflict of interest inherent in having doctors that treat players while also providing services to the club.
314
In reviewing a draft of this Report, MLB stated that our indication that MLB players do not have the right to the
surgeon of their choice was “inaccurate.” We disagree. As discussed above, while MLB clubs are directed to “take a
Player’s reasonable preferences into account when designating doctors to perform surgery,” “the Club has the right to
designate the doctors and hospitals when a Player is undergoing a surgery for an employment related injury[.]” 2012
MLB CBA, Attachment 35. In addition, “in no event should they force a Player to have a surgery performed by the
Club physician but should instead, in any case in which a Player has objected to the surgery being performed by the
Club physician, designate another physician to perform the surgery.” Id. Thus, the decision of which surgeon to use
ultimately rests with the club, subject to player’s ability to object to the club doctor performing the surgery.
315
2013 NHL CBA, § 34.5(a).
316
2013 NHL CBA, § 34.4(f).
317
2011 NFL CBA, Art. 40, § 2(a).
318
2014 CFL CBA, § 24.08.
319
Id.
320
Under the CFL Standard Player Contract, clubs are obligated to pay an injured player’s medical expenses and
salary (provided the player is a veteran) for so long as the player is physically unable to play. CFL Standard Player
Contract ¶¶ 20-21. An Injury Grievance would be filed if the player and club disputed the extent of the player’s
injuries, and thus the club’s obligations to pay the player’s salary and medical expenses.
321
In our report Protecting and Promoting the Health of NFL Players: Legal and Ethical Analysis and
Recommendations, Chapter 3: Club Doctors, we describe in depth doctors legal and ethical obligations in the two
different situations: providing medical care; and, performing fitness-for-play evaluations.
322
See Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations, § 2(H) (2016).
323
2011 NFL CBA, Art. 45, § 2.
324
An Injury Grievance is “a claim or complaint that, at the time a player’s NFL Player Contract or Practice Squad
Player Contract was terminated by a Club, the player was physically unable to perform the services required of him
by that contract because of an injury incurred in the performance of his services under that contract.” 2011 NFL CBA,
Art. 45, § 1.
325
See Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations, Recommendation 1:1-F (2016).
326
In our Report Protecting and Promoting the Health of NFL Players: Legal and Ethical Analysis and
Recommendations we set forth a comprehensive recommendation to address this issue. We propose restructuring
NFL club medical staff in such a way that the doctor treating the players has as his or her only concern the well-being
of the player-patient and has no advisory role to the club.
327
See Am. Acad. Pediatrics, Preparticipation Physical Evaluation (4th ed. 2010). This monograph was created
through the coordination of the American Academy of Family Physicians, American Academy of Pediatrics, American
College of Sports Medicine, American Medical Society for Sports Medicine, American Orthopaedic Society for Sports
Medicine, and the American Osteopathic Academy of Sports Medicine.
328
Am. Acad. Pediatrics, Preparticipation Physical Evaluation 3 (4th ed. 2010).

!
237!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
329
We are immensely grateful for the assistance of Karen G. Roos, PhD, MSPT, ATC, from California State
University, Long Beach in preparing this Chapter.
330
Nonetheless, we are uncertain what types of internal statistical analyses the leagues may be performing.
331
Gary A. Green et al., Mild Traumatic Brain Injury in Major and Minor League Baseball Players, 43 Am. J. Sports
Medicine 5, 1124 (2015) (discussing historic underreporting of concussions in sports); Carly D. McKay et al., The
Epidemiology of Professional Ice Hockey Injuries: A Prospective Report of Six NHL Seasons, 48 Brit. J. Sports Med.
57, 61 (2014) (discussing possibility that injuries in the NHL are underreported); Kristen L. Kucera et al., Validity of
Soccer Injury Data from the National Collegiate Athletic Association‘s Injury Surveillance System, 46(5) J. Athletic
Training 489 (2011).
332
See Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations, § 1(C) (2016); Christine M. Baugh et al., Perceived
Coach Support and Concussion Symptom-Reporting: Differences between Freshmen and Non-Freshmen College
Football Players, 42 J. L. Med., & Ethics 314 (2014) (analyzing possible explanations for under-reporting of
concussions by college football players); Zachary Y. Kerr et al., Disclosure and non-disclosure of concussion and
concussion symptoms in athletes: Review and application of the socio-ecological framework, 28 Brain Inj. 1009
(2014) (analyzing factors influencing athletes’ disclosure of sports-related concussions and concussion symptoms).
333
See Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations, § 1(C) (2016).
334
See Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations Recommendation 1:1-F (2016).
335
Gary A. Green et al., Mild Traumatic Brain Injury in Major and Minor League Baseball Players, 43 Am. J. Sports
Med. 5, 1124 (2015) (discussing historic underreporting of concussions in sports), available at
http://ajs.sagepub.com/content/early/ 2015/02/06/0363546514568089.full.pdf+html; E. Kroshus, L. D. Kubzansky, R.
E. Goldman, and S. B. Austin, Norms, Athletic Identity, and Concussion Under-Reporting among Male Collegiate Ice
Hockey Players: A Prospective Cohort Study, Annals of Behav. Med. (forthcoming, 2014); Christine M. Baugh et al.,
Frequency of head-impact-related outcomes by position in NCAA division I collegiate football players, 32 J.
Neurotrauma 5 (2015); Brad Partridge, Dazed and confused: sports medicine, conflicts of interest, and concussion
management, 11 J. Bioethical Inquiries 1, 67 (2014).
336
See NFL Head, Neck and Spine Committee‘s Protocols Regarding Diagnosis and Management of Concussions,
Nat’l Football League,
http://images.nflplayers.com/mediaResources/lyris/pdfs/NFL_Diagnosis_Mgmt_Concussion.pdf (last visited Sep. 18,
2015), archived at http://perma.cc/H2M7-U2KL (listing “potential concussion signs (observable)” and “potential
concussions symptoms”).
337
Id.
338
For discussion on the appropriate methodology for measuring player injuries, see John Orchard and Wayne
Hoskins, For Debate: Consensus Injury Definitions in Team Sports Should Focus on Missed Playing Time, 17 Clin. J.
Sport Med. 192 (2007); Lisa Hodgson et al. For Debate: Consensus Injury Definitions in Team Sports Should Focus
on Encompassing All Injuries 17 Clin. J. Sport Med. 188 (2007).
339
In this Chapter, we utilize the terminology commonly used by experts in sports injury data analysis. As such, the
term “player-game” represents one player playing in one game. Similarly, the term “player-season” represents one
player playing in one season regardless of how many games that player played in that season.
340
Paul McCrory, Consensus statement on concussion in sport: the 4th International Conference on Concussion in
Sport, Zurich, November 2012, 48 J. Athletic Trainers 4 (2013) (“Consensus Statement”).
341
Id. at 1.
342
We also acknowledge that there are concerns about subconcussive impacts, Steven P. Broglio, et al., Cognitive
Decline and Aging: The role of Concussive and Subconcussive Impacts, 40 Exerc. Sport Sci. Rev. 138 (2012), but
are unaware of any data on this issue from the leagues discussed in this Report.
343
Id.
344
See 2011 MLB CBA, Att. 36 (MLB Concussion Protocol); NFL Head, Neck and Spine Committee‘s Protocols
Regarding Diagnosis and Management of Concussions, Nat’l Football League,
http://images.nflplayers.com/mediaResources/lyris/pdfs/NFL_Diagnosis_Mgmt_Concussion.pdf (last visited Sep. 18,
2015), archived at http://perma.cc/H2M7-U2KL (NFL Concussion Protocol); NHL Concussion Evaluation and
Management Protocol 2015/16 (on file with authors); Concussion Evaluation and Management Protocol, MLS (2015)
(on file with authors). Information about the NBA’s concussion protocol was provided by the NBA – we did not review
the protocol directly.
345
See Consensus Statement at 1-4.
346
Compare Consensus Statement with NFL Concussion Protocol, supra note 344; MLB Concussion Protocol, supra
note 344; NBA.com: Official - Concussion Policy Summary, Nat’l Basketball Ass’n,
http://www.nba.com/official/concussion_policy_summary.html (last visited Sep. 18, 2015), archived at
http://perma.cc/D84E-JHLM; NHL Concussion Protocol, supra note 344; CFL Concussion Guidelines 2014 (on file
with author); MLS discusses concussion protocol, ESPN, Jan. 7, 2012,

!
238!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
http://espn.go.com/sports/soccer/news/_/id/7436065/mls-medical-staffers-target-concussion-protocol, archived at
http://perma.cc/78EF-6DWZ (describing MLS Concussion Protocol); Concussion Evaluation and Management
Protocol, MLS (2015) (on file with authors).
347
MLS’ Concussion Evaluation and Management Protocol does contain two provisions that appear unique and
potentially concerning. First, “[th]e Team Physician has the ultimate and absolute authority to decide when a player
should be removed for evaluation[.]” In contrast, the NFL empowers both officials and independent athletic trainers to
require a player to be removed from a game for evaluation. Second, while the MLS Protocol does require a player
who has suffered a concussion to consult with the club’s neuropsychologist, “[t]he team neuropsychologist should
NOT communicate to the player whether he or she thinks that the player should/should not return to play.” Instead,
“[th]e Team Physician has the ultimate and absolute authority to decide… whether that player is fit to return to play.”
In the event of a conflict between the Team neuropsychologist and Team Physician, Dr. Ruben Echemendia, chair of
MLS’ concussion program, is to be consulted. Nevertheless, the player is being deprived of potentially important
medical information concerning his health.
348
See, e.g., Dan Feldman, Clippers Violate NBA’s Concussion Policy, Play Austin Rivers With Concussion, Pro
Basketball Talk (Dec. 13, 2016, 11:54 AM), http://nba.nbcsports.com/2016/12/13/clippers-violate-nbas-concussion-
policy-play-austin-rivers-with-concussion/, archived at https://perma.cc/JE73-D9ZV.
349
Indeed, the NFL in 2015 and the NHL in 2016 adopted policies whereby they discipline clubs for failing to comply
with the concussion protocols. See James O’Brien, NHL Plans on Fining Teams Who Violate New Concussion
Protocol, Pro Hockey Talk (Oct. 11, 2016, 6:30 PM), http://nhl.nbcsports.com/2016/10/11/nhl-plans-on-fining-teams-
who-violate-new-concussion-protocol/, archived at https://perma.cc/34YL-VF85; Darin Gantt, NFL to fine, suspend
teams who don’t follow injury protocols, ProFootballTalk (Dec. 17, 2015, 6:00 AM),
http://profootballtalk.nbcsports.com/2015/12/17/nfl-to-fine-suspend-teams-who-dont-follow-injury-protocols/, archived
at https://perma.cc/8CH3-77F9.
350
Injury Surveillance in the NFL: an Update from Quintiles Outcome, Applied Clinical Trials, Aug. 30, 2012,
http://www.appliedclinicaltrialsonline.com/injury-surveillance-nfl-update-quintiles-outcome (last visited Jan. 21, 2016),
archived at https://perma.cc/5ZUF-9NF7.
351
Id.
352
Transcript – 2016 Injury Data Results Conference Call, NFL Communications, Jan. 29, 2016,
https://nflcommunications.com/Pages/Transcript---2016-Injury-Data-Results-Conference-Call.aspx, archived at
https://perma.cc/RKC6-352G.
353
Id.
354
Id.
355
This information was provided by the NFLPA.
356
Alan Schwarz, Walt Bogdanich, Jacqueline Williams, N.F.L.’s Flawed Concussion Research and Ties to Tobacco
Industry, N.Y. Times, Mar. 26, 2016, http://www.nytimes.com/2016/03/25/sports/football/nfl-concussion-research-
tobacco.html, archived at https://perma.cc/NM4N-SW4Q. See also NFL response to New York Times’ concussion
research story, NFL.com (Mar. 24, 2016, 4:11 PM), http://www.nfl.com/news/story/0ap3000000647389/article/nfl-
response-to-new-york-times-concussion-research-story, archived at https://perma.cc/Z3XE-8FQ6.
357
Other studies of NFL injury rates have been conducted using the clubs’ publicly released injury reports. See, e.g.,
David W. Lawrence, Paul Comper, and Michael G. Hutchison, Influence of Extrinsic Risk Factors on National Football
League Injury Rates, Orthopaedic J. Sports Med. (2016); David W. Lawrence, Paul Comper, and Michael G.
Hutchison, Descriptive Epidemiology of Musculoskeletal Injuries and Concussions in the National Football League,
2012–2014, Orthopaedic J. Sports Med. (2015). While these studies provide interesting analyses, NFL injury reports
are not the best data source, for reasons discussed in Chapter 17: The Media of our Report, Protecting and
Promoting the Health of NFL Players: Legal and Ethical Analysis and Recommendations.
358
Injury Surveillance in the NFL: an Update from Quintiles Outcome, Applied Clinical Trials, Aug. 30, 2012,
http://www.appliedclinicaltrialsonline.com/injury-surveillance-nfl-update-quintiles-outcome (last visited Sep. 18, 2014),
archived at http://perma.cc/FH93-5259.
359
Id.
360
This information was provided by the NFLPA.
361
These tables were created by examining the year-end NFLISS reports prepared by Quintiles for the year 2014,
and the reports presented at the NFL’s annual Health & Safety Press Conference during the week of the Super Bowl.
362
As a reminder, the injury reporting systems have changed in recent years. Consequently, the figures cannot be
strictly compared across the seasons and the mean is not definitively accurate.
363
Each year, there are 256 regular season NFL games. Thus, this figure is derived by dividing the number of injuries
in the “Games” column by 256.
364
Each year, there are 256 regular season NFL games. Thus, this figure is derived by dividing the number of injuries
in the “Games” column by 256.
365
The reports do not provide postseason data.
366
The reports do not provide postseason data.

!
239!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
367
The number of regular season players’ statistics were obtained from official NFL and NFLPA playtime figures. To
be clear, these statistics only include players who played in a regular season game and thus do not include players
who only played in the pre-season.
368
This statistic was obtained from calculations derived from official NFL and NFLPA playtime figures.
369
This Report does not include per-play injury data for the other leagues as that data is generally not available and
the definition of a “play” in other leagues can vary.
370
This statistic is calculated by dividing the total number of regular season game injuries from 2009–15 (10,577) by
the total number of game exposures over the same time period (164,864). The 164,864 statistic is calculated by
multiplying 7 seasons by 256 regular season games per season by 92 players per game. Clubs are limited to 46
active players during a game, 2011 NFL CBA, Art. 25, § 1, thus, 92 players have the opportunity to play each week.
371
This statistic is calculated by dividing the total number of regular season game concussions from 2009–16 (1,280)
by the total number of game exposures over the same time period (188,416). The 188,416 statistic is calculated by
multiplying 7 seasons by 256 regular season games per season by 92 players per game.
372
In other words, a mean of 2,182.6 players played in a regular season NFL game each season. The number of
player-seasons was obtained from official NFL and NFLPA playtime figures.
373
The NFL and NFLPA disagree on the mean career length of NFL players. The NFLPA has long stated that the
mean career is about 3.2 years. The NFL insists players’ mean career length is about 6 years. The difference arises
from which population of players is being examined. The NFLPA seems to include in their calculation every player
who ever signed a contract with an NFL club, regardless of whether they ever make the club or play in an NFL
regular season game, while also including players who are still active (and whose careers will thus exceed their
current length). On the other hand, the NFL’s calculation comes from players who made the opening day roster and
that played between 1993–2002, a slightly different era from today’s NFL. The website sharpfootballanalysis.com
ultimately found that players who were drafted between 2002 and 2007 have a mean career length of 5.0 years.
Average NFL Career Length, Sharp Football Analysis (Apr. 30, 2014),
http://www.sharpfootballanalysis.com/blog/?p=2133, archived at http://perma.cc/KR58-R8DA.
374
This information is from the year-end NFLISS reports prepared by Quintiles for the year 2014, and the reports
presented at the NFL’s annual Health & Safety Press Conference during the week of the Super Bowl.
375
Statistics for injuries other than concussions are only available in bar graph form. Consequently, we estimate the
injury figure based on the graph available.
376
See 2012 NFL Constitution and Bylaws, § 12.3(E).
377
Socalisteph, NFL PUP list, Injured Reserve, NFI List rules and the 2014 San Francisco 49ers, Superbowl Nation
Blog – Niners Nation (Jul. 18, 2014, 5:30 AM), http://www.ninersnation.com/2014/7/18/5914295/nfl-pup-list-rules-
injured-reserve-nfi-list-rules-49ers-2014, archived at https://perma.cc/D5YZ-87HX.
378
2011 NFL CBA, Art. 25, § 4.
379
2011 NFL CBA, Art. 25, § 1.
380
NFL Personnel (Injury) Report Policy, available at http://operations.nfl.com/media/2235/06-07-16-2016-injury-
report-policy.pdf, archived at https://perma.cc/D822-PXDN.
381
Id.
382
Id.
383
For additional information on gambling’s role in the NFL, see Christopher R. Deubert, I. Glenn Cohen, Holly
Fernandez Lynch, Protecting and Promoting the Health of NFL Players: Legal and Ethical Analysis and
Recommendations, § 18(A) (2016).
384
NFL Personnel (Injury) Report Policy, supra n. 380.
385
Tom Pelissero, Major change to NFL’s injury report will take some getting used to, USA Today (Aug. 21, 2016,
4:33 PM), http://www.usatoday.com/story/sports/nfl/2016/08/21/injury-report-probable-bill-belichick-
patriots/89080582/, archived at https://perma.cc/QT4C-MAA6.
386
See Scott Boeck, Skip Wood, Analysis: Injury report is game within the game, USA Today, Nov. 22, 2007,
http://usatoday30.usatoday.com/sports/football/nfl/2007-11-22-injury-report-cover_N.htm, archived at
http://perma.cc/SRU4-ZWY4. Midway through the 2012 season, 4 NFL teams had been fined $20,000 each for injury
report violations. Mike Florio, Rams rack up an injury-reporting fine, too, ProFootballTalk (Nov. 2, 2012, 10:44 PM),
http://profootballtalk.nbcsports.com/2012/11/02/rams-rack-up-an-injury-reporting-fine-too/, available at
http://perma.cc/S8TF-G78N. In 2009, the Jets were fined a total $125,000 for former quarterback Brett Favre’s injury
for the last 5 games of the season ($75,000 for the team and $25,000 each for G.M. Mike Tannenbaum and former
head coach Eric Mangini), the highest injury-reporting violation fine publicly announced. See Greg Bishop, Jets Still
Paying Price for Favre and Mangini, N.Y. Times, Sept. 16, 2009,
http://www.nytimes.com/2009/09/17/sports/football/17favre.html, archived at http://perma.cc/XV4N-GMTB.
387
Scott Boeck, Skip Wood, Analysis: Injury report is game within the game, USA Today, Nov. 22, 2007,
http://usatoday30.usatoday.com/sports/football/nfl/2007-11-22-injury-report-cover_N.htm.
388
See id.; Gregg Rosenthal, Redskins play the “questionable” game, again, ProFootballTalk.com (Sept. 25, 2010,
10:07 AM), http://profootballtalk.nbcsports.com/2010/09/25/redskins-play-the-questionable-game-again/, archived at
https://perma.cc/7MBX-ZXL4. Players reporting that coaches report the wrong injuries: Michael David Smith, Spikes,

!
240!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
Talib say Patriots file false injury reports (Mar. 19, 2014, 7:01 AM),
http://profootballtalk.nbcsports.com/2014/03/19/spikes-talib-say-patriots-file-false-injury-reports/, archived at
https://perma.cc/X6YP-H33S.
389
See Scott Boeck and Skip Wood, Analysis: Injury report is game within the game, USA Today, Nov. 22, 2007,
http://usatoday30.usatoday.com/sports/football/nfl/2007-11-22-injury-report-cover_N.htm, archived at
http://perma.cc/SRU4-ZWY4.
390
Jeff Zrebiec, John Harbaugh: ‘The injury report has no value’, Balt. Sun, Nov. 2, 2012,
http://www.baltimoresun.com/sports/ravens/ravens-insider/bal-harbaugh-criticizes-nfl-over-injury-report-20121102-
story.html, archived at https://perma.cc/E9TQ-3JPY.
391
Michael David Smith, Spikes, Talib say Patriots file false injury reports, ProFootballTalk (Mar. 19, 2014, 7:01 AM)
http://profootballtalk.nbcsports.com/2014/03/19/spikes-talib-say-patriots-file-false-injury-reports/, archived at
http://perma.cc/3GKS-GL5T.
392
See Gregg Rosenthal, Redskins play the “questionable” game, again, ProFootballTalk (Sept. 25, 2010,10:07 AM),
http://profootballtalk.nbcsports.com/2010/09/25/redskins-play-the-questionable-game-again/, archived at
http://perma.cc/N6S6-SULJ; John Niyo, NFL injury reports a weekly joke, Detroit News, Nov. 10, 2012,
http://www.detroitnews.com/article/20121110/OPINION03/211100317, archived at http://perma.cc/K8PQ-GST6; Scott
Boeck, Skip Wood, Analysis: Injury report is game within the game, USA Today, Nov. 22, 2007,
http://usatoday30.usatoday.com/sports/football/nfl/2007-11-22-injury-report-cover_N.htm, archived at
http://perma.cc/SRU4-ZWY4. The Pittsburgh Tribune-Review found “the NFL’s 1999 [Injury Reports] data was so
suspect, the Trib didn’t use it” (from Carl Prine, Bloody Sundays, Pittsburgh Trib.-Rev., Jan. 9, 2005,
http://triblive.com/x/pittsburghtrib/sports/steelers/s_291033.html#axzz3OdCi5UC7, archived at http://perma.cc/4A89-
N7AB.
393
Mike Florio, New Injury report creates plenty of questions, concerns, ProFootballTalk (Aug. 21, 2016, 8:20 PM),
http://profootballtalk.nbcsports.com/2016/08/21/new-injury-report-creates-plenty-of-questions-concerns/, archived at
https://perma.cc/ZMX9-XQT2.
394
See Darin Gantt, Julian Edelman won’t say whether he had concussion tests, ProFootballTalk (Feb. 1, 2015,
11:30 PM), http://profootballtalk.nbcsports.com/2015/02/01/julian-edelman-wont-say-whether-he-had-concussion-
tests/, archived at http://perma.cc/BS7C-2AUQ (discussing Patriots policy of prohibiting players from speaking about
injuries).
395
Copies of these waivers are included as Appendices L and M in our other report, Protecting and Promoting the
Health of NFL Players: Legal and Ethical Analysis and Recommendations (2016).
396
John Schlegel, MLB Instituting New Medical Records System, Major League Baseball, Mar. 1, 2010,
http://m.mlb.com/news/article/8632528/, archived at http://perma.cc/EH3X-B6CP.
397
Keshia M. Pollack, “Of Course They Are an Occupational Group!” Preventing Injuries Among Professional
Baseball Players, Johns Hopkins Center for Injury Res. & Policy, Mar. 4, 2014,
http://www.ucdenver.edu/academics/colleges/PublicHealth/research/ResearchProjects/piper/resources/Documents/In
jury%20seminar%20Co%20March%204%202014_revised.pdf, archived at http://perma.cc/7YJ2-429E.
398
See MLB CBA, Attachment 5 (Standard Form of Diagnosis); MLB CBA, Attachment 36, Ex. B (Concussion
Diagnostic Form for 7-Day Disabled List Placement).
399
It is unclear what is meant by a “preventative event.” Preventative events typically include specific strength or
balance training and exercise programs for the purpose of injury prevention and are common in sports. The programs
are coordinated by athletic trainers or strength and conditioning coaches to improve specific strength or coordination
in order to preemptively avoid injuries. However, it is unclear what the authors meant by preventative events in this
case.
400
Pollack, supra note 397. Players must provide consent for their records to be included in the system. Id. See also
Christopher S. Ahmad et al., Major and Minor League Baseball Hamstring Injuries: Epidemiologic Findings From the
Major League Baseball Injury Surveillance System, 42 Am. J. Sports Med. 1464, 1466 (2014) (“In the MLB EMR,
athletic trainers record all injuries, illnesses, and preventative visits for both baseball-related and non-baseball related
events for all players on their respective team as their medical-legal record.”)
401
See, e.g., Gary A. Green et al., Mild Traumatic Brain Injury in Major and Minor League Baseball Players, 43 Am. J.
Sports Med. 5, 1118–26 (2015).
402
Keshia M. Pollack et al., Developing and Implementing Major League Baseball’s Health and Injury Tracking
System, 183 Am. J. Epidemiology 1, 3 (2016).
403
See id.
404
Stan Conte, Christopher L. Camp, Joshua S. Dines, Injury Trends in Major League Baseball Over 18 Seasons:
1998-2015, 45 Am. J. Orthopedics 116 (2016).
405
Christopher S. Ahmad et al., Major and Minor League Baseball Hamstring Injuries: Epidemiologic Findings From
the Major League Baseball Injury Surveillance System, 42 Am. J. Sports Med. 1464 (2014).
406
Diane L. Dahm et al., Epidemiology and Impact of Knee Injuries in Major and Minor League Baseball Players, 45
Am. J. Orthopedics E54 (2016).

!
241!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
407
Struan H. Coleman et al., The Epidemiology of Hip and Groin Injuries in Professional Baseball Players, 45 Am. J.
Orthopedics 168 (2016).
408
Gary A. Green et al., Mild Traumatic Brain Injury in Major and Minor League Baseball Players, 43 Am. J. Sports
Med. 5 (2015).
409
Keshia M. Pollack et al., Developing and Implementing Major League Baseball’s Health and Injury Tracking
System, 183 Am. J. Epidemiology 1, 5 (2016).
410
Id. at 4.
411
Id. at 3.
412
Stan Conte, Christopher L. Camp and Joshua S. Dines, Injury Trends in Major League Baseball Over 18 Seasons:
1998-2015, 45 Am. J. Orthopedics 116, 118 (2016).
413
Major League Rule 2(g).
414
Between 1998 and 2015, the average duration of a player’s time on the DL was 55.1 days. Stan Conte,
Christopher L. Camp and Joshua S. Dines, Injury Trends in Major League Baseball Over 18 Seasons: 1998-2015, 45
Am. J. Orthopedics 116, 118 (2016).
415
MLB’s website provides spring training standings from which to calculate the number of spring training games.
See Standings, Major League Baseball, http://mlb.mlb.com/mlb/standings/exhibition.jsp?ymd=20161002 (last visited
Oct. 14, 2016), archived at https://perma.cc/W6KQ-ZBBZ.
416
Each of the 30 clubs plays 162 regular season games against another club, resulting in 2,430 games per season
(162 x 15). 2,430 games x 5 seasons = 12,150 games.
417
See World Series Winners, Records, and Results and Postseason Series, Baseball-Reference.com,
http://www.baseball-reference.com/postseason/ (last visited Oct. 14, 2016), archived at https://perma.cc/KP2W-
NRXR.
418
2012 MLB CBA, Art V.
419
See Gary A. Green et al., Mild Traumatic Brain Injury in Major and Minor League Baseball Players, 43 Am. J.
Sports Med. 5, 1118, 1125 (2015) (describing “the few practices in professional baseball”).
420
See Dr. Gary Green named Medical Director of Major League Baseball, Major League Baseball, April 14, 2010,
http://mlb.mlb.com/news/press_releases/press_release.jsp?ymd=20100414&content_id=9290282&vkey=pr_mlb&fext
=.jsp, archived at http://perma.cc/5EW8-7XRP.
421
According to MLB, the study was conducted pursuant to its partnership with Johns Hopkins and MLB did not
provide any funding or financial support.
422
See Gary A. Green et al., Mild Traumatic Brain Injury in Major and Minor League Baseball Players, 43 Am. J.
Sports Med. 5, 1118, 1121 (2015).
423
See Disabled List Data, Baseball Heat Maps, http://www.baseballheatmaps.com/disabled-list-data/, (last visited
Jan. 21, 2016), archived at http://perma.cc/2VNP-GD9P (providing spreadsheets of all players placed on the DL for
the 2010-15 seasons by gathering data from MLB.com).
424
This is likely not the case, as more injuries may be suffered as the season goes on due to cumulative strain. See
Randall Dick et al., Descriptive Epidemiology of Collegiate Men’s Baseball Injuries: National Collegiate Athletic
Association Injury Surveillance System, 1988–89 through 2003–04, 42 J. Athletic Training 183 (2007). Nevertheless,
any variance in the injury rates is challenging to determine and thus proceed based on this assumption. While
imperfect, we still believe the data and these calculations are sufficiently reliable and useful.
425
This figure was gathered from MLB.com’s “Sortable Player” statistics page by adding together all players who had
a plate appearance and all pitchers, and then removing those pitchers that also had a plate appearance.
426
Keshia M. Pollack et al., Developing and Implementing Major League Baseball’s Health and Injury Tracking
System, 183 Am. J. Epidemiology 1, 5 (2016).
427
Gary A. Green et al., Mild Traumatic Brain Injury in Major and Minor League Baseball Players, 43 Am. J. Sports
Med. 5, 1118, 1118-21 (2015). By comparison, a 2014 study examining DL data from 2001 to 2010 found only 33
concussions over that 10-season period. Leslie E. Schwindel et al., Epidemiology and Outcomes of Concussions in
Major League Baseball, 2 Annals of Orthopedics & Rheumatology 3, 1022, 1022 (2014). The smaller figures were
likely the result of lesser awareness and failure to diagnose concussions in the earlier seasons. Indeed, the study
found that 0 concussions were reported in 2001, while 10 were reported in 2010. Id.
428
Gary A. Green et al., Mild Traumatic Brain Injury in Major and Minor League Baseball Players, 43 Am. J. Sports
Med. 5, 1118, 1125 (2015).
429
Each of the 30 clubs plays 162 games, resulting in a total of 2,430 games per season (because each game
involves two clubs, we multiplied 162 x 15). Thus, in two seasons, there are 4,860 games (2,430 x 2).
430
This statistic is calculated by dividing the total number of regular season game concussions from 2011–12 (41) by
the total number of game exposures over the same time period (138,024). The 138,024 statistic is calculated by
multiplying 2 seasons by 2,430 regular season games per season by 28.4 players per game. The Green Study
provided that there were 69,043 games played per season. With 2,430 regular season games per season, we can
thus calculate that a mean of 28.4 players play in each MLB game.

!
242!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
431
MLB has a 7-day DL “solely for the placement of players who suffer a concussion.” 2012 MLB CBA, Att. 36, ¶ 2.
Given the specific nature of this DL, there are likely very few (if any) instances in which a player suffered a
concussion and was not placed on the DL.
432
Gary A. Green et al., Mild Traumatic Brain Injury in Major and Minor League Baseball Players, 43 Am. J. Sports
Med. 5, 1118, 1120 (2015) (“To estimate exposure, we based the average number of players per team per game on
analysis of regular-season game participation via box scores that are publicly available. This average number over a
season, multiplied by the number of team games… was used as an estimate of game exposures[.]”)
433
Green, supra note 432 at 1122 (finding catchers accounted for 40% of concussions); see also Schwindel, supra
note 427, at 1022-23 (finding that 30.3% of concussions were suffered by catchers).
434
Green, supra note 432 at 1122; see also Schwindel, supra note 427 at 1022–23.
435
William D. Witnauer, Richard G. Rogers & Jarron M. Saint Onge, Major league baseball career length in the 20th
century, 26 Population Res. & Pol’y Rev. 4, 371-386 (2007).
436
MLB CBA, Attachment 36 § 2(A). “Acute” is not defined in the CBA.
437
Major League Rule 2(g)(1); MLBPA, MLB Announce Details of New Labor Agreement, MLBPA (Dec. 2, 2016),
http://www.mlbplayers.com/ViewArticle.dbml?DB_OEM_ID=34000&ATCLID=211336390, archived at
https://perma.cc/4XUA-2DAW (announcing replacement of 15-day DL with 10-day DL).
438
MLB CBA, Attachment 5 (Standard Form of Diagnosis). There is a different form for clubs attempting to place a
player who has suffered a concussion on the 7-day DL. MLB CBA, Attachment 36, Ex. B (Concussion Diagnostic
Form for 7-Day Disabled List Placement). The Concussion Diagnostic Form for 7-Day Disabled List requires clubs to
provide such information as the date of injury, diagnosis description, event that cause the injury, whether the player
was removed from the game, and the basis of the concussion diagnosis (including the SCAT2 Assessment Form).
The form also requests video information if available. Id.
439
MLB CBA, Attachment 5 (Standard Form of Diagnosis).
440
MLB CBA, Art. XIII(C).
441
See Major League Rule 2(g)(1). For example, a player placed on the 15-day DL is not eligible to play in an MLB
game until at least 15 days have passed, though he may remain out of play longer if his rehabilitation is not complete
after 15 days
442
MLB CBA, Art. XIII(G)(4) (emphasis added).
443
Id.
444
Major League Rule 2(a).
445
Center to Standardize Health Care for NBA Players with Easy-to-Use and Automated System “HealthAthlete”,
Globe Newswire, Nov. 14, 2012, http://globenewswire.com/news-release/2012/11/14/505082/10012449/en/Cerner-to-
Standardize-Health-Care-for-NBA-Players-With-Easy-to-Use-and-Automated-System-HealtheAthlete.html, archived
at http://perma.cc/8TEG-9LKQ.
446
See id.
447
2017 NBA CBA, Art. XXII, § 8.
448
NBA CBA, Art. XXII, §§ 3, 7.
449
Mark C. Drakos, Benjamin Domb, Chad Starkey, Lisa Callahan, Answorth A. Allen, Injury in the National
Basketball Association: A 17-Year Overview, 2 Sports Health 284, 285 (2010).
450
Id.
451
Id.
452
Id.
453
See Athletic Health Management, Cerner Corp.,
https://www.cerner.com/solutions/individuals_and_families/athletic_health_management/ (last visited Sept. 22, 2015),
archived at http://perma.cc/4BGH-HNB5.
454
!Baxter Holmes and Tom Haberstroh, The Cutting Edge: Injury Prediction and Prevention, ESPN (Jun. 7, 2016),
http://www.espn.com/nba/story/_/id/16009403/cutting-edge-injury-prediction-prevention, archived at
https://perma.cc/PF6G-GDTZ.!
455
Mark C. Drakos, Benjamin Domb, Chad Starkey, Lisa Callahan, Answorth A. Allen, Injury in the National
Basketball Association: A 17-Year Overview, 2 Sports Health 284 (2010).
456
Id. at 285.
457
Id.
458
Id.
459
Id.
460
Id. at 289–90.
461
Id. at 285.
462
Id.at 286.
463
Id. at 286.
464
NBA clubs play 82 games a season, except in the 1998–99 season they only played 50 due to a lockout.
Additionally, the NBA added clubs prior to the 1989–90, 1995–96 and 2004–05 seasons.

!
243!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
465
This statistic was calculated by adding together the number of players who played in at least one NBA game in
each of the 17 seasons covered by the Drakos study. During the seasons in question, a range of 353 to 464 players
would make an appearance in an NBA game during any given season.
466
Mark C. Drakos, Benjamin Domb, Chad Starkey, Lisa Callahan, Answorth A. Allen, Injury in the National
Basketball Association: A 17-Year Overview, 2 Sports Health 284, 287 (2010). The Drakos Study provided the total
number of game-related injuries by body part. To obtain the figures in this Report, we divided these totals by the 17
seasons of the study.
467
Id. at 288. There were 1,066 ankle sprains during the 17 years of the study, equaling 62.7 per year (1,066/17).
468
Id.
469
Jeff Stotts, Only 9 NBA Players Got Concussion This Year, FiveThirtyEight (May 21, 2014, 1:43 pm),
http://fivethirtyeight.com/datalab/only-9-nba-players-got-concussions-this-year/, archived at http://perma.cc/KY4L-
B32Y.
470
This data was gathered from basketball-reference.com.
471
Susan Konig, Financial Planning for the Pros, 34 Registered Representative (Apr. 2010), available at 2010 WLNR
26366417.
472
If we assume that the total number of player injuries in a season has remained constant at the mean of 369.8
observed during the period studied in the Drakos Study, we can calculate that the 9 concussions that occurred during
the 2013–14 season represented 2.4% of all player injuries (369.8/9). Nevertheless, because the data is not from the
same year, this calculation method is of questionable validity.
473
See Larry Coon, NBA Salary Cap FAQ, CBA FAQ, July 8, 2015, http://www.cbafaq.com/salarycap.htm#Q79,
archived at http://perma.cc/X3CS-F58N; NBA CBA, Art. XXIX § 2.
474
Coon, supra n. 473.
475
Id.
476
!This!information!was!provided!by!the!NBA!-!we!did!not!review!the!!policy!directly.!
477
2017 NBA CBA, Art. XXII, § 4(d).
478
2017 NBA CBA, Art. XXII, § 4(e).
479
Athlete Health Management System, Athlete RMS, http://athleterms.com/Solutions/AHMSPro.aspx (last visited
Sept. 22, 2015), archived at http://perma.cc/7L67-4AZT.
480
Carly D. McKay et al., The Epidemiology of Professional Ice Hockey Injuries: A Prospective Report of Six NHL
Seasons, 48 Brit. J. Sports Med. 57, 57 (2014).
481
Id.
482
Id.
483
Id.
484
Id. at 61.
485
Id.
486
Id. at 58. The study calculated total AEs by multiplying 82 games per season per club by 30 NHL clubs by 19
players per game, equaling 46,740 per season. The 19 players per game figure is the equivalent of a club’s entire
roster each night, less a backup goaltender. We find this calculation to be reliable. Unlike in other sports, every player
on an NHL club’s roster will play every game, except for the backup goaltender.
487
See id. at 59.
488
Id.
489
Id. at 60.
490
There are 82 games per season and 30 NHL clubs. Thus, this statistic was determined by multiplying 82 by 15 (30
NHL clubs divided by 2 clubs per game) by the 6 seasons in the study.
491
This statistic is calculated by dividing the total number of regular season game injuries from 2006–12 (4,368) by
the total number of game exposures over the same time period (299,136). The 299,136 statistic is calculated by
multiplying 6 seasons by 1,312 regular season games per season by 38 players per game. Although NHL clubs are
permitted to have 20 players active for each game, see Jay Levin, The Business of the Game: Roster Limits,
NASHVILLE PREDATORS, July 11, 2008, http://predators.nhl.com/club/news.htm?id=439739, archived at
http://perma.cc/W9FB-MUW8 (describing “a 20-player ‘dressed list’ for games”); Bounty of riches for Carbonneau;
Wounded return, MONTREAL GAZETTE, Oct. 17, 2008, available at 2008 WLNR 28430795 (Montreal Canadians coach
discussing challenge of choosing which 20 players will dress for the game), the backup goalie normally does not play,
making 19 players per game per club a more accurate statistic. See Brian Benson et al., A Prospective Study of
Concussions Among National Hockey League Players During Regular Season Games: The NHL-NHLPA Concussion
Program, 183 CANADIAN MED. ASS’N J. 905, App. 2 (2011) (basing athlete-exposure calculations on only “one goalie
playing per team, per game”).
492
The study provides the following number of players for each season: 840 in 2006–07; 843 in 2007–08; 837 in
2008–09; 838 in 2009–10; 891 in 2010–11; and, 895 in 2011–12. See McKay at 58.
493
Id. at 59.
494
Id. at 60.

!
244!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
495
An additional study on concussions in the NHL worth considering is Michael G. Hutchison et al., A systematic
video analysis of National Hockey League (NHL) concussions, part 1: who, when, where and what? Br. J. Sports
Med. 1 (2013). This study analyzed the situational factors associated with concussions in the NHL, such as contact
with an opponent and position. The study analyzed concussions that occurred during the 2006–07, 2007–08, 2008–
09, and 2009–10 seasons. However, the analysis did not include all concussions that occurred during the 2009–10
season. Instead, the authors stopped their data collection as of December 31, 2009. Consequently, the data from this
study is not the best data for determining the number of concussions that occur during an NHL regular season.
496
Richard A. Wennberg & Charles H. Tator, Concussion Incidence and Time Lost from Play in the NHL During the
Past Ten Years, 35 Can. J. Neurological Sci. 647, 649 (2008).
497
See id. at 649.
498
Id.
499
This statistic was calculated by dividing 688 concussions by 11,931 regular season games. There are 82 regular
season games in the NHL each season. The number of games per season, however, depends on the number of
clubs. There were 26 clubs in 1997–98, 27 in 1998–99, 28 in 1999–00, and 30 from 2000–01 and beyond. Thus, the
total number of games played by clubs during this time equals 23,862 [(26 clubs x 82 games x 1 season) + (27 clubs
x 82 games x 1 season) + (28 clubs x 82 games x 1 season) + (30 clubs x 82 games x 7 seasons)]. Because each
game involves two clubs, you then divide the total number of games (23,862) by 2 to reach the number of unique
games.
500
Id. at Table 2.
501
The NHL/NHLPA Concussion Program, launched in 1997, was the first professional sports working group program
that addressed concussions. See Frequently Asked Questions About Concussions, Nat’l Hockey League, Feb. 7,
2011, http://www.nhl.com/ice/news.htm?id=551900, archived at http://perma.cc/63YK-8C8H. Through input from the
NHLPA, physicians, and athletic trainers, the Concussion Program has sought to better understand concussions. See
id. The Program has resulted in the implementation of mandatory neurophysiological baseline testing for all players,
as well as changes to rules, equipment, and the playing environment. Id.
502
Brian Benson et al., A Prospective Study of Concussions Among National Hockey League Players During Regular
Season Games: The NHL-NHLPA Concussion Program, 183 Can. Med. Ass’n J. 905 (2011).
503
See id.
504
Id. at 907.
505
This statistic was calculated by dividing 559 concussions by 8,241 regular season games. The 8,241 regular
season game statistic was calculated using the same methodology as described in footnote dd.
506
See footnote bb for an explanation of this assumption.
507
This statistic was calculated by multiplying 8,241 regular season games (see footnote dd for methodology) by 38
players per game.
508
See id.
509
James Wisniewski, NHL still grappling with concussions, ESPN, June 8, 2014,
http://espn.go.com/nhl/playoffs/2014/story/_/id/11051889/nhl-says-concussions-decreased-protocol-remains-
imperfect, archived at http://perma.cc/YD2R-CPUE (“According to data from STATS provided to The Associated
Press, there were 53 concussions during the regular season, a sharp decline from the 78 reported during the
league’s last full season two years ago.”)
510
This statistic is calculated by dividing 82 by regular season games by 48 regular season games and multiplying it
by 78 concussions that occurred during the shortened 2012–13 regular season.
511
The number of games in the 2012–13 season is calculated by multiplying 30 clubs x 48 regular season games and
then dividing by 2 clubs per game, to reach 720 games. The number of games in the 2013–14 season is calculated
by multiplying 30 clubs x 82 regular season games and then dividing by 2 clubs per game, to reach 1,230 games. 720
+ 1,230 = 1,950.
512
This statistic was calculated by dividing 1,950 regular season games over the two seasons by 131 concussions.
513
This statistic was calculated by dividing 131 concussions by 1,950 regular season games.
514
This statistic is calculated by multiplying 1,950 regular season games over the two seasons by 38 players.
515
The study provides the following number of players for each season: 840 in 2006-07; 843 in 2007-08; 837 in 2008-
09; 838 in 2009-10; 891 in 2010-11; and, 895 in 2011-12. See McKay at 58.
516
Readers should be cautioned that this calculation applies statistics from the time period of the McKay study to
other years. In normal statistical methods, this is not preferred as it makes assumptions that various considerations
do not change over time. We are unaware of any policy or practice changes that would have caused a meaningful
change in the number of players per regular season between the years of the McKay study (2006–12) and the years
of the most recent concussion data (2012–14). However, we again caution that we are extrapolating data from the
2012–13 season as if it were a full 82 game regular season.
517
Average Length of an NHL Player Career, QuantHockey.com,
http://www.quanthockey.com/Distributions/CareerLengthGP.php (last visited Aug. 28, 2015), archived at
http://perma.cc/95QB-X9P9.

!
245!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
518
As explained in the preceding footnote, this estimate is limited by the fact that we are comparing data from two
different time periods.
519
2013 NHL CBA, § 16.11(a).
520
2013 NHL CBA, § 16.4(a).
521
2013 NHL CBA, § 16.11(d).
522
2013 NHL CBA, § 16.11(a).
523
Id. Although clubs have a 23-man Active Roster, only 20 players (18 skaters and 2 goaltenders) are permitted to
dress for each game. NHL Official Rules, Rule 5.1 (2014-15).
524
See 2013 NHL CBA, Art. 1 (defining “Reserve List” as, among other things, “all Players signed to a[] [Standard
Player Contract],” and limiting the Reserve List to “[n]o more than 50 Players signed to a[] [Standard Player
Contract]”).
525
Stu Hackel, The Morning Skate: N.H.L.’s New Injury-Disclosure Policy Draws Heavy Criticism, Slapshot Blog, N.Y.
Times (Nov. 10, 2008, 3:26 p.m.), http://slapshot.blogs.nytimes.com/2008/11/10/the-morning-skate-nhls-new-injury-
disclosure-policy-draws-heavy-criticism/, archived at http://perma.cc/X5FS-JD9Q (quoting the policy).
526
Id.
527
2013 CBA, Art. 34, § 3(c)(iii).
528
Despite the authorizations contained in the CBA, in re: Nat’l Hockey League Players’ Concussion Injury Litigation,
120 F. Supp.3d (D. Minn. 2015), the Court expressed that the NHL’s disclosure of player medical information might
violate the Americans with Disabilities Act (“ADA”) confidentiality provisions. See id. at 951.
529
Stu Hackel, The Morning Skate: N.H.L.’s New Injury-Disclosure Policy Draws Heavy Criticism, Slapshot Blog, N.Y.
Times (Nov. 10, 2008, 3:26 p.m.), http://slapshot.blogs.nytimes.com/2008/11/10/the-morning-skate-nhls-new-injury-
disclosure-policy-draws-heavy-criticism/, archived at http://perma.cc/X5FS-JD9Q.
530
See Curtis Rush, The “Upper-Body” Injury—from Pat Quinn’s Brain to NHL Lexicon, Toronto Star, Mar. 18, 2014,
http://www.thestar.com/sports/leafs/2014/03/18/the_upperbody_injury_from_pat_quinns_brain_to_nhl_lexicon.html,
archived at http://perma.cc/7KDB-B6Q6; see also NHL Injuries, ESPN, http://espn.go.com/nhl/injuries (last visited
Oct. 28, 2015).
531
A.J. Perez, NHL Unlikely to Get Closer to Ending Little Disclosure on Injuries, CBS Sports, Mar. 24, 2011,
http://www.cbssports.com/nhl/story/14850387/nhl-unlikely-to-get-closer-to-ending-little-disclosure-on-injuries,
archived at http://perma.cc/5YED-UDL7.
532
See Chris Zelkovich, CFL Concussions Not Always Revealed to Fans, Toronto Star, Apr. 7, 2011,
http://www.thestar.com/sports/football/argos/2011/04/07/cfl_concussions_not_always_revealed_to_fans.html,
archived at http://perma.cc/T3Q8-2AZW.
533
Mark Masters, ‘Awareness Is Half The Battle’ for CFL and Concussions, Nat’l Post, Apr. 7, 2011,
http://sports.nationalpost.com/2011/04/07/awareness-is-half-the-battle-for-cfl-and-concussions/, archived at
http://perma.cc/T3Q8-2AZW (“There were 50 concussions recorded in 85 CFL games last year”).
534
Id. The only other study our research revealed concerning CFL injuries concerned concussions suffered by CFL
players during the 1997 season. J. Scott Delaney et al., Concussions During the 1997 Canadian Football League
Season, 10 Clin. J. Sport Med. 9 (2000). The data was self-reported in the form of a voluntary questionnaire and the
understanding of concussions has changed considerably since 1997. For these reasons, the data in the study cannot
be considered useful today. Nevertheless, of the 289 players who responded to the questionnaire, 8.4% reported that
they had suffered a concussion, but 44.8% reported one or more concussion symptoms. Based on these responses,
the researchers concluded that concussions are likely substantially underreported. Id.
535
The nine CFL clubs each play 18 regular season games, for a total of 81 games. In addition, there are five playoff
games, for a total of 86 regular season and postseason games. It is thus unclear what games may or may not have
been included to reach a figure of 85 games.
536
Marika Washchynshyn, Is the Canadian Football League Safer than the NFL?, Complex (Nov. 25, 2015),
http://www.complex.com/sports/2015/11/cfl-concussions, archived at https://perma.cc/G47Y-RTT5.
537
Id.
538
This statistic is calculated by dividing the estimated number of concussions (57) by the total number of games in a
regular season (81). We can calculate that there are 81 regular season games by multiplying the number of CFL
clubs (9) by the number of regular season games each club plays (18), and dividing by two to factor in that in each
game there are two clubs playing.
539
This statistic is calculated by dividing the estimated number of concussions (57) by the total number of game
exposures over the same time period (7,128). The 7,128 statistic is calculated by multiplying 81 regular season
games per season by 88 players per game. CFL clubs maintain a 44-player active roster. Rosters Glossary, CFLDB,
https://cfldb.ca/glossary/rosters/ (last visited Sept. 22, 2015), archived at http://perma.cc/77LF-2E4Y.
540
The reserve list consists of two players who do not dress for a club’s game. Rosters Glossary, CFLdb,
https://cfldb.ca/glossary/rosters/ (last visited Sept. 22, 2015), archived at http://perma.cc/77LF-2E4Y. Players on the
injured list do not count toward the reserve list. Id.
541
The Game, Can. Football League, http://www.cfl.ca/page/game_rule_ratio (last visited Sept. 22, 2015), archived at
http://perma.cc/5RRT-RSGZ.

!
246!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
542
See Rosters Glossary, CFLdb, https://cfldb.ca/glossary/rosters/ (last visited Sept. 22, 2015), archived at
http://perma.cc/77LF-2E4Y; CFL CBA, § 14.02(F).
543
See Id.
544
See Zelkovich, supra note 532; CFL CBA, Art. 29 § 2.
545
Cerner Collaborates With Major League Soccer to Improve Medical Care for Professional Athletes, Cerner Corp.,
August 9, 2011, http://phx.corporate-ir.net/phoenix.zhtml?c=118401&p=irol-newsArticle&ID=1594607, archived at
http://perma.cc/R74X-993X.
546
Id.
547
Id.
548
MLS Medical Policies and Procedures Manual § V.11 (2015).
549
Bruce E. Morgan and Michael A. Oberlander, An Examination of Injuries in Major League Soccer, 29 Am. J.
Sports Med. 426 (2001).
550
Id. at 427.
551
2013/14 Season Report - UEFA Elite Club Injury Study, UEFA (2014),
http://www.uefa.org/MultimediaFiles/Download/uefaorg/Medical/02/19/04/32/2190432_DOWNLOAD.pdf, archived at
http://perma.cc/Q6GL-RTAA.
552
Id. at § 5.2.1.
553
Jan Ekstrand, Martin Haägglund, and Markus Waldén, Injury Incidence and Injury Patterns in Professional
Football: The UEFA Injury Study, 45 Brit. J. Sports Med. 553, 553 (2011).
554
Id. at 3.
555
Id.
556
2013/14 Season Report - UEFA Elite Club Injury Study, § 5, Table 1, UEFA (2014),
http://www.uefa.org/MultimediaFiles/Download/uefaorg/Medical/02/19/04/32/2190432_DOWNLOAD.pdf, archived at
http://perma.cc/Q6GL-RTAA.
557
Id. at § 1, § 4.
558
Id. at § 5.
559
Id. at § 4.
560
The Federation International de Football Association (“FIFA”) is the international governing body for the sport of
soccer. See Who We Are, FIFA, http://www.fifa.com/about-fifa/who-we-are/index.html (last visited Sept. 22, 2015),
archived at http://perma.cc/GH54-3XKS.
561
Law of the Game 2013-2014, FIFA (2013),
http://www.fifa.com/mm/document/footballdevelopment/refereeing/81/42/36/log2013en_neutral.pdf, archived at
http://perma.cc/VJJ8-6G7V, at p. 17.
562
2013/14 Season Report - UEFA Elite Club Injury Study, § 5, Table 1, UEFA (2014),
http://www.uefa.org/MultimediaFiles/Download/uefaorg/Medical/02/19/04/32/2190432_DOWNLOAD.pdf, archived at
http://perma.cc/Q6GL-RTAA.
563
Id. at Table 2.
564
See Concussion policies by league, USA Today, Oct. 11, 2012,
http://www.usatoday.com/story/sports/2012/10/11/concussions-nascar-nfl-mlb-nhl-nba/1628129/, archived at
http://perma.cc/WV7S-5PG3.
565
Roster Rules and Regulations, Major League Soccer, http://pressbox.mlssoccer.com/content/roster-rules-and-
regulations (last visited Sept. 22, 2015), archived at http://perma.cc/9BLN-R7QD.
566
Id.
567
Id.
568
Id.
569
Id.
570
Major League Soccer Fines LA Galaxy for Violating Injury Report Policy, Major League Soccer, June 24, 2011,
http://pressbox.mlssoccer.com/content/major-league-soccer-fines-la-galaxy-violating-injury-report-policy, archived at
http://perma.cc/EC3H-HY5C.
571
MLS Medical Policies & Procedures Manual, § IX.B (2015).
572
Id.
573
Id.
574
2015 MLS CBA, Ex. 2.
575
MLS Medical Policies & Procedures Manual, § IX.B.11 (2015).
576
Id.
577
We remind the reader that we use the data that we consider the most reliable—and generally the most recent—in
order to provide the most accurate assessment of injury rates in sports today. We also remind the reader that our
data is limited to regular season data.
578
As mentioned above, there was no publicly available data on CFL injuries.
579
There is no recent data concerning player injuries in MLS.

!
247!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
580
As mentioned above, UEFA is not a league but instead an organization of member clubs who participate in many
different leagues. Consequently, our review of UEFA here is constrained to injury data and does not include an
analysis of the policy issues covered in this Chart.
581
This statistic includes injuries that occurred during regular season games, not practices, except for MLB. Data for
MLB only includes as injuries those injuries that caused a player to be placed on the Disabled List, regardless of the
reason the player was placed on the Disabled List. Nevertheless, we remind the reader that practices are infrequent
during the MLB regular season.
582
The UEFA Report did not provide data on how many players played in the games for which injury data was
compiled and, due to the variations in season types and lengths among the different UEFA clubs, this figure is difficult
to calculate.
583
This statistic only includes concussions that occurred during regular season games.
584
It is unclear whether the CFL data concerning concussions includes pre-season or postseason games.
585
The UEFA Report only provided data from a select number of clubs.
586
MLS refuses to provide data on the number of concussions suffered by its players.
587
Although some concussion data are available concerning the CFL, reliable data on the number of players per
season are not.
588
The UEFA Report did not provide data on how many players played in the games for which injury data was
compiled and, due to the variations in season types and lengths among the different UEFA clubs, this figure is difficult
to calculate.
589
It is important to remember that this statistic is a relative statistic—it does not reflect the actual number of
concussions in the leagues.
590
Here, we use the terminology from the studies relevant to each of the leagues—some identify the most common
injury while others identify the most commonly injured body part.
591
We emphasize that this statistic is a mean of all player positions. As discussed in the full Report, we know that
rates vary depending on a player’s position. Unfortunately, we do not have sufficient data to do position-by-position
analysis. Nevertheless, even in the absence of that data we think the comparison of means is useful.
592
However, a player or his immediate family (where appropriate) “shall have the right to approve the terms and
timing of any public release of medical information relating to any injuries or illnesses suffered by that player that are
potentially life- or career-threatening, or that do not arise from the player’s participation in NBA games or practices.”
2017 NBA CBA, Art. XXII, § 4(e).
593
While the other leagues also have pre-season training camps and practices, it is generally believed that the
physical intensity and competitiveness of an NFL training camp surpasses the training camp environment in the other
leagues.
594
See Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations, App. I (2016) (discussing and providing history of health-
related rule changes in the NFL). See also Joseph S. Torg et al., The National Football Head and Neck Injury
Registry, 14-Year Report on Cervical Quadriplegia, 1971- Through 1984, 254 J. Am. Med. Ass’n 3439 (1985)
(discussing NCAA rule changes in response to player health data).
595
Short-term inactive lists are not practical in MLB. MLB rosters are limited to 25 players, including the five-man
starting pitching staff, each of whom only pitches every fifth game. Players on the club’s Disabled List do not count
towards a club’s 25-man roster. Thus, if MLB’s Disabled List did not include time requirements and clubs could place
players on the Disabled List one game at a time, the club could place the starting pitchers on the Disabled List and
only take them off the list when they were going to pitch. If, on any given day, four of the five starting pitchers are on
the Disabled List, the club could then have four other players on the roster in their place, effectively creating a 29-
man roster since the starting pitchers would return to action without having missed any games in which they were
scheduled to pitch.
596
See, e.g., AMA Code Opinion 3.1.5 – Professionalism in Relationships with Media, Am. Med. Ass’n, available at
http://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics.page (last visited Aug. 1,
2016), archived at https://perma.cc/ZR8K-FC93 (“To safeguard patient interests when working with representatives of
the media, all physicians should: (a) Obtain consent from the patient or the patient’s authorized representative before
releasing information; (b) Release only information specifically authorized by the patient or patient’s representative or
that is part of the public record”); Fédération Internationale de Médecine [du Sport, Code of Ethics, ¶ 11 (“[n]o
information about an athlete may be given to a third party without the consent of the athlete.”)
597
See, e.g., Mark A. Hall, et al., Health Care Law and Ethics 168–69 (2003) (collecting cases and statutes for the
proposition that doctors have both common law and statutory obligations to keep patient information confidential);
Health Insurance Portability and Accountability Act (“HIPAA”), 45 C.F.R. § 164.502 (prohibiting use or disclosure of
health information except in certain situations, including where patient has provided consent).
598
See, e.g., Charles A. Welch, Sacred Secrets - The Privacy of Medical Records, 435 N. Eng. J. Med. 371 (2001);
Mark A. Rothstein, Improve Privacy in Research By Eliminating Informed Consent? IOM Report Misses the Mark, 37
J.L. Med. & Ethics 507, 510 (2009) (describing the confidentiality of medical information as a “sacred trust” with
healthcare providers). See also U.S. v. Westinghouse Elec. Corp., 638 F.2d 570, 577 (“Information about one’s body

!
248!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
and state of health is matter which the individual is ordinarily entitled to retain within the private enclave where he
may lead a private life.”) (Internal quotations and citations omitted).
599
See Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations, § 2(C) (2016) (discussing NFL club doctors’ legal and
ethical obligations to keep player health information confidential, including when such information can be provided to
the clubs).
600
See id.
601
Josh Alper, Brandon Browner on Earl Thomas, Richard Sherman: Hit that shoulder, hit that elbow, ProFootballTalk
(Jan. 26, 2015, 3:15 PM), http://profootballtalk.nbcsports.com/2015/01/26/brandon-browner-on-earl-thomas-richard-
sherman-hit-that-shoulder-hit-that-elbow/, archived at http://perma.cc/B5YF-NT3C.
602
Mike Florio, Concussions take on a strategic component, ProFootballTalk (Jan. 23, 2012, 10:09 PM),
http://profootballtalk.nbcsports.com/2012/01/23/concussions-take-on-a-strategic-component/, archived at
http://perma.cc/5D6N-AMVT.
603
Mike Florio, Disclosure of injury information continues to put NFL players in a delicate spot, ProFootballTalk (July
10, 2015, 12:34 PM), http://profootballtalk.nbcsports.com/2015/07/10/disclosure-of-injury-information-continues-to-
put-nfl-players-in-a-delicate-spot/, archived at http://perma.cc/PYL4-KMRY (“When it comes to disclosing injury
information, the NFL has struggled at times to strike the right balance. To create a sense of transparency (and in turn
to discourage gamblers from pursuing inside information by cozying up to players, coaches, and other team
employees), the NFL has developed an injury-reporting system far more complex than, for example, hockey’s upper-
body/lower-body shell game.”)
604
Id.
605
See NFL League Policies for Players, 52 (2013) (“The NFL opposes all forms of illegal gambling, as well as legal
betting on NFL games or other professional, college or Olympic sports. Such activity negatively affects the interests,
welfare and integrity of the NFL, its games, clubs, players and coaches, and diminishes public confidence in
legitimate sport. Equally important, even social gambling among co-workers can lead to discord, violence and a loss
of team cohesion.”)
606
See NFL League Policies for Players, 52–58 (2013) (“League policy strictly prohibits NFL Personnel [including
players] from participating in or facilitating any form of illegal gambling,” “League policy prohibits advertising or
promotional activities by NFL Personnel [including players] that reasonably can be perceived as constituting affiliation
with or endorsement of gambling or gambling-related activities”).
607
See Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations, § 18(A) (2016).
608
See Michael B. Engle, The No-Fantasy League: Why the National Football League Should Ban Its Players from
Managing Personal Fantasy Football Teams, 11 DePaul J. Sports L. & Contemp. Probs. 59, 85 (2015) (discussing
Karras and Hornung cases).
609
Additionally, gambling on football represents approximately 45% of all legal gambling. See David Purdum,
Wagers, Bettor Losses Set Record, ESPN (Jan. 30, 2015), http://espn.go.com/chalk/story/_/id/12253876/nevada-
sports-bettors-wagered-lost-more-ever-2014, archived at http://perma.cc/RKR8-WPD7. Thus, there is substantially
less gambling in the other sports, which might explain their less robust injury reporting policies.
610
For examples of such studies in high school and college sports, see Barry P. Boden et al., Catastrophic Injuries in
Pole Vaulters, A Prospective 9-Year Follow-up Study, 40 Am. J. Sports Med. 1488 (2012); Frederick O. Mueller and
Robert C. Cantu, Catastrophic injuries and fatalities in high school and college sports, fall 1982–spring 1988, 22 Med.
& Sci. in Sports & Exercise 737 (1990).
611
Some of the studies discussed in this Report were the result of the leagues’ willingness to provide some injury
data upon request. While it is commendable that the leagues occasionally provide the data when requested, this does
not entirely address the concerns outlined in Recommendation 1.
612
Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations, Recommendation 17:1-B (2016).
613
See The Datalys Center for Sports Injury Research and Prevention, NCAA, http://www.ncaa.org/health-and-
safety/medical-conditions/datalys-center-sports-injury-research-and-prevention (last visited Aug. 3, 2016), archived at
https://perma.cc/2M75-B24L.
614
See, e.g., Data transparency, GlaxoSmithKline, http://www.gsk.com/en-gb/behind-the-science/innovation/data-
transparency (last visited June 20, 2016), archived at https://perma.cc/M5HN-NLHN; Frequently Asked Questions,
the YODA Project, http://yoda.yale.edu/frequently-asked-questions-faqs#Data (last visited June 20, 2016), archived
at https://perma.cc/2Z98-R7HC.
615
This recommendation also appears as Recommendation 7:1-E in our Report Protecting and Promoting the Health
of NFL Players: Legal and Ethical Analysis and Recommendations. Due to the fact that the recommendation was
inspired by MLB’s concussion-specific DL list, we include it here as well.
616
See Paul McCrory et al., Consensus statement on concussion in sport: the 4th Int’l Conference on Concussion in
Sport held in Zurich, November 2012, 47 Br. J. Sports Med. 250, 251 (2013).
617
Id. at 253.

!
249!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
618
2012 MLB CBA, Att. 36, ¶ 2.
619
See Paul McCrory et al., Consensus statement on concussion in sport: the 4th Int’l Conference on Concussion in
Sport held in Zurich, November 2012, 47 Br. J. Sports Med. 250, 250–58 (2013) (discussing the challenges of and
best practices for diagnosing concussions).
620
See id.
621
See id. at 252-58 (discussing generally the challenges of determining when an athlete has recovered from a
concussion).
622
We recognize that this new injured reserve list is subject to gaming by clubs, whereby a club might designate a
player as concussed in order to add another player and effectively expand the roster. We do not view this this
concern to be sufficient to outweigh the health benefits of the proposal. Moreover, all injury lists are subject to some
risk of being gamed in this manner, and thus the issue is not unique to what we propose.
623
Letter from Larry Ferazani, NFL, to authors (July 18, 2016).
624
Id.
625
Mike Florio, NFL tells teams to stop commenting about concussed players, ProFootballTalk (Nov. 11, 2016, 7:50
PM), http://profootballtalk.nbcsports.com/2016/11/11/nfl-tells-teams-to-stop-commenting-about-concussed-players/,
archived at https://perma.cc/Z7ML-ZP7W.
626
Id.
627
Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations Recommendation 7:4-B (2016).
628
Mike Florio, Disclosure of injury information continues to put NFL players in a delicate spot, ProFootballTalk (July
10, 2015, 12:34 PM), http://profootballtalk.nbcsports.com/2015/07/10/disclosure-of-injury-information-continues-to-
put-nfl-players-in-a-delicate-spot/, archived at http://perma.cc/PYL4-KMRY (“many players would like to keep [injury
information] secret, in order to keep an opponent from hitting, poking, and/or kicking the injured region.”)
629
By “education-related benefits,” we mean programs that assist players to obtain or complete their college degree,
or to obtain training for a second career.
630
Many experts have recognized that “financial insecurity can cause people to ‘cut corners in ways that may affect
their health and well-being,’ like spending less on food, clothing, or prescriptions.” Nadia N. Sawicki, Modernizing
Informed Consent: Expanding the Boundaries of Materiality, Univ. Ill. L. Rev. (2016), citing Kevin R. Riggs and Peter
A. Ubel, Overcoming Barriers to Discussing Out-of-Pocket Costs With Patients, 174 Jama Int. Med. 849 (2014); Peter
A. Ubel, Amy P. Abernethy, and S. Yousuf Zafar, Full Disclosure—Out-of-Pocket Costs as Side Effects, 369 New
Eng. J. Med. 1484 (2013). Indeed, to many, “financial well-being is certainly within the boundaries of most peoples’
concept of health.” Id., quoting Michael S. Wilkes and David L. Schriger, Caution: The Meter is Running: Informing
Patients About Health Care Costs, 165 Western J. Med 74, 78 (1996) (noting that “discussions about the cost of care
are an important part of the physician-patient relationship”).
631
See Thomas Richardson et al., The relationship between personal unsecured debt and mental and physical
health: A systematic review and meta-analysis, 33 Clinical Psychol. Rev. 8, 1148-62 (2013).
632
Based on an average career length of approximately three years, the NFLPA has estimated that the average
career earnings of an NFL player are $4 million after taxes. See Adam Molon, Why So Many Ex-NFL Players
Struggle With Money, CNBC (Jan. 31, 2014, 12:29 PM), www.cnbc.com/id/101377457#, archived at
http://perma.cc/F5YN-FJE2. Using an average salary of $1.9 million and an average career length of 3.5 years,
others have estimated NFL players earn about $6.7 million in their careers, a figure largely on par with that of the
NFLPA’s. See Nick Schwartz, The Average Career Earnings Of Athletes Across America’s Major Sports Will Shock
You, USA Today, Oct. 24, 2013, http://ftw.usatoday.com/2013/10/average-career-earnings-nfl-nba-mlb-nhl-mls,
archived at http://perma.cc/9DFP-WPQ2. However, the NFL has disputed the 3.5 years figure generally provided by
the NFLPA, stating instead that players who actually make an NFL club have, on average, careers of about 6 years.
See What is average NFL player’s career length? Longer than you might think, Commissioner Goodell says, NFL
(Apr. 18, 2011), http://nflcommunications.com/2011/04/18/what-is-average-nfl-player%E2%80%99s-career-length-
longer-than-you-might-think-commissioner-goodell-says/, archived at http://perma.cc/PX5U-9SFK. Finally, it is
important to point out that the average in this case does not reflect the median career earnings of NFL players, i.e.,
the career earnings of your typical NFL player—the calculation of which would depend on how you define the typical
player.
633
Pablo S. Torre, How (and Why) Athletes Go Broke, Sports Illustrated, Mar. 23, 2009,
http://www.si.com/vault/2009/03/23/105789480/how-and-why-athletes-go-broke, archived at http://perma.cc/7KVD-
QA72.
634
David R. Weir, et al., National Football League Player Care Foundation Study of Retired NFL Players 37, Inst. for
Social Res. at Univ. of Mich. (2009), http://ns.umich.edu/Releases/2009/Sep09/FinalReport.pdf, archived at
http://perma.cc/WY8A-HZ8Z.
635
Kyle Carlson, et al., Bankruptcy Rates Among NFL Players with Short-Lived Income Spikes 8, Nat’l Bureau of
Economic Res. (April 2015), http://www.nber.org/papers/w21085.pdf, archived at http://perma.cc/Y8A5-NJLZ. The
study found that the rate of bankruptcy among the general population in the 25–34 year age group was very similar to

!
250!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
the bankruptcy rate of NFL players. However, the general population’s average income is almost certainly
substantially less than that of the average NFL player.
636
Linda Holmes, ESPN’s ‘Broke’ Looks At The Many Ways Athletes Lose Their Money, NPR (Oct. 2, 2012, 1:35
PM), http://www.npr.org/blogs/monkeysee/2012/10/02/162162226/espns-broke-looks-at-the-many-ways-athletes-
lose-their-money, archived at https://perma.cc/VPK7-QLBX.
637
See Jim Baumbach, Life After Football, Newsday, Jan. 22, 2015,
http://data.newsday.com/projects/sports/football/life-football/, archived at http://perma.cc/77DP-LUUE.
638
Pablo S. Torre, How (and Why) Athletes Go Broke, Sports Illustrated, Mar. 23, 2009,
http://www.si.com/vault/2009/03/23/105789480/how-and-why-athletes-go-broke, archived at http://perma.cc/7KVD-
QA72.
639
See Ken Belson, When Settlement Buys Time, N.Y. Times, Jul. 19, 2014,
http://www.nytimes.com/2014/07/19/sports/football/former-nfl-players-make-difficult-choice-in-opposing-concussion-
settlement.html, archived at http://perma.cc/5P3D-94A8; Sally Jenkins and Rick Maese, Do No Harm: Who Should
Bear The Costs Of Retired NFL Players’ Medical Bills? Wash. Post, May 9, 2013,
http://www.washingtonpost.com/sports/redskins/do-no-harm-who-should-bear-the-costs-of-retired-nfl-players-
medical-bills/2013/05/09/2dae88ba-b70e-11e2-b568-6917f6ac6d9d_story.html, archived at http://perma.cc/VER2-
EM24.
640
See, e.g., Melissa B. Jacoby, Teresa A. Sullivan, Elizabeth Warren, Rethinking the Debates over Health Care
Financing: Evidence from the Bankruptcy Courts, 76 N.Y.U. L. Rev. 375 (2001) (empirical data demonstrating how
many American families declare bankruptcy in the aftermath of illness or other healthcare crisis); Christopher Tarver
Robertson, Richard Egelhof, Michael Hoke, Get Sick, Get Out: The Medical Causes of Home Mortgage Foreclosures,
18 Health Matrix 65 (2008) (empirically demonstrating and discussing the role that health crises have in home
foreclosures).
641
Gabe Feldman, Closing the Floodgates: The Battle Over Workers’ Compensation Rights in California, 8 FIU L.
Rev. 107, 109 (2012).
642
Lex Larson, Workers’ Compensation Law, § 1.01 (Matthew Bender 2014).
643
Lex Larson, Workers’ Compensation Law, § 1.03 (Matthew Bender 2014).
644
Howard Berkes, Injured Workers Suffer As ‘Reforms’ Limit Workers’ Compensation Benefits, Nat’l Pub. Radio,
Mar. 4, 2015, http://www.npr.org/2015/03/04/390441655/injured-workers-suffer-as-reforms-limit-workers-
compensation-benefits, archived at https://perma.cc/6MB8-56Y4 (discussing states’ reductions in maximum workers’
compensation benefits).
645
See, e.g. 2011 NFL CBA, Art. 41, § 4.
646
See, e g., 2011 CBA, App. A, ¶ 9.
647
With the assistance of the NFLPA, we were able to gain access to lengthy summaries of NFL plan documents.
648
These programs can be found at the NFL’s Player Engagement Department website at
https://www.nflplayerengagement.com.
649
See NFLPA Externship Program Enters Second Year, Nat’l Football League Players Ass’n, Feb. 23, 2015,
https://nflpa.com/news/all-news/nflpa-externship-program-enters-second-year, archived at https://perma.cc/AZX7-
G8AY; Active Players – Grow Experience, Nat’l Football League Players Ass’n, https://nflpa.com/active-
players/playerdevelopment/experience (last visited Apr. 7, 2015), archived at https://perma.cc/AZX7-G8AY; A
Winning Team: Kelley School of Business and the NFLPA, Kelley Sch. of Bus.,
https://nflpawebqa.blob.core.windows.net/media/Default/PDFs/Player%20Development/NFLPA-
Kelley_%20Program.pdf (last visited Apr. 7, 2015), archived at https://perma.cc/E4UJ-N6CT.
650
These programs are discussed in Appendices D and E of our Report, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations.
651
See Bert Bell/Pete Rozelle NFL Player Retirement Plan (Apr. 1, 2012) § 1.11 (defining “Credited Season“); 2011
CBA, Art. 26, § 2 (same).
652
2011 CBA, Art. 12, § 6(c)(i).
653
2011 CBA, Art. 1.
654
2011 CBA, Art. 12, § 2.
655
2011 CBA, Art. 12, § 6(c)(v).
656
The summary provided in this Section comes from reviewing a Summary Plan Description for the Severance Pay
Plan prepared for NFL players by the NFL Management Council, the administrators of the Severance Pay Plan.
657
Pursuant to the terms of the 2006 CBA, the NFL was not required to fund several benefit plans, including the
Severance Pay Plan, in 2010 if the 2010 season was not played with a Salary Cap—a situation that would only exist
if the NFL and NFLPA were unable to agree to an extension of the CBA, which is what actually transpired. See 2006
CBA, Art. L; Art. LVI. These provisions were included as “poison pills,” designed to encourage the NFL and NFLPA to
agree to a new CBA before the prior version expired.
658
The summary provided in this Section comes from reviewing a Summary Plan Description for the Bert Bell/Pete
Rozelle NFL Player Retirement Plan (“Retirement Plan”) prepared for NFL players by the Retirement Board, the
administrators of the Retirement Plan.

!
251!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
659
Aaron Gordon, Battle for Benefits, Part 3: “Don’t Make Proud Men Beg”, Vice Sports (Sept. 18, 2015),
https://sports.vice.com/en_us/article/battle-for-benefits-part-3-dont-make-proud-men-beg, archived at
https://perma.cc/YP4J-8AGY.
660
Id.
661
See Mark Fainaru & Steve Fainaru, League of Denial: The NFL, Concussions, and the Battle for Truth 86–87
(2013).
662
Pursuant to the Employee Retirement Income Security Act (“ERISA”), individuals claiming entitlement to benefits
under a retirement plan are entitled to bring a civil action to enforce or clarify their rights under the plan. 29 U.S.C. §
1132(a). Former players routinely sue the Retirement Plan alleging they were wrongfully denied benefits, with mixed
success. See, e.g., Atkins v. Bert Bell/Pete Rozelle NFL Player Retirement Plan, 694 F.3d 557 (5th Cir. 2012) (plan
administrator’s determination that player was not entitled to additional benefits was not an abuse of discretion); Giles
v. Bert Bell/Pete Rozelle NFL Player Retirement Plan, 925 F. Supp. 2d 700 (D.Md. 2012) (Retirement Board’s
classification of participant’s disability as “Inactive” rather than “Football Degenerative” was not reasonable decision
supported by substantial evidence in the record); Moore v. Bert Bell/Pete Rozelle NFL Player Retirement Plan, 282
Fed.Appx. 599 (9th Cir. 2008) (Retirement Board’s decision to terminate player’s benefits was not based on
reasonable interpretation of plan’s terms); Johnson v. Bert Bell/Pete Rozelle NFL Player Retirement Plan, 468 F.3d
1082 (8th Cir. 2006) (plan administrator did not abuse its discretion in setting date of disability as time of disability
determination by physician to whom plan had referred former player); Boyd v. Bert Bell/Pete Rozelle NFL Players
Retirement Plan, 410 F.3d 1173 (9th Cir. 2005) (administrator did not abuse its discretion in rejecting retiree’s claim,
given ambiguity as to cause of neurologic disability at issue); Courson v. Bert Bell NFL Player Retirement Plan, 75 F.
Supp. 2d 424 (W.D.Pa. 1999) aff’d 214 F.3d 136 (3d Cir. 2000) (plan administrator’s determination that former player
was not disabled was not arbitrary or capricious); Brumm v. Bert Bell NFL Retirement Plan, 995 F.2d 1433 (8th Cir.
1993) (trustees’ interpretation of ERISA plan to allow higher level of disability benefits only in cases involving single,
identifiable football injury, and excluding cases of disability resulting from football career’s overall impact on body,
was unreasonable in light of plan’s goals).
663
Oversight of the Nat’l Football League (NFL) Retirement System: Hearing Before the Comm. On Commerce, Sci.
& Transp., 110th Cong. 1177 (2007), available at http://www.gpo.gov/fdsys/pkg/CHRG-110shrg76327/html/CHRG-
110shrg76327.htm, archived at https://perma.cc/RK38-GBYQ?type=pdf.
664
Aaron Gordon, Battle for Benefits, Part 3: “Don’t Make Proud Men Beg”, Vice Sports (Sept. 18, 2015),
https://sports.vice.com/en_us/article/battle-for-benefits-part-3-dont-make-proud-men-beg, archived at
https://perma.cc/YP4J-8AGY.
665
Id.
666
The summary provided in this Section comes from reviewing a Summary Plan Description for the Player Annuity
Plan prepared for NFL players by the Annuity Board, the administrators of the Player Annuity Plan.
667
An annuity plan is one in which a person contributes money to an investment account and then, at a later date
(typically in retirement), the account makes regular payments to the person. Definition of Annuity, Investopedia,
http://www.investopedia.com/terms/a/annuity.asp (last visited Sep. 18, 2015), archived at http://perma.cc/CV69-
CQC7.
668
See IRS Announces 2016 Pension Plan Limitations; 401(k) Contribution Limit Remains Unchanged at $18,000 for
2016, Internal Revenue Service, Oct. 21, 2015, https://www.irs.gov/uac/Newsroom/IRS-Announces-2016-Pension-
Plan-Limitations%3B-401(k)-Contribution-Limit-Remains-Unchanged-at-$18,000-for-2016, archived at
https://perma.cc/G28S-9K6R.
669
“Vest” means “[t]o give (a person) an immediate, fixed right of present or future enjoyment.” BLACK’S LAW
DICTIONARY (9th ed. 2009). In essence, “vesting” in a benefit or retirement plan generally means the individual has
earned the right to the benefit or retirement plan, typically by meeting a minimum number of years of employment.
670
The summary provided in this Section comes from reviewing a Summary Plan Description for the Second Career
Savings Plan prepared for NFL players by the Savings Board, the administrators of the Second Career Savings Plan.
671
A 401(k) is a retirement plan provided for in Section 401(k) of the Internal Revenue Code 26 U.S.C. § 401(k).
Under a 401(k), employees contribute a certain percentage of their salary to an investment account before taxes are
withheld from the salary. Taxes on the income are deferred until the employee withdraws money from the 401(k)
account, which is generally not permitted until the employee reaches age 59½. An additional benefit of 401(k) plans is
that often times employers contribute to the accounts and these contributions are also tax-deferred. See 401k Plans,
Internal Revenue Service, http://www.irs.gov/Retirement-Plans/401k-Plans (last visited Sep. 18, 2015), archived at
http://perma.cc/DN7N-WVKS.
672
The Summary Plan Description for the Second Career Savings Plan does not specify whether a player who is
employed by a club as a coach or in some other capacity is not eligible for the benefits at 45.
673
Quotes from NFLPA Press Conference, Nat’l Football League Players Ass’n (Feb. 4, 2016),
https://www.nflpa.com/news/all-news/quotes-from-nflpa-sb50-press-conference, archived at https://perma.cc/2GZH-
FQ37.
674
The summary provided in this Section comes from reviewing a Summary Plan Description for the Player Insurance
Plan prepared for NFL players by Aon Hewitt, the administrators of the Player Insurance Plan.

!
252!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
675
COBRA, 29 U.S.C. §§ 1161–69, requires continuation coverage to be offered to covered employees, their
spouses, former spouses, and dependent children when group health coverage would otherwise be lost due to
certain specific events, including, as would be relevant in the NFL, “the termination (other than by reason of such
employee’s gross misconduct), or reduction of hours, of the covered employee’s employment.” 29 U.S.C. § 1163(2).
676
The summary provided in this Section comes from reviewing a Summary Plan Description for Health
Reimbursement Account Plan prepared for NFL players by the HRA Board, the administrators of the Health
Reimbursement Account Plan.
677
Upon the player’s death, the player’s spouse and dependents can continue to utilize the HRA Plan until the
account is exhausted or they die.
678
For comparison, according to the U.S. Department of Health and Human Services, the average cost of long-term
care in a semi-private room in a nursing home is $205 per day, and $229 per day for a private room. Costs of Care,
U.S. Dep’t of Health and Human Services (last visited Aug. 25, 2016), http://longtermcare.gov/costs-how-to-
pay/costs-of-care, archived at https://perma.cc/RZ4N-BFHB.
679
The summary provided in this Section comes from reviewing a Summary Plan Description for the Former Player
Life Improvement Plan prepared for NFL players by Aon Hewitt, the administrators of the Former Player Life
Improvement Plan.
680
The summary provided in this Section comes from reviewing the NFL Player Disability & Neurocognitive Benefit
Plan.
681
The Initial Claims Committee consists of three members: one appointed by the NFL; one appointed by the NFLPA;
and, a medical professional jointly chosen by the parties.
682
The Disability Board consists of three members selected by the NFL and three members selected by the NFLPA.
683
League football activities include any NFL “pre-season, regular-season, or post-season game, or any combination
thereof, our out of League football activity supervised by a[] [Club], including all required or directed activities.”
684
Edgeworth Economics, DRAFT Dangers of the Game: Injuries in the NFL – Analysis for the NFLPA (Sept. 6,
2010), http://esq.h-cdn.co/assets/cm/15/07/54dae83730ce3_-_Dangers-of-the-Game-Draft-Esquire.pdf, archived at
http://perma.cc/T3MH-YTVU.
685
Id.
686
Id.
687
Id.
688
Id.
689
The summary provided in this Section comes from reviewing a Summary Plan Description for the 88 Plan
prepared for NFL players by the 88 Board, the administrators of the 88 Plan.
690
2011 CBA, Art. 41, § 1.
691
See 2011 CBA, Art. 41, § 3 (identifying Florida as a state that does not require workers’ compensation coverage).
692
For more on the role of workers’ compensation in the NFL, see Christopher R. Deubert, I. Glenn Cohen, Holly
Fernandez Lynch, Protecting and Promoting the Health of NFL Players: Legal and Ethical Analysis and
Recommendations, § 8(B) (2016).
693
According to the College Board, the average tuition at a public four-year university for an in-state student is
$9,410; the average tuition at a public four-year university for an out-of-state student is $23,893; and, the average
tuition at a private four-year university is $32,405. See Average Published Undergraduate Charges by Sector, 2015-
16, CollegeBoard, http://trends.collegeboard.org/college-pricing/figures-tables/average-published-undergraduate-
charges-sector-2015-16 (last visited Mar. 17, 2016), archived at https://perma.cc/HNW6-FBKG.
694
2011 CBA, Art. 50, § 1(a).
695
1977 CBA, Art. XI.
696
2011 CBA, Art. 50, § 1(d). “Within 60 days of the initiation of an investigation, two or more neutral physicians will
be selected to investigate and report to the Joint Committee on the situation. The neutral physicians shall issue a
written report within 60 days of their selection, and their recommendations as to what steps shall be taken to address
and correct any issues shall be acted upon by the Joint Committee.” Id.
697
In Stringer v. Nat’l Football League, the Court also expressed concerns about the effectiveness of the Joint
Committee: “While the NFL is required to give ‘serious and thorough consideration’ to recommendations of the Joint
Committee, the CBA imposes no independent duty on the NFL to consider health risks arising from adverse playing
conditions, or to make recommendations for rules, regulations or guidelines for the Clubs to follow.” 474 F. Supp.2d
894, 906 (S.D. Ohio 2007).
698
This information was provided by the NFLPA.
699
Id.
700
2011 CBA, Art. 39, § 3(a).
701
Id.
702
The three NFL-appointed members of the ACC are: Dr. Matthew Matava, club doctor for the St. Louis Rams and
President of the NFL Physicians Society (“NFLPS”); Rick Burkholder, athletic trainer for the Kansas City Chiefs and
President of the Professional Football Athletic Trainers (“PFATS”); and, Dr. Elliott Hershman, Chairman of NFL Injury
and Safety Panel, Department of Orthopaedic Surgery, Lenox Hill Hospital, and Team Orthopedist, New York Jets.

!
253!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
The three NFLPA-appointed members of the ACC are: Dr. Anthony Alessi, neurologist and Associate Clinical
Professor of Neurology, University of Connecticut; Dr. Ross McKinney, Director, Trent Center for Bioethics,
Humanities & History of Medicine, Duke University & School of Medicine; and, Dr. Johnny Benjamin, orthopedist and
Director, Pro Spine Center.
703
The Benefit Plan can be found as an exhibit in a lawsuit brought by the widow of former MLB pitcher Jose Lima.
See Lima-Leclerc v. Major League Baseball Players Benefit Plan, 13-cv-271 (S.D.N.Y.), ECF No. 11-5.
704
Although there is one Canadian MLB club (Toronto Blue Jays), the Benefit Plan does not include any special
provisions for providing benefits under Canadian law.
705
Id. § 7.2.
706
!MLBPA, MLB Announce Details of New Labor Agreement, MLBPA (Dec. 2, 2016),
http://www.mlbplayers.com/ViewArticle.dbml?DB_OEM_ID=34000&ATCLID=211336390, archived at
https://perma.cc/4XUA-2DAW.!
707
See Benefit Plan at Tables 1–9.
708
Id. § 7.12–13. See also id. at Tables 1–9. U.S. Department of Treasury Regulations cap maximum annual player
benefits at $200,000. Id. § 9.1.
709
See id.
710
Id. § 27.62.
711
Id.
712
See id. (defining a “Vested Member”); id. § 27.37 (defining “Normal Retirement Date”).
713
Id.
714
See Benefit Plan at Tables 1–9 (“For fractional years of credited service, benefits shall be determined by
interpolation.”)
715
Benefit Plan § 6.1.
716
Id. § 7.6(b).
717
IRS Announces 2016 Pension Plan Limitations, Internal Revenue Service, Oct. 21, 2015,
https://www.irs.gov/uac/newsroom/irs-announces-2016-pension-plan-limitations-401-k-contribution-limit-remains-
unchanged-at-18-000-for-2016, archived at https://perma.cc/8AQV-YZN8.
718
Benefit Plan § 8.1. In 2016, the maximum amount an employee could contribute to a 401(k) plan was $18,000.
IRS Announces 2015 Pension Plan Limitations, Internal Revenue Service, Oct. 23, 2014,
http://www.irs.gov/uac/Newsroom/IRS-Announces-2015-Pension-Plan-Limitations-1, archived at
http://perma.cc/4DFY-BQAL.
719
Benefit Plan § 8(g).
720
See id. § 8.1(b)(i) (permitting clubs to make contributions “in their discretion”).
721
MLB Comments and Corrections (Sept. 30, 2016).
722
Benefit Plan § 8.5.
723
! MLBPA, MLB Announce Details of New Labor Agreement, MLBPA (Dec. 2, 2016),
http://www.mlbplayers.com/ViewArticle.dbml?DB_OEM_ID=34000&ATCLID=211336390, archived at
https://perma.cc/4XUA-2DAW.!
724
Benefit Plan § 13.2(a)(i)–(iv).
725
Id. § 13.2(a)(iv).
726
Id. §§ 13.3, 13.4(a). Players are entitled to extend their healthcare coverage under the inactive health benefits
program until they are eligible for Medicare at age 65. Id. § 13.4(d).
727
MLB Comments and Corrections (Mar. 15, 2017).
728
!Id.!
729
Benefit Plan §§ 14.3–14.8.
730
! MLBPA, MLB Announce Details of New Labor Agreement, MLBPA (Dec. 2, 2016),
http://www.mlbplayers.com/ViewArticle.dbml?DB_OEM_ID=34000&ATCLID=211336390, archived at
https://perma.cc/4XUA-2DAW.!
731
Benefit Plan § 10.1.
732
Id. § 10.2(a). If the player was not injured as an active member or within five years of becoming inactive—or if the
player cannot prove by clear and convincing evidence that his disability is the result of his active services—he may
still receive disability benefits equal to one-twelfth of his total income from employment or self-employment during the
year preceding his disability (capped at a high of $5,000 and a low of $2,500) if he is otherwise eligible. Id.
733
Id. § 10.3(b).
734
See 2012 MLB CBA, Art. IX, § E (entitling player to receive unpaid balance of salary if contract was terminated
after injury “less all workers’ compensation payments received by the Player”); Art. XXIII, § D(1)(g) (including medical
“costs reimbursed or paid for through workers’ compensation” as part of the definition for Player Benefit Costs).
735
As discussed in the Introduction to this Section, the normal trade-off for workers’ compensation benefits is that the
injured employee cannot sue the employer for injuries suffered in the course of employment. Even though Florida
players do not receive workers’ compensation benefits, they likely still cannot sue the club. The CBA also presents a

!
254!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
potential obstacle against any such claim. Common law claims such as negligence are generally preempted by the
Labor Management Relations Act (“LMRA”). 29 U.S.C. § 185. The LMRA bars or “preempts” state common law
claims where the claim is “substantially dependent upon analysis of the terms” of a CBA, i.e., where the claim is
“inextricably intertwined with consideration of the terms of the” CBA.” Allis-Chambers Corp. v. Lueck, 471 U.S. 202,
213 (1985). In order to assess a club’s duty to a player—an essential element of a negligence claim—the Court may
have to refer to and analyze the terms of the CBA, resulting in the claim’s preemption. So long as the player’s claim is
“inextricably intertwined” with the CBA, it will be preempted. Instead, such claims are intended to be brought pursuant
to the arbitration provisions in the CBA.
736
2012 MLB CBA, Art. XV, § D.
737
! MLBPA, MLB Announce Details of New Labor Agreement, MLBPA (Dec. 2, 2016),
http://www.mlbplayers.com/ViewArticle.dbml?DB_OEM_ID=34000&ATCLID=211336390, archived at
https://perma.cc/4XUA-2DAW.!
738
2012 MLB CBA, Art. XIII, § A(1).
739
2012 MLB CBA, Art. XIII, § A(3).
740
2012 MLB CBA, Art. XIII, § A(4). Nevertheless, the SHAC does not appear to have completed any serious
investigations, other than looking into a rise in broken bats in 2008. Major League Baseball, MLB, MLBPA Adopt
Recommendations of Safety and Health Advisory Committee, Major League Baseball (Dec. 9, 2008), available at
http://mlb.mlb.com/pa/pdf/health_advisory_120908.pdf, archived at https://perma.cc/QN49-XDBJ.
741
See 2017 NBA CBA, Art. VII, § 2(a) (explaining that the Salary Cap, i.e., the amounts available to players in the
form of salary, is reduced by the amount spent on player benefits).
742
The NBA CBA also provides that players employed by the Toronto Raptors are required to receive comparable
benefits as those described in this Section as permitted under Canadian Law.
743
See Sonya Stinson, Go Long: Retirement Plans for Pro Athletes, Fox Bus., http://www.foxbusiness.com/personal-
finance/2012/09/25/go-long-retirement-plans-for-pro-athletes/, Sep. 25, 2012, archived at http://perma.cc/TR69-
SG8Z; Ron Kroichick, Pensions in Pro Sports: NBA All-Star break brought big boost to Ezersky, S.F. Chron., Mar. 18,
2007, http://www.sfgate.com/sports/kroichick/article/PENSIONS-IN-PRO-SPORTS-NBA-All-Star-break-2609494.php,
archived at https://perma.cc/9JTS-W7S6. “‘Years of Service’ means the number of years of NBA service credited to a
player in accordance with the following: a player will be credited with one (1) year of NBA service for each year that
he is on an NBA Active List or Inactive List for one (1) or more days during the Regular Season.” 2017 NBA CBA, Art.
I, § 1(iiii).
744
See Scott Soshnick, NBA Players Forced to Save Toward Retirement for First Time, Bloomberg Bus., Jul. 12,
2012, http://www.bloomberg.com/news/articles/2012-07-12/nba-players-forced-to-save-toward-retirement-for-first-
time, archived at http://perma.cc/EV83-V42Z (mentioning that NBA players can begin receiving their pension at 45).
745
2017 NBA, CBA Art. IV, § 1(a)(1).
746
2017 NBA, CBA Art. IV, § 1(a)(2).
747
2017 NBA CBA, Art. IV, § 1(c).
748
IRS Announces 2015 Pension Plan Limitations, Internal Revenue Service, Oct. 23, 2014,
http://www.irs.gov/uac/Newsroom/IRS-Announces-2015-Pension-Plan-Limitations-1, archived at
http://perma.cc/4DFY-BQAL.
749
2017 NBA, CBA, Art. IV, § 2.
750
See Jay MacDonald, Professional Athletes’ Big-League Tax Bills, Fox Bus., Mar. 15, 2012,
http://www.foxbusiness.com/personal-finance/2012/03/15/professional-athletes-big-league-tax-bills/, archived at
http://perma.cc/2WDF-RULG; Mark Riddix, Top Pro Athlete Pension Plans, Investopedia, July 16, 2010,
http://www.investopedia.com/financial-edge/0710/top-pro-athlete-pension-plans.aspx, archived at
http://perma.cc/SR8A-HV72. See also Top 15 Sports Organizations with the Best 401k Plans, BrightScope, Jun. 25,
2013, http://blog.brightscope.com/2013/06/25/top-15-sports-organizations-with-the-best-401k-plans/, archived at
http://perma.cc/XKT4-NNDZ (rating the plan as the best in professional sports, in part because of generous
contributions of NBA clubs).
751
2017 NBA CBA, Art. IV § 4(a).
752
!2017!NBA!CBA,!Art.!IV,!§!4(d)(1).!
753
Basketball Related Income, generally speaking, “means the aggregate operating revenues” of the NBA and NBA
clubs. 2017 NBA CBA, Art. VII, § 1(a)(1).!
754
This information was provided by the NBA.
755
See 2011 NBA CBA, Art. IV, § 4(b)(3).
756
Id.
757
Voluntary Employee Beneficiary Association - 501(c)(9), Internal Revenue Service, Jan. 13, 2015,
http://www.irs.gov/Charities-&-Non-Profits/Other-Non-Profits/Voluntary-Employee-Beneficiary-Association-
501%28c%29%289%29, archived at http://perma.cc/XGW2-WXEK. The VEBA is funded through 1% of Basketball
Related Income. 2011 NBA CBA Art. IV § 4(c).
758
2017 NBA CBA, Art. IV, § 3(a)(9).

!
255!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
759
2017 NBA CBA, Art. IV, § 3(a).
760
2017 NBA CBA, Art. IV, § 3(a)(9).
761
NBPA-NBA Supplemental Benefit Plan, CitizenAudit, July 2014, http://pdfs.citizenaudit.org/2014_07_EO/20-
1260597_990O_201306.pdf, archived at http://perma.cc/EG2S-XXCL.
762
Id.
763
See 2011 NBA CBA, Art. IV, § 3(b).
764
The CBA does not define what it means to be a “resident” of Canada.
765
2017 NBA CBA, Art. IV, § 3(a)(6)(i).
766
Current NBA Players Break New Ground by Choosing to Fund Health Insurance for Retired NBA Players, Nat’l
Basketball Players Ass’n (July 27, 2016), available at http://nbpa.com/current-nba-players-break-new-ground-by-
choosing-to-fund-health-insurance-for-retired-nba-players/, archived at https://perma.cc/4UKC-6KUU.
767
!This!information!was!provided!by!the!NBA.!
768
2017 NBA CBA, Art. IV § 3(a)(2)(ii).
769
2017 NBA CBA, Art. IV, § 6(a).
770
2017 NBA CBA, Art. IV, § 3(a)(7).
771
Id.
772
2017 NBA CBA, Art. IV, § 5(b).
773
Id.
774
2011 NBA CBA, Art. XXII § 2.
775
2011 NBA CBA, Art. XXII § 8.
776
!2017!NBA!CBA,!Art.!XXII,!§!9(b).!
777
In reviewing a draft of this Report, the NBA also highlighted that it and the NBPA have a Wearables Committee for
the purpose of reviewing and approving wearable devices for use by players. 2017 NBA CBA, Art. XXII, § 13. We
know from our research that the NFL and NFLPA have also collaborated on this issue. It is possible other leagues too
have also considered this issue. However, because it is a rapidly evolving issue with questionable ties to player
health, we have not endeavored to cover this issue across the leagues and thus do not include additional information
here. For more information on potential legal concerns with wearable technologies, see our law review article,
Jessica L. Roberts, et al., Evaluating NFL Player Health and Performance: Legal and Ethical Issues, 165 U. Penn. L.
Rev. 227 (2017).
778
2011 NBA CBA, Art. XXXIII, § 2 (d)(i).
779
2011 NBA CBA, Art. XXXIII, § 2 (d)(ii).
780
See 2013 NHL CBA, § 50.4(a)-(b) (explaining that “Players’ Share” of league revenues is equal to the clubs’
aggregate salaries plus player benefits).
781
“Actuarial equivalence” is a “[g]eneral term used for applying some measurement to two benefit plans to see if
resulting values are sufficiently close for the specified purpose.” John M. Bertko and Cori E. Uccello, Comparing
Health Benefit Plans: Demystifying “Actuarial Equivalence,” Am. Acad. of Actuaries, Jun. 11, 2008,
http://www.actuary.org/briefings/pdf/equivalence2_july08.pdf, archived at http://perma.cc/23VS-LBLP.
782
2013 NHL CBA, § 21.15.
783
2013 NHL CBA, § 21.13.
784
A player earned “credited service” for each regular season game he is on the club’s roster. 2013 NHL CBA, §
21.14.
785
Id. Additionally, a player who has five years of credited service is eligible, upon becoming totally and permanently
disabled, to receive pension benefits under the Retirement Plan equal to “the value of his accrued pension benefits,
actuarially reduced to the age of commencement.” 2013 NHL CBA, Art. 21, § 18.
786
2013 NHL CBA, § 21.11(a)(i).
787
See IRS Announces 2016 Pension Plan Limitations; 401(k) Contribution Limit Remains Unchanged at $18,000 for
2016, Internal Revenue Service, Oct. 21, 2015, https://www.irs.gov/uac/Newsroom/IRS-Announces-2016-Pension-
Plan-Limitations%3B-401(k)-Contribution-Limit-Remains-Unchanged-at-$18,000-for-2016, archived at
https://perma.cc/G28S-9K6R.
788
2013 NHL CBA, § 21.16.
789
Senior Retired Players Fund Increased, Nat’l Hockey League Player Ass’n, Jul. 31, 2013,
www.nhlpa.com/news/senior-retired-players-fund-increased, archived at http://perma.cc/YYD8-KZCQ.
790
Id.
791
Id.
792
See IRS Announces 2016 Pension Plan Limitations; 401(k) Contribution Limit Remains Unchanged at $18,000 for
2016, Internal Revenue Service, Oct. 21, 2015, https://www.irs.gov/uac/Newsroom/IRS-Announces-2016-Pension-
Plan-Limitations%3B-401(k)-Contribution-Limit-Remains-Unchanged-at-$18,000-for-2016, archived at
https://perma.cc/G28S-9K6R.
793
2013 NHL CBA, § 23.2.
794
2013 NHL CBA, § 23.6(a).

!
256!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
795
See 2013 NHL CBA, § 23.6(d).
796
2013 NHL CBA, § 23.7(b).
797
2013 NHL CBA, § 21.18.
798
2013 NHL CBA, § 23.3(a).
799
2013 NHL CBA, § 23.3(d).
800
2013 NHL CBA, § 23.3(b).
801
See 2013 NHL CBA, § 23.3(a) (limiting career ending disability benefits to “a Player who is on a Club’s Insured
Roster”); § 23.3(b) (limiting serious disability benefits to “a Player who is on a Club’s Insured Roster”).
802
2013 NHL CBA, § 31.5.
803
2013 NHL CBA, § 31(5).
804
2013 NHL CBA, Art. 29.
805
Rick Westhead, NHLPA readies $3M ‘back to school’ program, TSN, Jun. 9, 2015, www.tsn.ca/nhlpa-readies-3m-
back-to-school-program-1.303734, archived at http://perma.cc/G6BQ-WGSL.
806
Id.
807
2013 NHL CBA, § 34.9(b).
808
2013 NHL CBA, § 34.9(a).
809
2013 NHL CBA, § 34.9(e).
810
2013 NHL CBA, § 34.1(c).
811
2013 NHL CBA, § 34.3(b)(i).
812
2013 NHL CBA, § 34.4(a).
813
2014 CFL CBA, § 13.02.
814
Id.
815
Id.
816
The relationship between the CFL’s medical plan and the Canadian healthcare system, under which the
government pays for the majority of healthcare expenses, is unclear. The Canadian healthcare system is described
in more detail in Chapter 1: Club Medical Personnel.
817
2014 CFL CBA, Art. 16.
818
Id.
819
See Rick Westhead, CFL, union need to step up and protect the players, Toronto Star, Nov. 27, 2007, available at
2007 WLNR 23396716; Wealthy athletes go after compensation, Edmonton J. (Canada), Aug. 16, 1996, available at
1996 WLNR 3805939.
820
Farhan Lalji, CFLPA submits application for WCB coverage, TSN (Aug. 23, 2016), http://www.tsn.ca/cflpa-
submits-application-for-wcb-coverage-1.553968, archived at https://perma.cc/ZKB8-VCVP.
821
Id.
822
2014 CFL CBA, § 31.01.
823
Id.
824
2014 CFL CBA, §31.06.
825
2014 CFL CBA, § 31.03.
826
2015 MLS CBA, § 10.8.
827
Id.
828
Id.
829
2015 MLS CBA, § 22.
830
2015 MLS CBA, § 22.4.
831
Compare 2015 MLS CBA, § 22.4 and 2004 MLS CBA, § 22.4.
832
2015 MLS CBA, § 22.5.
833
Id.
834
This information was provided by the MLSPU.
835
Id.
836
See L. E. Eisenmenger, McCabe Explains Generation adidas, USSoccerPlayers.com, Jan. 8, 2010,
http://www.ussoccerplayers.com/2010/01/mccabe-explains-generation-adidas.html, archived at
https://perma.cc/RWK5-4R64.
837
2015 MLS CBA, § 24.1.
838
In Chapter 5: Compensation, Table 5-I, we use the following mean career lengths: NFL – 5.0 years; MLB – 5.6
years; NBA – 4.8 years; NHL – 5.6 years; CFL – 3.2 years; and, MLS – 3.2 years.
839
!The!retirement!benefit!amounts!for!NBA!players!were!provided!by!the!NBA.!
840
Prior to 2012, when a new CBA established a new Retirement Plan and 401(k) plan, clubs contributed amounts
into investment accounts on behalf of the players on an annual basis. For example, in 2012, if a player had played
less than 160 games in his career, the club contributed $23,820 in Canadian dollars into the player’s account that
season. If the player had played 160 or more career games, the club contributed $50,000 into the player’s account.
The amounts a player would receive under this plan after their career depends on investment results and when the
player starts to draw benefits from the account.

!
257!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
841
Benefits and Services, Nat’l Football League Players Ass’n, https://www.nflpa.com/active-players/benefits-and-
services (last visited Sep. 18, 2015), archived at https://perma.cc/45QW-DPZC.
842
See FAQs about COBRA Continuation Health Coverage, U.S. Dept. of Labor, http://www.dol.gov/ebsa/faqs/faq-
consumer-cobra.html (last visited Sep. 18, 2015), archived at http://perma.cc/79A8-EKUQ (discussing COBRA’s
temporary nature); Anna Rapa, Individual Health Insurance, Sometimes a Bane, Sometimes a Benefit, and
Increasingly the Only Option, 88 Mich. B. J. 16, 17 (2009) (“Maintaining insurance coverage under COBRA rather
than having a separate individual policy between jobs may provide the best coverage, even if COBRA premiums are
notoriously expensive.”); Tiffany M. Alexander, Are You Covered? Your Health Insurance Options, 32 Sum Fam.
Advoc. 20 (2009) (“COBRA disadvantages are (1) it tends to be much more expensive than a private policy because
it often offers better coverage, and (2) it is only a temporary solution.”)
843
While speculative, some similarity in the plans offered by MLB and the NHL may be due to overlapping leadership
at the MLBPA and NHLPA. Don Fehr was Executive Director of the MLBPA from 1983 until 2009, during which time
Fehr helped established the MLBPA’s reputation as one of the strongest unions in the country. After leaving the
MLBPA in 2009, Fehr became the NHLPA’s Executive Director in 2010. In addition, Steve Fehr, Don’s brother,
serves as outside counsel to both the MLBPA and NHLPA.
844
See Average NFL Career Length, Sharp Football Analysis, Apr. 30, 2014,
http://www.sharpfootballanalysis.com/blog/?p=2133, archived at http://perma.cc/X8QV-77A3 (discussing
disagreement between NFLPA and NFL and determining that the average drafted player plays about 5 years);
William D. Witnauer, Richard G. Rogers, Jarron M. Saint Onge, Major league baseball career length in the twentieth
century, 26 Population Res. & Policy Rev. 4, 371-386, Jun. 14, 2007,
http://link.springer.com/article/10.1007%2Fs11113-007-9038-5 (finding average MLB career to be 5.6 years).
845
For more on this issue, see Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and
Promoting the Health of NFL Players: Legal and Ethical Analysis and Recommendations, Recommendation 7:3-B
(2016).
846
According to columnist Mike Freeman, the NFLPA did analyze the potential costs of providing NFL players with
health insurance for life and found the cost to be approximately $2 billion. Mike Freeman, Two Minute Warning: How
Concussions, Crime, and Controversy Could Kill the NFL (and What the League Can Do to Survive), xxv (2015).
847
The principal distinction would be that employers require a certain number of years of service to, in part,
encourage employees to continue working for them rather than obtaining employment elsewhere. This incentive
structure is not needed in the NFL—where the vast majority of players play in the NFL for as long as they are able.
848
An exact definition for PES or PEDs is elusive. See Michael T. Lardon, Performance-Enhancing Drugs: Where
Should the Line be Drawn and by Whom? 5 Psychiatry 58 (2008) (discussing the difficulty with determining what
substances should be considered PEDs and thus banned). The United States Anti-Doping Agency describes PEDs
as substances that “have the ability or potential to drastically alter the human body and biological functions, including
the ability to considerably improve athletic performance in certain instances… [but that] can be extremely dangerous
and, in certain situations, deadly.” Effects of PEDs, U.S. Anti-Doping Agency,
http://www.usada.org/substances/effects-of-performance-enhancing-drugs/, archived at http://perma.cc/CM2U-5SGK.
849
MLB JDA, § 2(A).
850
2014 NFL Drug Policy, n.1. The NBA defines “drugs of abuse” as amphetamines, cocaine, LSD, opiates, and
PCP.
851
21 U.S.C. § 812(b)(1)(B).
852
State Marijuana Laws Map, Governing, http://www.governing.com/gov-data/state-marijuana-laws-map-medical-
recreational.html (last visited Feb. 21, 2017), archived at https://perma.cc/5U82-EAWN.
853
Nineteen sports clubs play in these states and the District of Columbia: Denver Broncos (NFL); Colorado Rockies
(MLB); Denver Nuggets (NBA); Colorado Avalanche (NHL); Colorado Rapids (MLS); New England Patriots (NFL);
Boston Red Sox (MLB); Boston Celtics (NBA); Boston Bruins (NHL); New England Revolution (MLS); Portland Trail
Blazers (NBA); Portland Timbers (MLS); Seattle Seahawks (NFL); Seattle Mariners (MLB); Seattle Sounders FC
(MLS); Washington Nationals (MLB); Washington Wizards (NBA); Washington Capitals (NHL); and, D.C. United
(MLS). The Washington football club is of course associated with Washington, D.C. but practices in Virginia and plays
in Maryland.
854
See, e.g., Nora D. Volkow, Ruben D. Baler, Wilson M. Compton, Susan R.B. Weiss, Adverse health effects of
marijuana use, 370 N. Engl. J. Med. 23 (2014); Editorial Board, Repeal Prohibition, Again, N.Y. Times, Jul. 27, 2014,
http://www.nytimes.com/interactive/2014/07/27/opinion/sunday/high-time-marijuana-legalization.html?op-nav,
archived at http://perma.cc/EH28-BZU6; Lawrence Downes, The Great Colorado Weed Experiment, N.Y. Times, Aug.
2, 2014, http://www.nytimes.com/2014/08/03/opinion/sunday/high-time-the-great-colorado-weed-experiment.html?op-
nav, archived at http://perma.cc/H6W9-Y7ZE.
855
See Kevin Seifert, Survey: Two-thirds of NFL players say legal pot equals fewer painkillers, ESPN (Nov. 2, 2016),
http://www.espn.com/nfl/story/_/id/17951858/nfl-players-legal-pot-equals-fewer-painkillers, archived at
https://perma.cc/9JJV-WENY; Darin Gantt, Former Broncos tight end says NFL should lift marijuana ban,
ProFootballTalk (Mar. 6, 2015, 6:37 AM), http://profootballtalk.nbcsports.com/2015/03/06/former-broncos-tight-end-

!
258!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
says-nfl-should-lift-marijuana-ban/, archived at http://perma.cc/82MN-BCK7; Mike Freeman, Banned, but Bountiful:
Marijuana Coveted by NFL Players as Invaluable Painkiller, Bleacher Rep., Jun. 30, 2015,
http://bleacherreport.com/articles/2486218-banned-but-bountiful-marijuana-coveted-by-nfl-players-as-invaluable-
painkiller, archived at http://perma.cc/L8QS-X2KD.
856
See Eric P. Baron, Comprehensive Review of Medical Marijuana, Cannabinoids, and Therapeutic Implications in
Medicine and Headache: What a Long Strange Trip It’s Been…, Headache 885 (2015) (collecting studies and
concluding “[t]he literature suggests that the medicinal use of cannabis may have a therapeutic role for a multitude of
diseases, particularly chronic pain disorders”); Arthur L. Caplan, Lee H. Igel, It’s Time to Normalize Medical Marijuana
in Pro Sports, Forbes (Dec. 7, 2016, 7:50 AM), http://www.forbes.com/sites/leeigel/2016/12/07/its-time-to-normalize-
medical-marijuana-in-pro-sports/#7d1977dd2e3f, archived at https://perma.cc/H5SD-6ZYC (discussing marijuana as
a pain management tool in professional sports and the US Food and Drug Administration’s approval of two
medications containing cannabinoids).
857
Zac Jackson, NFLPA will study marijuana as a pain-management tool for players, ProFootballTalk (Nov. 9, 2016,
7:19 PM), http://profootballtalk.nbcsports.com/2016/11/09/nflpa-will-study-marijuana-as-a-pain-management-tool-for-
players/, archived at https://perma.cc/S2C5-EE67.
858
Gregg Rosenthal, Marijuana legalization won’t change NFL drug policy, Nat’l Football League, Nov. 7, 2012,
http://www.nfl.com/news/story/0ap1000000091645/article/marijuana-legalization-wont-change-nfl-drug-policy,
archived at https://perma.cc/YV7M-G49B.
859
Mike Florio, Goodell says league would consider marijuana as a concussion treatment, ProFootballTalk (Jan. 23,
2014, 4:56 PM), http://profootballtalk.nbcsports.com/2014/01/23/goodell-says-league-would-consider-marijuana-as-
a-concussion-treatment/, archived at http://perma.cc/7K93-FK93; Mike Florio, NFL could indeed change its mind
about marijuana, in time, ProFootballTalk (Jan. 18, 2014, 1:47 PM),
http://profootballtalk.nbcsports.com/2014/01/18/nfl-could-indeed-change-its-mind-about-marijuana-in-time/, archived
at http://perma.cc/NTR2-NNW4.
860
In addition the reasons why certain drugs are banned, many would also likely add that the leagues regulate drugs
to: (1) protect clubs’ investments in the players; and, (2) to avoid negative publicity that results when players suffer
adverse health or legal consequences associated with drug use. See, e.g., Lee A. Linderman, A Congressional Carve
Out: The Necessity for Uniform Application of Professional Sports Leagues’ Performance-Enhancing Drug Policies,
84 S. CAL. L. REV. 751, 772 (2011) (“Sports leagues have an obvious interest in preventing their athletes from
severely damaging their own bodies through PED use. Leagues do not want their players—stars or otherwise—
destroying their own bodies because such actions would bring negative publicity to the sport and force teams to deal
with losing players to unnatural injuries.”); Mark M. Rabuano, An Examination of Drug-Testing as a Mandatory
Subject of Collective Bargaining in Major League Baseball, 4 U. PA. J. LAB. & EMP. L. 439, 458 (2002) (“Within the
League, the management-employer has a legitimate interest in controlling drug use to protect its investment and the
job performance of its employees. Because the profitability of MLB is tied to the success of players and fan support,
the preservation of League integrity through drug-testing is an issue that should thus be reserved for managerial
prerogative.”)
861
Pete Thomas, Hall’s Olympic Dream Gets the Boost It Needs, L.A. Times, Jul. 7, 2004, available at 2004 WLNR
19771636.
862
Id.
863
It is important to understand that if a player does not obtain a TUE before beginning use of the banned substance
he is likely to be disciplined, regardless of whether the drug has been prescribed. NFL player Robert Mathis was
suspended for the first four games of the 2014 season after testing positive for a banned substance that was in a
fertility drug Mathis had been prescribed to help Mathis and his wife conceive a child. Darin Gantt, Robert Mathis
balancing professional guilt and personal joy, PROFOOTBALLTALK (Jul. 31, 2014),
http://profootballtalk.nbcsports.com/2014/07/31/robert-mathis-balancing-professional-guilt-and-personal-joy/, archived
at http://perma.cc/C8DS-7VCA. Mathis failed to obtain a TUE for the drug and was thus subject to discipline. Mike
Florio, NFL responds to agent’s statement regarding Robert Mathis, PROFOOTBALLTALK (May 17, 2014, 12:57 AM),
http://profootballtalk.nbcsports.com/2014/05/17/nfl-responds-to-agents-statement-regarding-robert-mathis/, archived
at http://perma.cc/7JUH-ZS9H.
864
Amy Shipley, Drug Exemptions Triple in MLB Majority Granted to Players to Treat Attention-Deficit Disorder,
Wash. Post, Jan. 16, 2008, available at 2008 WLNR 28017256.
865
Id.
866
Id.
867
Joy R. Absalon, Orioles’ Davis ‘good to go’ with new therapeutic-use exemption, Fox Sports (Feb. 24, 2015, 9:12
PM), http://www.foxsports.com/mlb/story/baltimore-orioles-chris-davis-suspension-therapuetic-use-exemption-
adderall-022415, archived at http://perma.cc/3VS5-MTBQ.
868
Independent program administrator issues annual report, Major League Baseball (Dec. 1, 2015),
http://m.mlb.com/news/article/158704354, archived at http://perma.cc/BL74-JV9Q.

!
259!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
869
Independent Program Administrator Annual Report, Major League Baseball (Dec. 2, 2016),
http://www.mlbplayers.com/ViewArticle.dbml?SPID=181313&ATCLID=211336296&DB_OEM_ID=34000, archived at
https://perma.cc/RS3R-68H4.
870
This figure was gathered from MLB.com’s “Sortable Player” statistics page by adding together all players who had
a plate appearance and all pitchers, and then removing those pitchers that also had a plate appearance.
871
It is hard to know how this usage compares to the general population. Our research did not reveal usage rates for
a comparable control population. However, according to a national survey on drug use by the University of
Michigan, in 2015, approximately 1.6% of people aged 19-30 reported using Ritalin, an ADD medication.
Additionally, approximately 6.9% of people aged 19-30 reported using Adderall, also an ADD medication. However,
the relationship between usage and prescriptions was not provided. See Lloyd D. Johnston et al., Monitoring the
Future national survey results on drug use, 1975– 2015: Volume 2, College students and adults ages 19–55 111
(2015), available at http://monitoringthefuture.org/pubs.html#monographs.
872
See Lid Elec., Inc. v. Int’l Broth. of Elec. Workers, Local 134, 362 F.3d 940, 944 (7th Cir. 2004); Bolden v.
Southeastern Penn. Transp. Authority, 953 F.2d 807, 827-28 (3d Cir. 1991), citing National Labor Relations Board
cases and memorandum.
873
The NFL’s Specimen Collection Process is included in documents filed as part of lawsuit brought by then-Denver
Broncos Linebacker D.J. Williams against the NFL. Specifically, the Specimen Collection Process states: “[t]he player
must lower his pants and underwear below his knees”; [t]he player must not have any clothing above his knees
(naked from ‘Knees-to-Noggin’)”; and, “[t]he collector… will monitor the furnishing of the specimen by direct frontal
observation in order to assure the integrity of the specimen until the adequate volume of 100mL minimum is
provided.” See Exhibits in Support of Brief by Plaintiffs Ryan McBean and Genos “D.J.” Williams, Williams, et al. v.
Nat’l Football League, 12-cv-650 (D. Colo. Apr. 2, 2012), ECF No. 41-1.
874
Mike Florio, League wants HGH testing, needs players to want it, too, ProFootballTalk (May 4, 2013, 3:03 PM),
http://profootballtalk.nbcsports.com/2013/05/04/league-wants-hgh-testing-needs-players-to-want-it-too/, archived at
http://perma.cc/A8BD-ZRFW; Mike Florio, NFLPA says NFL could have had HGH testing before MLB,
ProFootballTalk (Jan. 11, 2013, 2:23 PM), http://profootballtalk.nbcsports.com/2013/01/11/nflpa-says-nfl-could-have-
had-hgh-testing-before-mlb/, archived at http://perma.cc/4LP5-879F.
875
NFL PES Policy, Appendix A.
876
Id.
877
NFL PES Policy, General Statement of Policy, n. 1.
878
Synthetic marijuana was banned in 2016. Mike Florio, NFL, NFLPA agree on revised drug, PED policies,
ProFootballTalk (Oct. 9, 2016, 8:40 AM), http://profootballtalk.nbcsports.com/2016/10/09/nfl-nflpa-agree-on-revised-
drug-ped-policies/, archived at https://perma.cc/4BVM-WYMT.
879
NFL Substance Abuse Policy, General Policy, n. 1.
880
NFL Substance Abuse Policy, § 1.3.3.
881
Michael David Smith, A new drug testing agreement could benefit Welker, Gordon, ProFootballTalk (Sept. 4,
2014, 7:47 PM), http://profootballtalk.nbcsports.com/2014/09/04/a-new-drug-testing-agreement-could-benefit-welker-
gordon/, archived at http://perma.cc/X8UX-45KB; Darin Gantt, Orlando Scandrick ready to rejoin Cowboys once new
drug deal done, ProFootballTalk (Sept. 13, 2014, 8:47 AM), http://profootballtalk.nbcsports.com/2014/09/13/orlando-
scandrick-ready-to-rejoin-cowboys-once-new-drug-deal-done/, archived at http://perma.cc/6AJD-B9DK.
882
Smith, supra n. 881; Gantt, supra n. 881.
883
NFL PES Policy, § 6, n. 5.
884
NFL PES Policy, §§ 3.1, 7.
885
NFL PES Policy, § 11. If a player tests positive for a banned substance, he may either: “accept the result and the
disciple, await the results of the scheduled ‘B’ sample analysis, or have an Observing Toxicologist witness the ‘B’
sample analysis.” NFL PES Policy, § 4.2. If the “B” sample does not confirm a positive result, then the Independent
Administrator never notifies the NFLMC or NFLPA of a positive test result. Id.
886
NFL PES Policy, § 5.
887
Id. Unlike other violations of the PED Policy, players who are convicted or otherwise admit to have used,
possessed, or distributed PEDs are subject to discipline at the discretion of the Commissioner, including suspension
up to six games for a first violation or, if appropriate, termination of a player’s contract. Id. Other PED Policy violations
follow the disciplinary schedule outlined in Section 6.
888
NFL PES Policy, §§ 3.3, 6, Appendix H. Players who fail to appear for testing for reasons other than attempting to
deliberately evade or avoid testing are also subject to discipline—a fine of up to $25,000 and placement in the
reasonable cause testing program for a first violation, a fine of two weeks’ pay for a second violation, and a four-
game suspension without pay for a third violation. NFL PES Policy, Appendix H.
889
NFL PES Policy, § 6.
890
See, e.g., NFL Substance Abuse Policy, § 1.3.2.
891
NFL Substance Abuse Policy, § 1.3.3. If a player tests positive for a banned substance, he may either: “accept the
result and the disciple, await the results of the scheduled ‘B’ sample analysis, or have an Observing Toxicologist
witness the ‘B’ sample analysis.” Id. If the “B” sample does not confirm a positive result, then the Independent

!
260!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
Administrator never notifies the NFLMC or NFLPA of a positive test result. Id. The “B” sample need only show that
the substance revealed in the “A” sample test is evidence to the “limits of detection.” Id.
892
Id.
893
NFL Substance Abuse Policy, Appendix E. A player who fails to appear for testing, but who is adjudged not to
have purposefully attempted to evade or avoid testing is subject to a $25,000 fine and placement in the Intervention
Program for his first violation, a fine of 2/17ths of his Paragraph 5 NFL Player Contract salary for his second violation,
and a four game suspension without pay for his third violation. Id.
894
NFL Substance Abuse Policy, § 2.
895
Id. A nolo contendere plea is one in which the accused does not contest or admit guilt. See Black’s Law Dictionary
(9th ed. 2009) (defining “nolo plea” as “[a] plea by which the defendant does not contest or admit guilt.”).
896
NFL PES Policy, § 3.1.
897
Id.
898
Id.
899
Id.
900
In other words, for 8 of the NFL’s 32 clubs, half of the ten players randomly selected for urine testing in any given
week are also subject to blood testing.
901
NFL PES Policy, § 7.
902
“As used in this Policy, sufficient credible evidence includes but is not limited to: criminal convictions or plea
arrangements; admissions, declarations, affidavits, authenticated witness statements, corroborated law enforcement
reports or testimony in legal proceedings; authenticated banking, telephone, medical or pharmacy records; or credible
information obtained from Players who provide assistance pursuant to Section 10 [“Appeals”] of the Policy.” NFL PES
Policy, § 3.1 n.4.
903
NFL PES Policy, §§ 3.1, 7.
904
See, e.g., NFL PES Policy, § 7.
905
All NFL players are eligible for entrance into the Intervention Program. Players enter Stage One of the Intervention
Program through a positive test result, behavior that exhibits symptoms of misuse of substances of abuse (e.g., an
arrest for misuse of substance of abuse), or self-referral. NFL Substance Abuse Policy, § 1.4.1. A self-referred player
always remains in Stage One of the Substance Abuse Policy. Id.
906
NFL Substance Abuse Policy, § 1.3.1.
907
Mike Florio, Marijuana testing window opens today, ProFootballTalk (Apr. 20, 2015, 8:12 AM),
http://profootballtalk.nbcsports.com/2015/04/20/marijuana-testing-window-opens-today/, archived at
http://perma.cc/DU9Z-RYGW.
908
Id.
909
Mike Florio, NFLPA gives players 30-day marijuana warning, ProFootballTalk (Mar. 19, 2015, 3:27 PM),
http://profootballtalk.nbcsports.com/2015/03/19/nflpa-gives-players-30-day-marijuana-warning/, archived at
http://perma.cc/Q4PC-NUEN.
910
See Ben Volin, How did Aaron Hernandez not fail NFL drug tests?, Bos. Globe, Apr. 4, 2015,
http://www.bostonglobe.com/sports/2015/04/04/how-did-aaron-hernandez-not-fail-nfl-drug-
tests/NXI7edYeTLKFhJIyfe0s1M/story.html, archived at http://perma.cc/DMU4-3GGX.
911
NFL PES Policy, § 2.1.
912
See John A. Lombardo, MD, Max Sports Medicine OhioHealth, http://maxsportscenter.com/Meet-Our-Team/John-
A-Lombardo,-MD (last visited Aug. 31, 2015), archived at http://perma.cc/872S-R7C9.
913
NFL PES Policy, § 2.1.
914
NFL PES Policy, §§ 2.2, 2.3, 2.4.
915
NFL Substance Abuse Policy, § 1.1.1.
916
NFL Substance Abuse Policy, § 1.1.2.
917
Selected by the medical director, treating clinicians are responsible for administering the treatment plans for
players assigned to them. NFL Substance Abuse Policy, § 1.1.3.
918
Each NFL club must designate one of its affiliated physicians as its team physician for substance abuse matters.
NFL Substance Abuse Policy, § 1.1.4. The team substance abuse physician consults and coordinates club-level
aspects of the player’s treatment program, including the prescription or prohibition of certain medications necessary
to facilitate compliance with the treatment program. Id.
919
The chief forensic toxicologist, jointly selected by the NFLMC and NFLPA, is responsible for laboratory evaluation
of urine samples, providing scientific advice on toxicology matters, scientific interpretation of positive drug findings,
and providing forensic testimony as needed. NFL Substance Abuse Policy, § 1.1.5.
920
“The NFL and NFLPA shall jointly agree upon one or more Collection Vendors to be responsible for specimen
collection, storage and transportation to the designated laboratory.” NFL Substance Abuse Policy, § 1.1.6.
921
Club physicians facilitate players’ entrance into the Intervention Program on a self-referral basis. See NFL
Substance Abuse Policy, § 1.4.1.
922
NFL PES Policy, Appendix I; NFL Substance Abuse Policy, Appendix F.
923
Id.

!
261!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
924
Id.
925
NFL Substance Abuse Policy at p. 1.
926
Id.
927
NFL Substance Abuse Policy, § 1.4.1.
928
NFL Substance Abuse Policy, § 1.5.1(a).
929
Id.
930
Id.
931
NFL Substance Abuse Policy, § 1.5.1(b).
932
Id.
933
NFL Substance Abuse Policy, § 1.5.2(a).
934
NFL Substance Abuse Policy, § 1.5.2(d).
935
Id.
936
In all of the leagues, suspensions are without pay except in rare circumstances.
937
NFL PES Policy, § 6.
938
“[S]ufficient credible evidence includes but is not limited to: criminal convictions or plea arrangements; admissions,
declarations, affidavits, authenticated witness statements, corroborated law enforcement reports or testimony in legal
proceedings; authenticated banking, telephone, medical or pharmacy records; or credible information obtained from
Players who provide assistance[.]” NFL PES Policy, § 3.1, n. 4.
939
Spotrac.com provides a list of NFL suspensions. NFL Fines & Suspensions 2016, Spotrac,
http://www.spotrac.com/nfl/fines-suspensions/ (last visited Jan. 23, 2017), archived at https://perma.cc/KAK9-63FG.
940
As stated above, Spotrac.com provides a list of NFL suspensions. See NFL Fines & Suspensions 2015, Spotrac,
http://www.spotrac.com/nfl/fines-suspensions/2015/ (last visited Mar. 10, 2016), archived at https://perma.cc/R3K4-
FB74; NFL Fines & Suspensions 2014, Spotrac, http://www.spotrac.com/nfl/fines-suspensions/2014/ (last visited Mar.
10, 2016), archived at http://perma.cc/4VCB-PSCM. Additional research was then done on each player on the list to
determine the reported cause of the suspension.
941
NFL PES Policy, § 14.
942
See id., citing 2011 NFL CBA, Art. 4, § 9. See also Chris Deubert, Glenn M. Wong, John Howe, All Four Quarters:
A Retrospective and Analysis of the 2011 Collective Bargaining Process and Agreement in the National Football
League, 19 UCLA Ent. L. Rev. 1, 48-51 (2012) discussing clubs’ efforts to recoup portions of bonus money already
paid to players); Chris Deubert, Glenn M. Wong, Understanding the Evolution of Signing Bonuses and Guaranteed
Money in the National Football League: Preparing for the 2011 Collective Bargaining Negotiations, 16 UCLA Ent. L.
Rev. 179, 202-26 (2009) (same).
943
See 2011 NFL CBA, At. 4, § 9(g) (discussing voiding of guarantees).
944
NFL PES Policy, § 1.4.1.
945
See Spotrac.com, supra note 939.
946
Id.
947
NFL Substance Abuse Policy, § 2.2.
948
Id.
949
Id.
950
Id. at § 2.3.
951
Id.
952
Id.
953
NFL PES Policy, § 12; NFL Substance Abuse Policy, § 1.2.
954
NFL PES Policy, § 12.1.
955
NFL PES Policy, § 12.
956
NFL PES Policy, § 12.2.
957
NFL Substance Abuse Policy, § 1.2.1.
958
Id.
959
NFL Substance Abuse Policy, § 1.2.3.
960
“Any and all drugs or substances included on Schedules I and II of the Code of Federal Regulations’ Schedule of
Controlled Substances . . . shall be considered Drugs of Abuse covered by the Program,” in addition to synthetic and
natural marijuana, cocaine, LSD, opiates, MDMA, GHB, and PCP (and their analogues). MLB Joint Program, § 2(A).
961
“Any and all anabolic androgenic steroids covered by Schedule III of the Code of Federal Regulations’ Schedule of
Controlled Substances . . . and [certain enumerated] categories of hormones and agents with antiestrogenic activity .
. . shall be considered Performance Enhancing Substances covered by the Program. Anabolic androgenic steroids,
hormones, and agents with antiestrogenic activity, that may not be lawfully obtained or used in the United States
(including, for example, “designer steroids” and peptide hormones) also shall be considered Performance Enhancing
Substances irrespective of whether they are covered by Schedule III.” MLB Joint Program, § 2(B). Human Growth
Hormone (hGH) is explicitly listed as a PED. Id.
962
Stimulants are defined in the Joint Program by an exhaustive list of 56 substances, including amphetamine,
ephedrine, and methamphetamine. MLB Joint Program, § 2(C).

!
262!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
963
MLB Joint Program, § 2(D). “DHEA is a hormone that is naturally made by the human body. . . . Athletes and other
people use DHEA to increase muscle mass, strength, and energy.” DHEA, Medline Plus - U.S. Nat’l Library of Med.,
http://www.nlm.nih.gov/medlineplus/druginfo/natural/331.html#Description (last visited Aug. 31, 2015), archived at
http://perma.cc/R76C-YR75. As recently as 2009, MLB was the only of the big four American professional sports
leagues to allow DHEA. See Jeff Passan, Baseball still allows the steroid DHEA, Yahoo! Sports, May 14, 2009,
http://sports.yahoo.com/mlb/news?slug=jp-dhealegal051409, archived at http://perma.cc/5WJP-WSL8. MLB and the
MLBPA often fought over inclusion of DHEA on the prohibited substance list, see id., which may explain why DHEA
was included in its own category when MLB finally added it to the list.
964
MLB Joint Program, § 2(E).
965
Id.
966
MLB Joint Program, § 3(A)(1).
967
Id.
968
MLB Joint Program, § 3(A)(3).
969
MLB Joint Program, § 3(F)(1). This situation is known as an “analytical positive.”
970
MLB Joint Program, § 3(F)(2).
971
MLB Joint Program, § 3(F)(3).
972
MLB Joint Program, § 7(G)(2). Suspensions under this provision of the Joint Program do not follow a specified
punishment schedule; they may, however, qualify as predicate offenses that increase the punishment for subsequent
violations. See MLB Joint Program, § 7(A).
973
MLB Joint Program, § 3(A)(1).
974
MLBPA, MLB Announce Details of New Labor Agreement, MLBPA (Dec. 2, 2016),
http://www.mlbplayers.com/ViewArticle.dbml?DB_OEM_ID=34000&ATCLID=211336390, archived at
https://perma.cc/4XUA-2DAW.
975
Id.; MLB Joint Program, § 3(A)(2).
976
MLB Joint Program, § 3(A)(3)(a).
977
MLB Joint Program, § 3(A)(3). Of those 900 hGH tests, 500 are conducted during the season and 400 are
performed during the off-season. MLB Joint Program, § 3(A)(3)(b)–(c); MLBPA, MLB Announce Details of New Labor
Agreement, MLBPA (Dec. 2, 2016),
http://www.mlbplayers.com/ViewArticle.dbml?DB_OEM_ID=34000&ATCLID=211336390, archived at
https://perma.cc/4XUA-2DAW.
978
See MLB Joint Program, § 3(A)(3).
979
Independent Program Administrator Issues Annual Report, Major League Baseball (Dec. 2, 2016),
http://www.mlbplayers.com/ViewArticle.dbml?SPID=181313&ATCLID=211336296&DB_OEM_ID=34000, archived at
https://perma.cc/2PPQ-S397.
980
Id.
981
Id.
982
MLB Joint Program, § 3(C)(1). However, the party receiving the notification may dispute the reasonable cause
basis, in which case the Arbitration Panel Chair will determine whether reasonable cause exists. MLB Joint Program,
§ 3(C)(1).
983
MLB Joint Program, §§ 3(D)(1)–(2). These follow-up tests do not count toward the 3,200 random urine tests or
400 random hGH tests otherwise permitted under the Joint Program. Id.
984
MLB Joint Program, §§ 3(B), 3(C)(2)(a).
985
MLB Joint Program, § 4(A).
986
MLB Joint Program, § 4(B)(1).
987
MLB Joint Program, § 1(A)(1).
988
MLB Joint Program, § 1(A)(2).
989
MLB Joint Program, §§ 1(B)(1)–(2). The Treatment Board made headlines in 2015 after deciding not to suspend
former Los Angeles Angels (and current Texas Rangers) player Josh Hamilton. Hamilton, who had struggled with
cocaine and alcohol addiction in the past, confessed to Major League Baseball in February that he had suffered a
relapse in his sobriety in an incident involving cocaine. Matt Schiavenza, Josh Hamilton’s Relapse Reveals Baseball’s
Double Standard on Drugs, Atlantic, Apr. 4, 2015, http://www.theatlantic.com/entertainment/archive/2015/04/josh-
hamiltons-relapse-reveals-baseballs-hypocrisy-on-drugs/389685/, archived at http://perma.cc/WXP8-M4JP. Because
Hamilton self-reported the incident and had not failed a drug test since 2004, he appeared to technically qualify as a
first-time offender under the Joint Program. See Jeff Todd, Josh Hamilton Facing Discipline for Drug of Abuse, MLB
Trade Rumors (Feb. 25, 2015), http://www.mlbtraderumors.com/2015/02/josh-hamilton-meeting-with-mlb-regarding-
disciplinary-matter.html, archived at https://perma.cc/SDB9-Y4K9; Cliff Corcoran, Report: Josh Hamilton’s Career Hits
Roadblock as He Relapses on Drugs, Sports Illustrated, Feb. 26, 2015, http://www.si.com/mlb/2015/02/25/josh-
hamilton-angels-relapse-drugs, archived at http://perma.cc/EWL4-U5AT. However, MLB argued that Hamilton had
violated his treatment program, which dated back as far as 2003 when Hamilton was in the minor leagues with the
Tampa Bay Rays. Michael O’Keefe & Teri Thompson, Arbitrator Rules for Josh Hamilton, Angels Outfielder Will Not
Be Suspended by MLB for Substance Abuse Relapse, N.Y. Daily News, Apr. 3, 2015,

!
263!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
http://www.nydailynews.com/sports/baseball/arbitrator-rules-josh-hamilton-angel-dodges-suspension-article-
1.2172441, archived at http://perma.cc/L7UN-MAX5. Hamilton and his camp, meanwhile, argued that he had faithfully
followed his treatment program, which included counseling and drug testing, and he had a “one-night slip which he
immediately self-reported.” Id. Ultimately, an arbitrator ruled that Hamilton’s conduct did not violate his treatment
program and MLB thus could not suspend or impose any discipline on him. Ted Berg, Josh Hamilton Will Not Be
Suspended for Reported Offseason Drug Relapse, USA Today, Apr. 3, 2015, http://ftw.usatoday.com/2015/04/josh-
hamilton-los-angeles-angels-suspension-drug-relapse-mlb, archived at https://perma.cc/W8QC-GFM3 (quoting
MLB’s statement on the matter); see also MLB Joint Program, § 4(C)(3).
990
MLB Joint Program, § 1(A)(2)(g).
991
MLB Joint Program, § 3(I)(1).
992
MLB Joint Program, § 3(I)(3).
993
MLB Joint Program, § 4.
994
MLB Joint Program, § 4(B)(1).
995
Id.
996
MLB Joint Program, §§ 7(A)(1)–(3), 7(E)(1)–(3).
997
MLB Joint Program, § 7(F)(1)–(2).
998
MLB Joint Program, § 7(B)(1)–(4); MLBPA, MLB Announce Details of New Labor Agreement, MLBPA (Dec. 2,
2016), http://www.mlbplayers.com/ViewArticle.dbml?DB_OEM_ID=34000&ATCLID=211336390, archived at
https://perma.cc/4XUA-2DAW.
999
MLB Joint Program, § 7(B)(1)–(4).
1000
MLB Joint Program, §§ 7(F)(1), (3).
1001
MLB Joint Program, § 7(C)(1)–(4).
1002
MLB Joint Program, § 7(E)(1)–(3).
1003
MLB Joint Program, §§ 7(F)(1), (3).
1004
MLB Joint Program, § 7(D)(1)–(5).
1005
Additional failures to comply with the treatment program results in further discipline at the Commissioner‘s
discretion. MLB Joint Program, § 7(C)(5).
1006
MLB Joint Program, §§ 7(F)(1), (3).
1007
MLB Joint Program, § 7(E)(1)–(3). However, absent a conviction, players are not subject to suspension for the
use or possession of marijuana, hashish, or synthetic THC. MLB Joint Program, § 7(D)(5). Also, drug of abuse
violations do not include alcohol or alcohol-related (e.g., DUI) violations.
1008
DHEA, Medline Plus - U.S. Nat’l Library of Med.,
http://www.nlm.nih.gov/medlineplus/druginfo/natural/331.html#Description (last visited Aug. 31, 2015), archived at
http://perma.cc/R76C-YR75.
1009
DHEA is specifically exempt from the term “anabolic steroid” in the Controlled Substances Act. 21 U.S.C. §
802(41)(A).
1010
See, e.g., DHEA, Walgreens, http://www.walgreens.com/store/c/dhea/ID=361725-tier3 (last visited Aug. 31,
2015), archived at http://perma.cc/7E6P-PH4Y (listing DHEA for sale); DHEA, GNC,
http://www.gnc.com/Vitamins/Specialty-Supplements/DHEA/family.jsp?categoryId=2166425&sr=1&origkw=dhea (last
visited Aug. 31, 2015), archived at http://perma.cc/F79Z-K7WK (same).
1011
WADA, established in 1999, is an international agency funded by sports organizations and governments with its
principal focus on eliminating the use of PES in sports. WADA publishes annually a “Prohibited List” that lists
prohibited substances. The WADA Code and the Prohibited List are the governing anti-doping documents of all
Olympic sports organizations and most sports organizations worldwide.
1012
See MLB Joint Program, § 2(D); NFL Steroid Policy, App. A – List of Prohibited Substances; 201 NBA CBA, Ex. I-
2 – Prohibited Substances; The World Anti-Doping Code, WADA (2015), https://wada-main-
prod.s3.amazonaws.com/resources/files/wada-2015-prohibited-list-en.pdf, archived at http://perma.cc/P2KM-KKKB.
The NHL substantially uses the WADA Code.
1013
MLB Joint Program, § 5(B)(1).
1014
MLB Joint Program, § 5(B)(4).
1015
MLB Joint Program, § 5(D)(1).
1016
Id. Clubs must then keep that information confidential. See MLB Joint Program, § 5(B)(1).
1017
MLB Joint Program, § 5(C).
1018
MLB Joint Program, § 5(C)(1).
1019
MLB Joint Program, § 5(E).
1020
Drugs of abuse include, among other substances, cocaine, LSD, methamphetamine, opiates, and PCP. 2017
NBA CBA, Ex. I-2.
1021
Exhibit I-2 to the CBA specifically lists out over 150 banned SPEDs. hGH is included among banned SPEDs.
1022
Exhibit I-2 to the CBA includes 24 banned diuretics.
1023
The 2017 NBA CBA does not specify whether the illegality of the steroid or PES refers to federal and/or state law.
However, according to the NBA, in practice, the league is concerned with federal law.

!
264!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1024
2017 NBA CBA, Art. XXXIII § 16.
1025
2017 NBA CBA, Art. XXXIII, § 4(a).
1026
2017 NBA CBA, Art. XXXIII, § 4(d)(i).
1027
2017 NBA CBA, Art. XXXIII, § 4(d)(ii).
1028
2017 NBA CBA, Art. XXXIII, § 4(d)(vi).
1029
2017 NBA CBA, Art. XXXIII, § 4(d)(iii).
1030
2017 NBA CBA, Art. XXXIII, § 4(d)(iv).
1031
2017 NBA CBA, Art. XXXIII, § 4(d)(v).
1032
2017 NBA CBA, Art. XXXIII, § 5(a).
1033
2017 NBA CBA, Art. XXXIII, § 6(a). Off-season urine samples are only tested for SPEDs and diuretics. Id.
1034
!2017!NBA!CBA,!Art.!XXXIII,!§!14(a).!
1035
2017 NBA CBA, Art. XXXIII, § 6(a).
1036
2017 NBA CBA, Art. XXXIII, § 5(a). “In evaluating the information presented to him, the Independent Expert shall
use his independent judgment based upon his experience in substance abuse detection and enforcement.” 2017
NBA CBA, Art. XXXIII, § 5(b).
1037
Id.; 2017 NBA CBA, Ex. I-1.
1038
2017 NBA CBA, Art. XXXIII, § 2(a). In addition to generally managing and overseeing the Program, the Medical
Director is expressly responsible for selecting and supervising counselors (preferably, retired NBA players) and other
personnel necessary for the effective implementation of the Program and evaluating and treating players subject to
the Program. Id.
1039
!2017 NBA CBA, Art. XXXIII, § 2(b).!
1040
2017 NBA CBA, Art. XXXIII, § 2(c).
1041
2017 NBA CBA, Art. XXXIII, § 2(e).
1042
2017 NBA CBA, Art. XXXIII, § 2(g).
1043
Email from David Weiss, Associate Vice President and Assistant General Counsel, NBA, to Christopher R.
Deubert (Sep. 1, 2015).
1044
Id.
1045
Id.
1046
2017 NBA CBA, Art. XXXIII, § 1(f); Art. XXXIII, § 7.
1047
2017 NBA CBA, Art. XXXIII, § 6(b)(i).
1048
2017 NBA CBA, Art. XXXIII, 7(a).
1049
2017 NBA CBA, Art. XXXIII, § 1(k).
1050
2011 NBA CBA, Art. XXXIII, § 8(c).
1051
Id.
1052
Id.
1053
2017 NBA CBA, Art. XXXIII, § 8(a).
1054
2017 NBA CBA, Art. XXXIII, § 1(s).
1055
2017 NBA CBA, Art. XXXIII, § 9(b).
1056
Id.
1057
2011 NBA CBA, Art. XXXIII, § 9(a).
1058
See 2017 NBA CBA, Art. XXXIII, § 1(b) (“A player may not Come Forward Voluntarily for the use of a SPED”).
1059
2017 NBA CBA, Art. XXXIII, § 6(b)(i).
1060
2017 NBA CBA, Art. XXXIII, § 10(a)(ii)(1).
1061
2017 NBA CBA, Art. XXXIII, § 10(a)(ii)(2).
1062
See 2017 NBA CBA, Art. XXXIII, § 6(c); Art. XXXIII,§ 11(a).
1063
In reviewing a draft of this Report, the NBA confirmed that a veteran player that commits his first violation of the
Anti-Drug Program in relation to a drug of abuse (excluding marijuana) is dismissed and disqualified from the NBA
and is not entered into the Drugs of Abuse Program, i.e., the NBA does not provide or facilitate treatment for the
player.
1064
2017 NBA CBA, Art. XXXIII, § 10(a)(ii)(1).
1065
2017 NBA CBA, Art. XXXIII, § 10(a)(ii)(2).
1066
2017 NBA CBA, Art. XXXIII, § 7(a)(iv).
1067
2017 NBA CBA, Art. VI, § 14.
1068
2017 NBA CBA, Art. XXXIII, § 8(c)(A).
1069
2017 NBA CBA, Art. XXXIII, § 8(c)(B).
1070
2017 NBA CBA, Art. XXXIII, § 8(c)(C).
1071
2017 NBA CBA, Art. XXXIII, § 8(c)(D).
1072
2017 NBA CBA, Art. XXXIII § 8(a)(iii).
1073
2017 NBA CBA, Art. XXXIII, § 9(b)(A).
1074
2017 NBA CBA, Art. XXXIII, § 9(b)(B).

!
265!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1075
2017 NBA CBA, Art. XXXIII, § 9(b)(C).
1076
2011 NBA CBA, Art. XXXIII § 9(a).
1077
See 2017 NBA CBA, Art. XXXIII, § 1(b) (“A player may not Come Forward Voluntarily for the use of a SPED”).
1078
2017 NBA CBA, Art. XXXIII § 3(a).
1079
Id.
1080
2017 NBA CBA, Art. XXXIII § 3(b).
1081
The list itself does not appear to be publicly available; however, the parties agreed by letter agreement
accompanying the 2013 CBA to include on the Prohibited Substances List “‘illegal’ stimulants and amphetamines . . .
that are relevant to the sport of hockey.” NHL CBA, Issues Related to Article 47 of the CBA Letter Agreement.
1082
2013 NHL CBA, Letter Agreement, Don Zavelo, General Counsel, NHLPA, to William L. Daly, Deputy
Commissioner, NHL re: Issues Related to Article 47 of the CBA (Feb. 15, 2013).
1083
NHL/NHLPA, Substance Abuse and Behavioral Program Ex. A (Sep. 1996).
1084
See, e.g., Mark Craig, Deer-Antler Spray Latest ‘Thorny’ Issue in Athlete Supplements, Star Trib., Jul. 22, 2013,
http://www.startribune.com/sports/vikings/216523471.html, archived at http://perma.cc/RUG5-CCM9 (“The NHL and
NBA don’t test blood, although the NBA reportedly is getting closer to doing so.”); Bill Simmons, Daring to Ask the
PED Question, Grantland, Feb. 1, 2013, http://grantland.com/features/daring-ask-ped-question/, archived at
https://perma.cc/Y3A6-52WZ (“We look the other way when the MLB, NFL, NBA and NHL players associations keep
blocking blood testing in their respective sports (MLB finally started blood testing for the 2013 season).”). Additionally,
while the NHL discussed implementing hGH testing over the summer of 2013, it had no policy in place as of April
2015. See Mark Zwolinski, NHL Delays Testing for Human Growth Hormone Until 2014-15 Season at Earliest,
Toronto Star, Aug. 14, 2013,
http://www.thestar.com/sports/hockey/2013/08/14/nhl_delays_testing_for_human_growth_hormone_until_201415_se
ason_at_earliest.html#, archived at http://perma.cc/X89Z-RBYJ; Andrew Kehapril, N.B.A. to Test Players for H.G.H.
Starting Next Season, N.Y. Times, Apr. 17, 2015, http://www.nytimes.com/2015/04/17/sports/basketball/nba-to-test-
players-for-hgh-starting-next-season.html, archived at http://perma.cc/W7VM-85VS. Growth hormone is currently on
WADA‘s 2015 Prohibited Substances List from which NHL chooses its prohibited substances, however. See The
World Anti-Doping Code, WADA (2015), https://wada-main-prod.s3.amazonaws.com/resources/files/wada-2015-
prohibited-list-en.pdf, archived at http://perma.cc/P2KM-KKKB.
1085
See 2013 NHL CBA, Art. 47 § 6(d). The determination of whether a player had an unexcused failure or refusal or
whether a player attempted to substitute, dilute, mask, or adulterate a specimen rests with the Program Doctors,
subject to appeal to the Impartial Grievance Arbitrator. Id.
1086
2013 NHL CBA, Art. 47.9(e).
1087
2013 NHL CBA, Art. 47, § 8(b).
1088
Id.
1089
2013 NHL CBA, Art. 47, § 8(c).
1090
Id.
1091
NHL/NHLPA, Substance Abuse and Behavioral Program Ex. A (Sept. 1996).
1092
NHL/NHLPA, Substance Abuse and Behavioral Program Ex. A (Sept. 1996). For example, the cutoff level for
marijuana metabolites is 50 ng/ml for the initial test. If a specimen is identified as positive, then the program doctors
should confirm the presence of marijuana metabolites using gas chromatography/mass spectrometry techniques at
the cutoff value of 15 ng/ml. Id.
1093
2013 NHL CBA, Art. 47, § 6(a).
1094
Id.
1095
See 2013 NHL CBA, Art. 47, § 6.
1096
See id.
1097
2013 NHL CBA, Art. 47, § 6(c).
1098
Id.
1099
2013 NHL CBA, § 47.4(b).
1100
Id.
1101
Mike Halford, Report: NHL to Implement Comprehensive Cocaine Testing By End of Season, Pro Hockey Talk
(Nov. 23, 2015, 2:31 PM), http://nhl.nbcsports.com/2015/11/23/report-nhl-to-implement-comprehensive-cocaine-
testing-by-end-of-season/, archived at http://perma.cc/A66B-AL8Q.
1102
Id.
1103
NHL/NHLPA, Substance Abuse and Behavioral Program 4 (Sept. 1996).
1104
NHL/NHLPA, Substance Abuse and Behavioral Program 4 (Sept. 1996). Players may voluntarily seek treatment
through the SABH Program or Team Personnel (club physicians, trainers, coaches, and managers) may refer a
player to the Program. See id. at 4.
1105
2013 NHL CBA, Art. 47 § 2.
1106
The NHL is the only of the four major American sports leagues to use the WADA Prohibited List in choosing its
own prohibited substances.
1107
Id.

!
266!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1108
NHL/NHLPA, Substance Abuse and Behavioral Program 2 (Sept. 1996). The SABH is available as Exhibit C to
the Notice of Removal (ECF No. 1) in the case of Boogaard v. Nat’l Hockey League, No. 1:13-cv-04846 (N.D. Ill. July
3, 2013).
1109
Id.
1110
2013 NHL CBA, Art. 47 § 10.
1111
Id.
1112
NHL/NHLPA, Substance Abuse and Behavioral Program 1 (Sept. 1996).
1113
Id. at 3.
1114
2013 NHL CBA, Art. 47.7(a)(i).
1115
2013 NHL CBA, Art. 47.7(a)(ii).
1116
2013 NHL CBA, Art. 47.7(a)(iii).
1117
Andrew DeWitt, Are NHL players using PEDs? Jonathan Toews says naive to say no, CBS Sports (Aug. 16,
2013, 10:49 AM), http://www.cbssports.com/nhl/eye-on-hockey/23177818/are-nhl-players-using-peds-jonathan-
toews-says-naive-to-think-no, archived at http://perma.cc/4GMB-ENEH.
1118
Basketball and soccer are also Olympic sports and thus performance-enhancing drug usage in those sports
might also be lowered as a result of the Olympic drug-testing programs.
1119
NHL/NHLPA, Substance Abuse and Behavioral Program 4 (Sept. 1996).
1120
Id.
1121
Id.
1122
Id.
1123
Id.
1124
Id. at § 4(C).
1125
2013 NHL CBA, Art. 18-A.2.
1126
Id. at Art. 18-A.4.
1127
2013 NHL CBA, Art. 47 § 11. If the grievance is upheld, the Arbitrator can fashion an appropriate remedy
pursuant to traditional standards of contract law. Id.
1128
NHL/NHLPA, Substance Abuse and Behavioral Program Ex. B (Sept. 1996).
1129
See id. at Ex. C.
1130
Id. at 2.
1131
2014 CFL CBA, § 32.02.
1132
2014 CFL CBA, § 32.01.
1133
2016 CFL PED Policy, Appendix D. HGH is included on the list. Id.
1134
2016 CFL PED Policy, § 2.01.3.
1135
2016 CFL PED Policy, § 7.02.
1136
2016 CFL PED Policy, §§ 6.01, 6.02.
1137
CFL, CFLPA Agree on New Drug Policy for the 2016 Season, Can. Football League,
http://www.cfl.ca/2016/04/21/cfl-cflpa-agree-new-drug-policy-2016-season/ (last visited Apr. 25, 2016), archived at
https://perma.cc/4QY4-2SGL; 2016 CFL PED Policy, App. C.
1138
2016 CFL PED Policy, § 5.04.2.
1139
2016 CFL PED Policy, § 5.04.3.
1140
2016 CFL PED Policy, § 5.04.1.
1141
Id.
1142
2016 CFL PED Policy, § 3.
1143
The Designated Medical Authority is an individual jointly appointed by the CFL and CFLPA who has sole
responsibility for reviewing Therapeutic Use Exemption applications. 2016 CFL PED Policy, § 5.03.1.
1144
2016 CFL PED Policy, § 5.03.4.
1145
2016 CFL PED Policy, § 9.01.1.
1146
Id.
1147
CFL, CFLPA Agree on New Drug Policy for the 2016 Season, Can. Football League,
http://www.cfl.ca/2016/04/21/cfl-cflpa-agree-new-drug-policy-2016-season/ (last visited Apr. 25, 2016), archived at
https://perma.cc/4QY4-2SGL; CFL PED Policy, § 7.03
1148
Id.
1149
Id.
1150
Id.
1151
2016 CFL PED Policy, § 9.01.2.
1152
2016 CFL PED Policy, § 4.01.1.
1153
2016 CFL PED Policy, § 4.01.2.
1154
Id.
1155
MLS Substance Abuse Policy, § VI(A).
1156
Id.
1157
Id. at § VI(B).

!
267!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1158
Id. at § VI(C).
1159
Id. at § VI(D).
1160
Id. at § III(C) (“All specimen collection shall be done in accordance with the WADA Guidelines for Urine Sample
Collection.”)
1161
The Substance Abuse Policy also governs “violation[s] of criminal law,” “domestic violence,” and, “illegal or
excessive gambling[.]” MLS Substance Abuse Policy, § 5(A). Such violations are subject to “discipline[] for just
cause.” Id. at § X(B)(2).
1162
Id. at § V(A).
1163
Id. at § IX(A).
1164
Id. at § VII(B).
1165
Id. at § VII(A)(1).
1166
See id.
1167
Id. at § III(A).
1168
Id.
1169
Id.
1170
Id. at § V.
1171
Id. at § V(C).
1172
Id.
1173
Id. at § V(D).
1174
Id.
1175
This information was provided by the MLSPU.
1176
MLS Substance Abuse Policy, § X(A).
1177
See id. at § X(B) (providing different discipline scheme for players who have tested positive for PEDs).
1178
Id. at § X(A).
1179
Id.
1180
Id. at § X(A)(3).
1181
See id. at § X(A).
1182
Id. at § X (B).
1183
See id. at § VIII(D); § IX (B).
1184
See id. at § XII(B)(1).
1185
Id.
1186
Id.
1187
Id.
1188
For context, the NFL regular season is 16 games, the MLB regular season is 162 games, the NBA and NHL
regular seasons are 82 games, the CFL regular season is 18 games, and the MLS regular season is 34 games.
1189
2011 NBA CBA, Art. XXXIII, § 9(a).
1190
See 2017 NBA CBA, Art. XXXIII, § 1(b) (“A player may not Come Forward Voluntarily for the use of a SPED”).
1191
See 2017 NBA CBA, Art. XXXIII, § 9.
1192
See Alfhid Gronbladh, Erik Nylander, Mathias Halberg, The neurobiology and addiction potential of anabolic
androgenic steroids and the effects of growth hormone, 126 Brain Res. Bulletin 127, 129–30 (2016) (discussing PES
dependence); Harrison G. Pope et al., Adverse Health Consequences of Performance-Enhancing Drugs: An
Endocrine Society Specific Statement, 35 Endocrine Reviews 341, 355 (2013) (discussing PES dependence); Gen
Kanayama et al., Treatment of anabolic-androgenic steroid dependence: Emerging evidence and its implications, 109
Drug & Alcohol Dependence 6, 7 (2010) (“[PES usage] can cause a dependence syndrome where individuals may
use these drugs almost continuously for years, often despite adverse effects”); Gen Kanayama et al., Anabolic-
androgenic steroid dependence: an emerging disorder, 104 Addiction 12, 1966–78 (2009) (finding that About 30% of
anabolic steroid users appear to develop a dependence syndrome, characterized by chronic steroid use despite
adverse effects on physical, psychosocial, or occupational functioning).
1193
See Anders Hakansson et al., Anabolic androgenic steroids in the general population: user characteristics and
associations with substance use, 18 Eur. Addict Res. 2 (2012) (“[PED] use was most strongly associated with a
lifetime history of illicit drug use and the misuse of prescription drugs.”); Michael Bahrke et al., Risk factors associated
with anabolic-androgenic steroid use among adolescents, 29 Sports Med. 6 (2000) (“studies have reported that the
likelihood of using [PEDs] was associated with the use of several other drugs including marijuana, cocaine,
stimulants, relaxants, heroin, caffeine, alcohol, cigarettes and smokeless tobacco.”)
1194
Alfhid Gronbladh, Erik Nylander, Mathias Halberg, The neurobiology and addiction potential of anabolic
androgenic steroids and the effects of growth hormone, 126 Brain Res. Bulletin 127, 130 (2016) (“there is a strong
association between [PES] dependence and opioid dependence”); Harrison G. Pope et al., Adverse Health
Consequences of Performance-Enhancing Drugs: An Endocrine Society Specific Statement, 35 Endocrine Reviews
341, 348–49 (2013).
1195
Gen Kanayama et al., Treatment of anabolic-androgenic steroid dependence: Emerging evidence and its
implications, 109 Drug & Alcohol Dependence 6, 8–9 (2010).

!
268!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1196
Id. at 9.
1197
Harrison G. Pope et al., Adverse Health Consequences of Performance-Enhancing Drugs: An Endocrine Society
Specific Statement, 35 Endocrine Reviews 341, 348–49 (2013); Kanayama et al., supra n. 1195 at 10.
1198
Pope et al., supra n. 1197 at 353; Kanayama et al., supra n. 1195 at 10.
1199
See Daria Paicentino et al., Anabolic-androgenic Steroid Use and Psychopathology in Athletes. A Systematic
Review, 13 Current Neuropharmacology 101 (2015).
1200
Pope et al., supra n. 1197 at 348-49; Kanayama et al., supra n. 1195 at 10.
1201
Gronbladh, Nylander, Halberg, supra n. 1194 at 130; Pope et al., supra n. 1198 at 348-49.
1202
Pope et al., supra n. 1198 at 349; Kanayama et al., supra n. 1195 at 349.
1203
See Gronbladh, Nylander, Halberg, supra n. 1194 at 133-34; Pope et al., supra n. 1197 at 348-49; Kanayama et
al., supra n. 1195 at 10; Harrison G. Pope, MD, MPH, McLean Hospital,
http://www.mcleanhospital.org/biography/harrison-pope (last visited Dec. 15, 2016), archived at
https://perma.cc/EK4G-7MWU (“Harrison G. Pope, MD, MPH, has conducted research in a wide range of areas in
psychiatry and has authored more than 300 peer-reviewed papers. This work includes many publications on the
diagnosis and treatment of psychotic disorders and major mood disorders, together with extensive research on eating
disorders and related issues of body image in both women and men. More recently, Dr. Pope has also focused on
substance abuse disorders, with emphasis on drugs such as cannabis, hallucinogens, ecstasy, and anabolic-
androgenic steroids.”).
1204
In this Chapter, we are focused on the compensation structures of the players actually playing in the leagues, and
not on practice squad, minor league, or development league players. The structure of play and compensation for
players at these lower levels vary considerably across the leagues based on differing needs, and thus do not provide
for a useful comparison.
1205
See, e.g., Josh Alper, Sean Lee says it was his call to sit with $2 million on the line, ProFootballTalk (Jan. 4,
2016, 10:46 AM), http://profootballtalk.nbcsports.com/2016/01/04/sean-lee-says-it-was-his-call-to-sit-with-2-million-
on-the-line/, archived at https://perma.cc/69QS-FVPH.
1206
See Thomas Richardson, Peter Elliotta, & Ronald Roberts, The relationship between personal unsecured debt
and mental and physical health: A systematic review and meta-analysis, 33 Clinical Psychol. Rev. 8, 1148-62 (2013).
Many experts have recognized that “financial insecurity can cause people to ‘cut corners in ways that may affect their
health and well-being,’ like spending less on food, clothing, or prescriptions.” Nadia N. Sawicki, Modernizing Informed
Consent: Expanding the Boundaries of Materiality, Univ. Ill. L. Rev. (2016), citing Kevin R. Riggs, Peter A. Ubel,
Overcoming Barriers to Discussing Out-of-Pocket Costs With Patients, 174 Jama Int. Med. 849 (2014); Peter A. Ubel,
Amy P. Abernethy, S. Yousuf Zafar, Full Disclosure—Out-of-Pocket Costs as Side Effects, 369 New Eng. J. Med.
1484 (2013). Indeed, to many, “financial well-being is certainly within the boundaries of most peoples’ concept of
health.” Id., quoting Michael S. Wilkes & David L. Schriger, Caution: The Meter is Running: Informing Patients About
Health Care Costs, 165 Western J. Med. 74, 78 (1996) (noting that “discussions about the cost of care are an
important part of the physician-patient relationship”).
1207
See, e.g., Melissa B. Jacoby, Teresa A. Sullivan, Elizabeth Warren, Rethinking the Debates over Health Care
Financing: Evidence from the Bankruptcy Courts, 76 N.Y.U. L. Rev. 375 (2001) (empirical data demonstrating how
many American families declare bankruptcy in the aftermath of illness or other healthcare crisis); Christopher Tarver
Robertson, Richard Egelhof,Michael Hoke, Get Sick, Get Out: The Medical Causes of Home Mortgage Foreclosures,
18 Health Matrix 65 (2008) (empirically demonstrating and discussing the role that health crises have in home
foreclosures).
1208
For purposes of this Chapter, we define a “rookie” as any player who has not yet played and a veteran as any
player who has played.
1209
See, e.g., 2011 NFL CBA, Art. 1 (“‘Salary Cap‘ means the absolute maximum amount of Salary that each Club
may pay or be obligated to pay or provide to players… at any time during a particular League Year“); 2017 NBA CBA,
Art. 1, § 1(mmm) (“‘Salary Cap’ means the maximum allowable Team Salary for each Team for a Salary Cap Year,
subject to the rules and exceptions set forth in [the CBA]”).
1210
The National League had begun play in 1876 and the American League in 1901. MLB was the result of a merger
between the two leagues.
1211
Joshua P. Jones, A Congressional Swing and Miss: The Curt Flood Act, Player Control, and the National
Pastime, 33 Ga. L. Rev. 639, 642 (1999).
1212
Id.
1213
See American Needle, Inc. v. Nat’l Football League, 560 U.S. 183, 186 (2010), citing 15 U.S.C. § 1.
1214
Fed. Baseball Club of Balt., Inc. v. Nat’l League of Prof’l Baseball Clubs, 259 U.S. 200 (1922).
1215
See Nathaniel Grow, Defining the “Business of Baseball”: A Proposed Framework for Determining the Scope of
Professional Baseball’s Antitrust Exemption, 44 U.C. Davis L. Rev. 557, 566 (2010).
1216
See Toolson v. N.Y. Yankees, 346 U.S. 356 (1953).
1217
See Flood v. Kuhn, 407 U.S. 258 (1972).
1218
Stare decisis is Latin for “to stand by things decided.” It is “[t]he doctrine of precedent, under which a court must
follow earlier judicial decisions when the same points arise again in litigation.” BLACK’S LAW DICTIONARY (9th ed. 2009).

!
269!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1219
See id. at 284.
1220
Indeed, in 1998 Congress passed the Curt Flood Act, named for the plaintiff in the 1972 Supreme Court case,
which substantially overruled Federal Baseball and its progeny by declaring that actions relating to the employment of
Major League Baseball players are subject to antitrust law. However, the Act kept Major League Baseball’s antitrust
immunity concerning its handling of minor league baseball and franchise issues, such as relocation. See 15 U.S.C. §
26b; City of San Jose v. Office of the Comm’r of Baseball, 776 F.3d 686 (9th Cir. 2015).
1221
In Radovich v. Nat’l Football League, 352 U.S. 445 (1957), the Supreme Court held that the NFL was not exempt
from the antitrust laws. In Haywood v. Nat’l Basketball Ass’n, 401 U.S. 1204 (1971), the Supreme Court held that the
NBA was not exempt from the antitrust laws. Lower courts have subsequently refused to extend baseball’s antitrust
exemption to professional hockey, Phila. World Hockey Club, Inc. v. Phila. Hockey Club, Inc., 351 F. Supp. 462, 466
n.3 (E.D. Pa. 1972); professional golf, Blalock v. Ladies Prof’l Golf Ass’n, 359 F. Supp. 1260, 1263 (N.D. Ga. 1973);
and professional tennis, Gunter Harz Sports, Inc. v. U.S. Tennis Ass’n, 665 F.2d 222, 223 (8th Cir. 1981).
1222
See Chris Deubert & Glenn M. Wong, Understanding the Evolution of Signing Bonuses and Guaranteed Money
in the National Football League: Preparing for the 2011 Collective Bargaining Negotiations, 16 UCLA Ent. L. Rev.
179, 187 (2009) (describing the various legal proceedings leading to free agency in those sports).
1223
After the 1974 season, Los Angeles Dodgers pitcher Andy Messersmith refused to sign the contract presented to
him by the Dodgers. The club exercised its options under the reserve clause and Messersmith played the 1975
season without an executed contract. After the season, Messersmith claimed that he had played out the option year
of the contract and was now a free agent, able to sign with any club he chose. An arbitrator ultimately sided with
Messersmith. Joshua P. Jones, A Congressional Swing and Miss: The Curt Flood Act, Player Control, and the
National Pastime, 33 GA. L. REV. 639, 659-60 (1999). The arbitrator’s decision was affirmed in federal court. Kansas
City Royals Baseball Corp. v. Major League Baseball Players Ass’n, 409 F. Supp. 233 (W.D. Mo. 1976) aff’d, 532
F.2d 615 (8th Cir. 1976).
1224
See Glenn M. Wong, Essentials of Sports Law, Exs. 11.3–11.6 (4th ed. 2010) (providing CBA history for each of
the Big Four leagues).
1225
See Chris Deubert, Glenn M. Wong, John Howe, All Four Quarters: A Retrospective and Analysis of the 2011
Collective Bargaining Process and Agreement in the National Football League, 19 UCLA Ent. L. Rev. 1, 9–12 (2012)
(discussing NFL-NFLPA labor relations between 1987 and 1993).
1226
The NFL currently has television broadcasting agreements with ESPN, NBC, CBS, FOX, NFL Network and
DirecTV. In addition, the NFL has a radio broadcasting agreement with Westwood One. In total, the broadcasting
agreements bring in approximately $7 billion in annual revenue to the NFL. Kurt Badenhausen, The NFL Signs TV
Deals Worth $27 Billion, Forbes (Feb. 14, 2011, 6:13PM),
http://www.forbes.com/sites/kurtbadenhausen/2011/12/14/the-nfl-signs-tv-deals-worth-26-billion/, archived at
http://perma.cc/8PXK-2VNU.
1227
NFL Ventures is responsible for negotiating all of the league’s major sponsorship, marketing, and media rights
deals. NFL Ventures, which Commissioner Goodell ran before becoming Commissioner, includes four wholly-owned
subsidiaries: NFL Enterprises, NFL Properties, NFL Productions, and NFL International. See Tommy Craggs,
Exclusive: Leaked Documents Show Operating Profits for NFL Ventures Rose 29 Percent Last Year, Deadspin (July
15, 2011, 1:10 PM), http://deadspin.com/5821386/audited-financials-operating-profit-for-nfl-ventures-lp-rose-from-
999-million-to-13-billion-last-year, archived at http://perma.cc/3MNZ-XHLU.
1228
NFL Network is the league-owned and operated television network devoted full-time to the NFL, including
broadcasting select Thursday night games. For more information, see www.nfl.com/nflnetwork.
1229
NFL Properties is responsible for licensing, sponsorship, and marketing. NFL Properties was the subject of Am.
Needle, Inc. v. Nat’l Football League, 560 U.S. 183 (2010). NFL Properties was created by the 32 individual clubs to
collectively market and license the clubs’ individual intellectual property, such as names, colors, logos, and
trademarks. In 2000, the clubs—through NFL Properties—granted Reebok an exclusive license to produce and sell
trademarked headwear for the 32 clubs. American Needle—a former licensee and creator of NFL appareled
headwear—could no longer create headwear with NFL logos and trademarks. American Needle challenged the
exclusive license as an illegal restraint of trade by the 32 NFL clubs. The Northern District of Illinois granted the NFL
summary judgment after finding that NFL Properties constituted a single entity for antitrust purposes, and therefore
there was no contract, combination, or conspiracy to restrain trade. See Am. Needle, Inc. v. New Orleans La. Saints,
496 F. Supp. 2d 941, 943 (N.D. Ill. 2007). The Seventh Circuit affirmed. Am. Needle, Inc. v. Nat’l Football League,
538 F. 3d 736 (7th Cir. 2008). The Supreme Court reversed. Am. Needle, 560 U.S. 183. While the Court noted that
NFL clubs “depend upon a degree of cooperation for economic survival,” the necessity of cooperation does not
transform concerted action into the independent action of a single entity. Id. at 198. Furthermore, that “even if league-
wide agreements are necessary to produce football, it does not follow that concerted activity in marketing intellectual
property is necessary to produce football.” Id. at n.7.
1230
NFL Enterprises is responsible for advertising, publicizing, promoting, marketing, and selling broadcasts of NFL
games.
1231
NFL Productions, also known as NFL Films, is the league-owned film company that for over 50 years has
produced award-winning films about the NFL. For more information see www.nflfilms.com.

!
270!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1232
NFL Digital is responsible for the league’s technology and new media ventures, including www.nfl.com and NFL
Mobile.
1233
2011 NFL CBA, Art. 12, § 6.
1234
2011 NFL CBA, Art. 12, §1, § 6.
1235
Mike Florio, NFL will reach $14 billion in 2017 revenue, ProFootballTalk (Mar. 6, 2017, 11:29 AM),
http://profootballtalk.nbcsports.com/2017/03/06/nfl-will-reach-14-billion-in-2017-revenue/, archived at
https://perma.cc/X57A-VRXU.
1236
2011 NFL CBA, art. 12, § 6(c)(ii).
1237
2011 NFL CBA, Art. 12, § 6(c)(i).
1238
2011 NFL CBA, Art. 1.
1239
2011 NFL CBA, Art. 12, § 2.
1240
2011 NFL CBA, Art. 12, § 6(c)(v).
1241
2016 Adjusted Team Salary Caps, NFLPA (Mar. 7, 2016), https://www.nflpa.com/news/all-news/2016-adjusted-
team-salary-caps, archived at https://perma.cc/K9GZ-ZDGN.
1242
Josh Alper, Salary cap set at $167 million, ProFootballTalk (Mar. 1, 2017, 11:12 AM),
http://profootballtalk.nbcsports.com/2017/03/01/salary-cap-set-at-167-million/, archived at https://perma.cc/7W45-
ERVP.
1243
In reality, the NFL Salary Cap does permit for one exception for veteran players playing for the minimum salary.
Players with at least four Credited Seasons who sign for the league minimum will only have their salary count against
the Salary Cap as if the player only had two Credited Seasons. 2011 NFL CBA, Art. 27. This exception discourages
clubs from hiring younger players over experienced veterans simply because they are younger. Also, each club’s
Salary Cap is uniquely based upon whether certain incentives were earned by the club’s players in the previous
season. 2011 NFL CBA, Art. 13, § 6(c)(ii–iii).
1244
2011 NFL CBA, Art. 12, § 9(a).
1245
2011 NFL CBA, Art. 12, § 8(b).
1246
Chris Deubert & Glenn Wong, All Four Quarters: A Retrospective And Analysis Of The 2011 Collective
Bargaining Process And Agreement In The National Football League, 19 UCLA Ent. L. Rev. 1, 52 (2012), citing Rams
Give Bradford 50M Guaranteed, ESPN (July 31, 2010, 9:09 AM),
http://sports.espn.go.com/nfl/news/story?id=5425041, archived at http://perma.cc/BZW8-GNTH.
1247
Chris Deubert & Glenn Wong, All Four Quarters: A Retrospective And Analysis Of The 2011 Collective
Bargaining Process And Agreement In The National Football League, 19 UCLA Ent. L. Rev. 1, 52 (2012), citing Tom
Brady Signs Extension, ESPN (Sept. 11, 2010, 3:13 PM), http://
sports.espn.go.com/boston/nfl/news/story?id=5552561, archived at http://perma.cc/X69A-2G33.
1248
See Chris Deubert & Glenn Wong, All Four Quarters: A Retrospective And Analysis Of The 2011 Collective
Bargaining Process And Agreement In The National Football League, 19 UCLA Ent. L. Rev. 1, 52–60 (2012)
(discussing changes to rookie compensation as part of 2011 CBA).
1249
2011 NFL CBA, Art. 7 § 3(a).
1250
Id.
1251
Id.
1252
2011 NFL CBA, Art. 7, § 1(e).
1253
See Chris Deubert & Glenn Wong, All Four Quarters: A Retrospective And Analysis Of The 2011 Collective
Bargaining Process And Agreement In The National Football League, 19 UCLA Ent. L. Rev. 1, 58–60 (2012). The
formula for calculating the Total Rookie Allocation and each player’s portion of the Total Rookie Allocation are
intended to be secret to provide the clubs and players a range within which to negotiate a contract. However, prior to
the 2011 League Year, an NFLPA employee inadvertently sent to all contract advisors the 2011 Total Rookie
Allocations for each club, including for each drafted player. Consequently, all of the contract advisors and clubs knew
the total amount of compensation each rookie was to receive. Additionally, the Salary Cap and Total Rookie
Allocation increase by the same percentage each year. Thus, contract advisors and clubs can easily determine a
drafted player’s share of the Total Rookie Allocation by examining the 2011 Total Rookie Allocations and increasing
them the same percentage as the Salary Cap increased each year (a figure that is made public). Id.
1254
See 2011 CBA, Art. 7 § 3(e) (prohibiting “option bonuses, option exercise fees, option nonexercise fees, Salary
Advances ... voidable year(s) provisions, buybacks of voidable year(s) provisions, and any ‘contract within the
contract’ (i.e. terms and conditions of a contemplated superseding contract within the Rookie Contract).”); Chris
Deubert & Glenn Wong, All Four Quarters: A Retrospective And Analysis Of The 2011 Collective Bargaining Process
And Agreement In The National Football League, 19 UCLA Ent. L. Rev. 1, 52–60 (2012) (discussing changes to
rookie compensation as part of 2011 CBA).
1255
See Chris Deubert & Glenn Wong, All Four Quarters: A Retrospective And Analysis Of The 2011 Collective
Bargaining Process And Agreement In The National Football League, 19 UCLA Ent. L. Rev. 1, 60–61 (2012).
1256
Id. at 57–58. The Performance Incentive theoretically has the possibility of players risking injury to reach the
playtime threshold necessary to earn the bonus. While this possibility exists, it is only one of many pressures that

!
271!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
players feel to continue playing. Additionally, players are generally unlikely to know their cumulative playtime
percentages during the season.
1257
Michael David Smith, Jared Goff expected to sign with Rams today, ProFootballTalk (June 9, 2016, 10:00 AM),
http://profootballtalk.nbcsports.com/2016/06/09/jared-goff-expected-to-sign-with-rams-today/, archived at
https://perma.cc/3JBL-LSUY.
1258
Kalan Reed, Spotrac, http://www.spotrac.com/nfl/tennessee-titans/kalan-reed/ (last visited June 23, 2016),
archived at http://perma.cc/BY5K-PJ94.
1259
Id.
1260
2011 NFL CBA, Art. 8, § 1.
1261
Id.
1262
2011 NFL CBA, Art 1.
1263
2011 NFL CBA, Art. 8, § 2.
1264
For context, 2,274 players played in at least one NFL game in 2016. This statistic is derived from official NFL-
NFLPA playtime statistics.
1265
Weston Hodkiewicz, Safety Banjo re-signs, Green Bay Press-Gazette, Apr. 18, 2015, available at 2015 WLNR
11354235.
1266
2011 NFL CBA, Art. 9, § 2.
1267
See id.
1268
Curtis Crabtree, Jermaine Kearse signs restricted free agent tender with Seahawks, ProFootballTalk (May 5,
2015, 11:42 PM), http://profootballtalk.nbcsports.com/2015/05/05/jermaine-kearse-signs-restricted-free-agent-tender-
with-seahawks/, archived at http://perma.cc/N78Z-ZJAM.
1269
2011 NFL CBA, Art. 1 (“‘Unrestricted Free Agent‘ means a Veteran with four or more Accrued Seasons, who has
completed performance of his Player Contract”); 2011 CBA, Art. 8, § 1 (“a player shall receive one Accrued Season
for each season during which he was on, or should have been on, full pay status for a total of six or more regular
season games”).
1270
2011 NFL CBA, Art. 9, § 1(a).
1271
See James Walker, Breaking down Ndamukong Suh’s record-setting contract, ESPN, Mar. 12, 2015,
http://espn.go.com/blog/nflnation/post/_/id/163930/breaking-down-ndamukong-suhs-record-setting-contract, archived
at http://perma.cc/GD65-SFMV.
1272
2011 NFL CBA, Art. 9 § 2(b).
1273
For example, in 2015, former Detroit Lion Ndamukong Suh signed a six-year deal with the Miami Dolphins for
$114 million, $60 million of which was guaranteed. Josh Alper, Dolphins make it official with Ndamukong Suh,
ProFootballTalk (Mar. 11, 2015, 4:14 PM), http://profootballtalk.nbcsports.com/2015/03/11/dolphins-make-it-official-
with-ndamukong-suh/, archived at http://perma.cc/2T5Z-367S.
1274
See Chris Deubert & Glenn M. Wong, Understanding the Evolution of Signing Bonuses and Guaranteed Money
in the National Football League: Preparing for the 2011 Collective Bargaining Negotiations, 16 UCLA Ent. L. Rev.
179, 190–97 (2009) (discussing the different types of bonuses common in NFL player contracts).
1275
See 2011 NFL CBA, Art. 13, § 6(c) (listing incentives permitted to be included in NFL players).
1276
For example, in 2014, two years before he would have been eligible for free agency, J.J. Watt signed a six-year
contract extension with the Houston Texans for $100 million, $51.8 million of which was guaranteed. Texans give J.J.
Watt $100M deal, ESPN, Sept. 2, 2014, http://espn.go.com/nfl/story/_/id/11451373/jj-watt-houston-texans-reach-
agreement-6-year-100-million-deal, archived at http://perma.cc/GUQ4-GP9J.
1277
See Bert Bell/Pete Rozelle NFL Player Retirement Plan (Apr. 1, 2012) § 1.11 (defining “Credited Season“); 2011
NFL CBA, Art. 26, § 2 (same).
1278
Credited Seasons are particularly important when it comes to NFL players’ eligibility for health-related benefits, as
discussed in Chapter 3: Health-Related Benefits.
1279
Gregg Rosenthal, Winners, Losers from the NFL Lockout, ProFootballTalk (July 25, 2011, 3:15 PM),
http://profootballtalk.nbcsports.com/2011/07/25/winners-losers-from-the-nfl-lockout/, archived at
http://perma.cc/FB28-XHSF.
1280
2011 NFL CBA, Art. 13, § 6(b)(i).
1281
Id.
1282
See James Walker, Breaking down Ndamukong Suh’s record-setting contract, ESPN, Mar. 12, 2015,
http://espn.go.com/blog/nflnation/post/_/id/163930/breaking-down-ndamukong-suhs-record-setting-contract, archived
at http://perma.cc/GD65-SFMV.
1283
See Sally Jenkins, NFL’s concussion priorities: Dodging blame, making players responsible, Wash. Post, Dec. 3,
2015, https://www.washingtonpost.com/sports/redskins/nfls-concussion-priorities-dodging-blame-making-players-
responsible/2015/12/03/1b8752f8-99d2-11e5-94f0-9eeaff906ef3_story.html, archived at https://perma.cc/JT6P-JX44
(“The heart of the NFL’s concussion problem is not that players hide symptoms; it’s a compensation structure that
forces them to play hurt, or get cut.”)
1284
See 2011 NFL CBA, App. H. Notice of Termination; see also id., at Art. 4 §5(d).

!
272!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1285
See Chris Deubert & Glenn M. Wong, Understanding the Evolution of Signing Bonuses and Guaranteed Money
in the National Football League: Preparing for the 2011 Collective Bargaining Negotiations, 16 UCLA Ent. L. Rev. 179
(2009) (describing the various forms of guaranteed compensation in the NFL).
1286
Where a player is injured in one season, fails the pre-season physical the next season because of that injury, and
is terminated by the club as a result, the player is entitled to 50% of his salary for that season up to a maximum of
$1.1 million in the 2015 season. If the player is still physically unable to play two seasons after the injury, he is
entitled to 30% of his salary up to a maximum for $525,000 in 2015. A player is only entitled to Injury Protection once
in his career. See 2011 NFL CBA, Art. 45.
1287
A player with at least four years of experience who has his contract terminated after the first game of the season
is entitled to the remainder of his salary for that season once in his career. 2011 NFL CBA, Art. 30.
1288
See Mike Florio, The full Kaepernick contract details, ProFootballTalk (Jun. 5, 2014, 12:46 AM),
http://profootballtalk.nbcsports.com/2014/06/05/the-full-kaepernick-contract-details/, archived at
http://perma.cc/B6W9-WVC7 (discussing details of Colin Kaepernick’s 2014 contract with the San Francisco 49ers.
Despite reports that Kaepernick had received $61 million guaranteed, only about $13 million was guaranteed against
skill, injury, and Salary Cap).
1289
See Chris Deubert, Glenn M. Wong, John Howe, All Four Quarters: A Retrospective and Analysis of the 2011
Collective Bargaining Process and Agreement in the National Football League, 19 UCLA Ent. L. Rev. 1, 61–63 (2012)
(discussing the movement towards more guaranteed compensation). In 2012, Peyton Manning signed a five-year
deal with the Denver Broncos for $96 million, $58 million of which was guaranteed. Mike Klis & Jeff Legwold, Peyton
Manning’s $96 million deal with Broncos includes neck injury clause, Denver Post, Mar. 20, 2012,
http://www.denverpost.com/ci_20213659/peyton-mannings-deal-broncos-5-years-96-million, archived at
http://perma.cc/4GMF-C92W. In 2014, J.J. Watt signed a six-year deal with the Houston Texans for $100 million,
$51.8 million of which was guaranteed. Texans give J.J. Watt $100M deal, ESPN, Sept. 2, 2014,
http://espn.go.com/nfl/story/_/id/11451373/jj-watt-houston-texans-reach-agreement-6-year-100-million-deal, archived
at http://perma.cc/GUQ4-GP9J. And, in 2015, Ndamukong Suh signed a six-year deal with the Miami Dolphins for
$114 million, $60 million of which was guaranteed. Josh Alper, Dolphins make it official with Ndamukong Suh,
ProFootballTalk (Mar. 11, 2015, 4:14 PM), http://profootballtalk.nbcsports.com/2015/03/11/dolphins-make-it-official-
with-ndamukong-suh/, archived at http://perma.cc/2T5Z-367S.
1290
See Chris Deubert, Glenn M. Wong, John Howe, All Four Quarters: A Retrospective and Analysis of the 2011
Collective Bargaining Process and Agreement in the National Football League, 19 UCLA Ent. L. Rev. 1, 52–61 (2012)
(discussing changes to rookie compensation scheme).
1291
Id.
1292
The Substance Abuse Policy and PES Policy are discussed at length in Chapter 4: Drug and Performance-
Enhancing Substance Policies.
1293
See 2011 NFL CBA, Art. 4, § 9. See also Chris Deubert, Glenn M. Wong, John Howe, All Four Quarters: A
Retrospective and Analysis of the 2011 Collective Bargaining Process and Agreement in the National Football
League, 19 UCLA Ent. L. Rev. 1, 48–51 (2012) discussing clubs’ efforts to recoup portions of bonus money already
paid to players); Chris Deubert & Glenn M. Wong, Understanding the Evolution of Signing Bonuses and Guaranteed
Money in the National Football League: Preparing for the 2011 Collective Bargaining Negotiations, 16 UCLA Ent. L.
Rev. 179, 202-26 (2009) (same).
1294
See Chris Deubert & Glenn M. Wong, Understanding the Evolution of Signing Bonuses and Guaranteed Money
in the National Football League: Preparing for the 2011 Collective Bargaining Negotiations, 16 UCLA Ent. L. Rev.
179, 194-95 (2009) (same).
1295
See 2011 NFL CBA, At. 4, § 9(g) (discussing voiding of guarantees).
1296
2012 MLB CBA, Art. XXIII § B(2)
1297
! MLBPA, MLB Announce Details of New Labor Agreement, MLBPA (Dec. 2, 2016),
http://www.mlbplayers.com/ViewArticle.dbml?DB_OEM_ID=34000&ATCLID=211336390, archived at
https://perma.cc/4XUA-2DAW.!
1298
MLBPA, MLB Announce Details of New Labor Agreement, MLBPA (Dec. 2, 2016),
http://www.mlbplayers.com/ViewArticle.dbml?DB_OEM_ID=34000&ATCLID=211336390, archived at
https://perma.cc/4XUA-2DAW.
1299
Maury Brown, MLB Sees Record Revenues Approaching $10 Billion for 2016, Forbes (Dec. 5, 2016, 3:22 PM),
http://www.forbes.com/sites/maurybrown/2016/12/05/mlb-sees-record-revenues-approaching-10-billion-for-
2016/#7704e2e21845, archived at https://perma.cc/775E-WE9A.
1300
Theoretically, a player could execute a long-term contract with the club before his rookie season that provides for
greater pay in the rookie season, but such contracts are extremely rare. See Craig Calcaterra, At Least One Major
Leaguer is Not Pleased With the Jon Singleton Deal, HARDBALL TALK (June 3, 2014, 8:55 AM),
http://mlb.nbcsports.com/2014/06/03/at-least-one-major-leaguer-is-not-pleased-with-the-jon-singleton-deal/, archived
at https://perma.cc/2BPJ-YCHU.
1301
2012 MLB CBA Art. XXI(A)(1).

!
273!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1302
UPC ¶¶ 10(a), (b).
1303
Jeff Monhait, Baseball Arbitration: An ADR Success, 4 Harv. J. Sports & Ent. L. 105, 107 (2013). These players
could be considered “Exclusive Rights Players” per the definition we provided in the Introduction to this Chapter.
1304
Ed Edmonds, A Most Interesting Part of Baseball’s Monetary Structure—Salary Arbitration in Its Thirty-Fifth Year,
20 Marq. Sports L. Rev. 1, 7 (2009).
1305
See 2012 MLB CBA, Art. VI(E)(1)(a).
1306
2012 MLB CBA, Art. VI(E)(1)(b).
1307
Id.
1308
2012 MLB CBA, Art. VI(E)(4).
1309
2012 MLB CBA, Art. VI(E)(5). The salary arbitration panel is distinct from the arbitration panel used to hear
ordinary grievances under the CBA.
1310
2012 MLB CBA, Art. VI(E)(7).
1311
Id. The criteria to be used in determining the player’s salary include “the quality of the Player’s contribution to his
club during the past season (including but not limited to his overall performance, special qualities of leadership and
public appeal), the length and consistency of his career contribution, the record of the Player’s past compensation,
comparative baseball salaries… , the existence of any physical or mental defects on the part of the Player, and the
recent performance record of the Club including but not limited to its League standing and attendance as an
indication of public acceptance.” Id. at Art. VI, § E(10).
1312
Id., at Art. VI(E)(13).
1313
See Eldon L. Ham & Jeffrey Malach, Hardball Free Agency – The Unintended Demise of Salary Arbitration in
Major League Baseball: How the Law of Unintended Consequences Crippled the Salary Arbitration Remedy – And
How to Fix It, 11 Harv. J. Sports & Ent. L. 63 (2010).
1314
MLBPA Info - Frequently Asked Questions, MLB Players, http://mlb.mlb.com/pa/info/faq.jsp#minimum (last visited
Aug. 27, 2015), archived at http://perma.cc/92LP-4YYP.
1315
2012 MLB CBA, Art. XX(B)(1). These players could be considered “Unrestricted Free Agents” per the definition
we provided in the Introduction to this Chapter. MLB does not have Restricted Free Agents.
1316
Katie Stankiewicz, Length of Contracts and the Effect on the Performance of MLB Players, 17 Park Place
Economist 76, 76–78 (2009), https://www.iwu.edu/economics/PPE17/stankiewicz.pdf, archived at
http://perma.cc/M5CG-W6EY (surveying the related economics literature).
1317
Id.
1318
Jeff Todd, Free Agent Contract Trends: 2007–08 To Present, MLB Trade Rumors, Jan. 31, 2014,
http://www.mlbtraderumors.com/2014/01/free-agent-contract-trends-2007-08-to-present.html, archived at
http://perma.cc/4MWY-SU29.
1319
Id.
1320
Jayson Stark, Stanton Wanted Flexibility for Marlins, ESPN, Nov. 18, 2014,
http://espn.go.com/mlb/story/_/id/11897600/giancarlo-stanton-325m-miami-marlins-heavily-backloaded, archived at
http://perma.cc/VE7R-TWSS.
1321
Jason Beck, Tigers Announce Record Extension for Miggy, Major League Baseball, Mar. 28, 2014,
http://m.tigers.mlb.com/news/article/70257040/detroit-tigers-announce-eight-year-extension-for-miguel-cabrera,
archived at http://perma.cc/MD5W-ANBB.
1322
Cliff Corcoran, Don’t blame Cubs for taking advantage of rules with Kris Bryant, Sports Illustrated, Mar. 18, 2015,
http://www.si.com/mlb/2015/03/18/chicago-cubs-kris-bryant-scott-boras-theo-epstein-service-time, archived at
http://perma.cc/KQ73-2BKX; C.J. Nitkowski, Kris Bryant and the Service-Time Game, Fox Sports,
http://www.foxsports.com/mlb/just-a-bit-outside/story/chicago-cubs-kris-bryant-service-time-when-to-call-up-
prospects-031115 (last visited Aug. 27, 2015), archived at http://perma.cc/P9ER-99TV.
1323
Corcoran, supra n. 1322; Nitkowski, supra n. 1322. Jesse Rogers, Kris Bryant, to hit cleanup in major league
debut, ESPN, Apr. 17, 2015, http://espn.go.com/chicago/mlb/story/_/id/12705857/chicago-cubs-call-kris-bryant,
archived at http://perma.cc/WJ9M-2642.
1324
Corcoran, supra n. 1322; Nitkowski, supra n. 1322; Rogers, supra n. 1323.
1325
Id.
1326
See Ben Nicholson-Smith, Recent Extensions For Pre-Arb Eligible Players, MLB Trade Rumors, Apr. 10, 2012,
http://www.mlbtraderumors.com/2012/04/recent-extensions-for-pre-arbitration-eligible-players.html, archived at
http://perma.cc/5LVR-D26Y; Ken Rosenthal, More extensions, less free agency, Fox Sports (May 17, 2013, 4:01
PM), https://web.archive.org/web/20130921021255/http://msn.foxsports.com/mlb/story/more-contract-extensions-
less-free-agency-robinson-cano-justin-verlander-joey-votto-felix-hernandez-kyle-lohse-051613, archived at
https://perma.cc/88CH-HG57.
1327
Bill Brink & Michael Sanserino, Pirates, McCutchen agree on new contract, Mar. 5, 2012, Pittsburgh Post-
Gazette, http://www.post-gazette.com/sports/pirates/2012/03/05/Pirates-McCutchen-agree-on-new-
contract/stories/201203050213, archived at http://perma.cc/7XYD-6UFE.

!
274!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1328
Bob Nightengale, 2016 MLB salaries: Royals way pays, while average salary hits $4.4 million, USA Today, Apr.
4, 2016, http://www.usatoday.com/story/sports/mlb/2016/04/03/2016-mlb-salaries-payrolls/82592542/, archived at
https://perma.cc/PK6Y-BP4B.
1329
See 2012 MLB CBA, Art. VI(A)(1) (setting minimum salary at $500,000 plus cost of living adjustment); MLB
minimum salary remains at $507,500 for 2016, ESPN.com (Nov. 18, 2015),
http://espn.go.com/mlb/story/_/id/14161690/mlb-minimum-salary-remains-507500-2016, archived at
https://perma.cc/A73N-E7U7.
1330
For context, approximately 1,375 players played in an MLB regular season game in 2016.
1331
Barry Krissoff, Society and Baseball Facing Rising Income Inequality, Soc’y for Am. Baseball Res. (Spring 2013),
http://sabr.org/research/society-and-baseball-face-rising-income-inequality, archived at http://perma.cc/AHU7-KPX8.
1332
See Jordan I. Kobritz, Jeffrey F. Levine, Steven C. Palmer, Don Fehr Trades His Ball for a Puck: Will He
Continue to Score? 19 Vill. Sports & Ent. L.J. 521, 531 (2012) (describing contracts in MLB as “guaranteed”); Joseph
P. Kahn, Are long baseball contracts worth it?, Bos. Globe, Apr. 5, 2015, available at 2015 WLNR 9933513 (same).
1333
2017 NBA CBA, Art. XXXIX, § 2.
1334
2017 NBA CBA, Art. VII, § 12(b)(3).
1335
2017 NBA CBA Art. VII, § 1(a).
1336
2017 NBA CBA, Art. VII, § 2(a).
1337
NBA salary cap for 2016-17 set at $94.143 million, NBA (Jul. 2, 2016, 6:46 PM),
http://www.nba.com/2016/news/07/02/nba-salary-cap-set/, archived at https://perma.cc/PA8P-6JTP.
1338
Dan Feldman, Report: NBA’s 2017-18 Salary-Cap Projection Falls to $102 Million, Pro Basketball Talk (Feb. 3,
2017, 10:00 PM), http://nba.nbcsports.com/2017/02/03/report-nbas-2017-18-salary-cap-projection-falls-to-102-
million/, archived at https://perma.cc/U99B-MT4C.
1339
Dan Feldman, Report: NBA Projects Salary Cap to Reach $92 Million Next Season, Pro Basketball Talk (Apr. 18,
2016, 12:12 PM), http://nba.nbcsports.com/2016/04/18/report-nba-projects-salary-cap-to-reach-92-million-next-
season/, archived at https://perma.cc/D6T2-37UR.
1340
2017 NBA CBA Art. VII § 2(b).
1341
Dan Feldman, Report: NBA Revenue Projected to Reach $8 Billion Next Season, Pro Basketball Talk (Sep. 16,
2016, 10:05 AM), http://nba.nbcsports.com/2016/09/16/report-nba-revenue-projected-to-reach-8-billion-next-season/,
archived at https://perma.cc/73NP-QRJN.
1342
NBA salary cap for 2016-17 set at $94.143 million, NBA (Jul. 2, 2016, 6:46 PM),
http://www.nba.com/2016/news/07/02/nba-salary-cap-set/, archived at https://perma.cc/PA8P-6JTP.
1343
See Feldman, supra n. 1341.
1344
2017 NBA CBA, Art. VII, § 12(f)(1)(i).
1345
Id.
1346
2017 NBA CBA, Art. VII, § 12(g).
1347
Marc Stein, Money well spent: Cavs owe $54M in luxury taxes, sources say, ESPN (Jul. 3, 2016),
http://www.espn.com/nba/story/_/id/16719485/cleveland-cavaliers-owe-54-million-luxury-taxes, archived at
https://perma.cc/TVU2-TEDU.
1348
2017 NBA CBA Art. I § 1(jjj).
1349
2017 NBA CBA, Art. VIII § 1(a).
1350
Id.
1351
2017 NBA CBA, Ex. B.
1352
See Larry Coons, Larry Coon’s NBA Salary Cap FAQ, CBA FAQ, http://www.cbafaq.com/salarycap.htm (last
visited Feb. 2, 2017), archived at http://perma.cc/K9XV-FRTE.
1353
See id.
1354
See NBA 2014 Draft Tracker, Spotrac, http://www.spotrac.com/nba/draft/2016/ (last visited Feb. 2, 2017),
archived at https://perma.cc/2KAS-MUKA (providing contract details for 2016 NBA Draft picks).
1355
See 2017 NBA CBA, Art. XI, § 1(a).
1356
See id.; see also Larry Coons, Larry Coon’s NBA Salary Cap FAQ, CBA FAQ,
http://www.cbafaq.com/salarycap.htm (last visited Feb. 2, 2017), archived at http://perma.cc/K9XV-FRTE.
1357
See 2017 NBA CBA, Art. XI, § 1 (describing the circumstances under which a player become a Restricted Free
Agent); 2017 NBA CBA, Art. 1, § 1(hhhh) (“‘Veteran Free Agent‘ means a Veteran who completed his Player
Contract (other than a 10-Day Contract) by rendering the playing services called for thereunder.”)
1358
In the case of first round draft picks, the player would only become a restricted free agent if the club did not
exercise its option to extend his rookie contract for the next season.
1359
2017 NBA CBA, Art. XI, § 1.
1360
See 2017 NBA CBA Art. XI, § 1(c).
1361
2017 NBA CBA, Art. XI § 1(a)(ii).
1362
2017 NBA CBA, Art. XI, § 5 (b).
1363
2017 NBA CBA, Art. XI, § 5(g).
1364
Id.

!
275!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1365
See 2017 NBA CBA, Art. VII, § 6.
1366
CBA 101, Nat’l Basketball Ass’n, http://www.nba.com/media/CBA101.pdf, archived at http://perma.cc/VH8S-
9W55, at 5–8.
1367
The exception is named for Boston Celtics legend Larry Bird as the rule is believed to have been created to help
the Celtics resign Larry Bird in 1983, even though they never actually had to use the exception on Bird. Larry Coons,
Larry Coon’s NBA Salary Cap FAQ, CBA FAQ, http://www.cbafaq.com/salarycap.htm (last visited Feb. 21, 2017),
archived at http://perma.cc/K9XV-FRTE.
1368
The NFL Salary Cap does permit for one exception for veteran players playing for the minimum salary. Players
with at least four Credited Seasons who sign for the league minimum will only have their salary count against the
Salary Cap as if the player only had two Credited Seasons. 2011 NFL CBA, Art. 27. This exception avoids clubs from
hiring younger players over experienced veterans simply because they are younger.
1369
See 2017 NBA CBA, Exhibit C.
1370
See id.
1371
A player is credited with a year of service for each year that he is on an NBA roster for at least one day during the
regular season. 2017 NBA CBA, Art. I(iiii).
1372
2017 NBA CBA, Art. II § 7(a)(i).
1373
Id.
1374
See 2017 NBA CBA, Art. II § 7(a)(ii).
1375
See 2017 NBA CBA, Art. II § 7(a)(iii).
1376
2017 NBA CBA, Art. II, § 7(a)(ii).
1377
Brian Windhorst & Marc Stein, Sources: Warriors’ Stephen Curry stands to benefit in new CBA, ESPN (Dec. 15,
2016), http://www.espn.com/nba/story/_/id/18286141/under-new-cba-golden-state-warriors-guard-stephen-curry-get-
deal-worth-more-200-million, archived at https://perma.cc/8X9D-2LBK.
1378
We rely on information from the NBA and spotrac.com in making this estimate. Spotrac.com, as of March 2017,
maintained a database of 446 player contracts (including some partial-season contracts such as 10-day contracts)
that demonstrated a mean salary of $6.9 million and a median salary of $4.0 million. See NBA Contracts,
spotrac.com, http://www.spotrac.com/nba/contracts/ (last visited Mar. 13, 2017), archived at https://perma.cc/V7Y8-
LA5M. In reviewing this Report, the NBA stated that the mean salary was approximately $8 million and the median
salary was approximately $5 million. The NBA’s determination of the mean salary is determined by dividing all player
salaries by 396 players. 2017 NBA CBA, Art. 1, § 1(d). However, at any given time during the season, the number of
players on NBA rosters is approximately 450. Thus, we believe the best statistics are likely somewhere between
spotrac.com’s and the NBA’s. Basketball Reference, a well-regarded website, also provides data on this issue.
Basketball Reference lists the mean NBA salary as $4.9 million and the median salary as $2.1 million. See 2016-
2017 NBA Player Contracts, Basketball Reference, http://www.basketball-reference.com/contracts/players.html (last
visited Mar. 13, 2017), archived at https://perma.cc/94UD-3RCG. However, Basketball Reference’s salary database
includes 607 contracts, far more than the approximately 450 NBA players on rosters at any given time, and also
includes dozens of partial-season contracts for less than $100,000. Thus, we do not consider Basketball Reference’s
data sufficiently accurate to be used here.
1379
NBA Contracts, spotrac.com, http://www.spotrac.com/nba/contracts/ (last visited Mar. 13, 2017), archived at
https://perma.cc/V7Y8-LA5M.
1380
2017 NBA CBA, Art. XXIX, § 1.
1381
2011 NFL CBA, Art. 25, § 1.
1382
Major League Rules, Rule 2(c)(2)(A).
1383
2013 NHL CBA, § 16.4(a).
1384
See 2017 NBA CBA, Art. IX § 1.
1385
Id.
1386
See NBA Contracts, spotrac.com, http://www.spotrac.com/nba/contracts/ (last visited Mar. 13, 2017), archived at
https://perma.cc/V7Y8-LA5M.
1387
The ten largest contracts in the 2016–17 season were: Mike Conley and the Memphis Grizzlies ($152.6m)
Damian Lillard and the Portland Trailblazers ($139.9m); DeMar DeRozan and the Toronto Raptors ($139.0m);
Bradley Beal and the Washington Wizards ($127.2m); Andre Drummond and the Detroit Piston ($127.2m); Anthony
Davis and the New Orleans Pelicans ($127.2m); Carmelo Anthony and the New York Knicks ($124.0m); Nicolas
Batum and the Charlotte Hornets ($120.0m); Chris Bosh and the Miami Heat ($118.7m); and, James Harden and the
Houston Rockets ($118.0m). NBA Contracts, spotrac.com, http://www.spotrac.com/nba/contracts (last visited Jan. 30,
2017), archived at https://perma.cc/KR3K-M576.
1388
2017 NBA CBA, Ex. A.
1389
See 2017 NBA CBA, Art. II § 4. Negotiating over guarantees for mental disability is potentially troubling. A player
and his agent may be unlikely to want to raise that issue as a point of negotiation for fear of causing the club to be
concerned that the player suffers from a mental disability. Nevertheless, according to the NBA, many contracts in the
NBA include guarantees for mental disability.

!
276!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1390
A sign-and-trade contract is one in which a player signs with his prior club only to allow his prior club to then trade
him to a new club. These transactions allow both clubs to take advantage of certain Salary Cap provisions, which
ultimately benefits the player as well by enabling the desired transaction and contract.
1391
2017 NBA CBA, Art. VII § 8(e)(1).
1392
2017 NBA CBA, Art. VIII § 1(c)(ii).
1393
2017 NBA CBA, Art. XI § 1(c)(i)(4).
1394
Larry Coons, Larry Coon’s NBA Salary Cap FAQ #64, CBA FAQ, http://www.cbafaq.com/salarycap.htm (last
visited Aug. 27, 2015), archived at http://perma.cc/K9XV-FRTE; Tom Penn, NBA Player Have Best Deal, ESPN (Nov.
3, 2011 1:17 PM), http://espn.go.com/espn/commentary/story/_/id/7181583/even-concessions-nba-players-best-deal-
pro-athletes, archived at http://perma.cc/Z3SR-5JPK (“About 90 percent of all NBA contracts are fully guaranteed for
payment on the day that they are signed by the player.”)
1395
See NBA Contracts, Spotrac.com, http://www.spotrac.com/nba/contracts (last visited Jan. 30, 2017), archived at
https://perma.cc/KR3K-M576.
1396
2013 NHL CBA, § 3.1.
1397
2013 NHL CBA, § 50.4(b).
1398
2013 NHL CBA, § 50.1(a).
1399
See The Business of Hockey, Forbes (Nov. 30, 2016), http://www.forbes.com/nhl-valuations/list/, archived at
https://perma.cc/545K-NQBV (listing NHL clubs’ estimated revenues).
1400
2013 NHL CBA, § 50.5(b).
1401
James O’Brien, The NHL’s Salary Cap for 2016-17 is $73M, Pro Hockey Talk (June 21, 2016, 8:54 PM),
http://nhl.nbcsports.com/2016/06/21/the-nhls-salary-cap-for-2016-17-is-73m/, archived at https://perma.cc/R4FW-
WEWR.
1402
2013 NHL CBA, § 9.1(b).
1403
2013 NHL CBA, § 9.1(b).
1404
Players 25 and older are not subject to the Entry Level System and have no limits on their compensation. 2013
NHL CBA, § 9.1(b).
1405
A player’s Paragraph 1 Salary is the player’s salary as specified in Paragraph 1 of the SPC. See Ex. 1 to the
2013 NHL CBA (“The Club hereby employs the Player as a skilled hockey Player for the term of __________ League
Year(s) commencing the later of July 1, 20 or upon execution of this SPC and agrees, subject to the terms and
conditions hereof, to pay the Player a salary of ___________ US Dollars ($__________).”).
1406
See 2013 NHL CBA, §9.3, §9.5.
1407
2013 NHL CBA, § 9.3.
1408
The different performance bonuses available to players are described in Exhibit 5 of the 2013 NHL CBA.
1409
Id.
1410
2013 NHL CBA, § 10.2(a)(i).
1411
Id.
1412
2013 NHL CBA, § 10.1(a).
1413
Id.
1414
2013 NHL CBA, § 10.2(b)(i).
1415
2013 NHL CBA, § 10.1(b).
1416
Id.
1417
2013 NHL CBA at p. 502, letter from William L. Day, Deputy Commissioner, NHL, to Don Zavelo, General
Counsel, NHLPA (Feb. 15, 2013).
1418
Id.
1419
2013 NHL CBA, § 10.1(c).
1420
Id.
1421
See 2013 NHL CBA, § 10.2(c).
1422
Id.
1423
2013 NHL CBA, § 12.1(a).
1424
2013 NHL CBA, § 12.2.
1425
2013 NHL CBA, § 12.3(a).
1426
2013 NHL CBA, § 12.3(b).
1427
2013 NHL CBA, § 12.9(b)-(c).
1428
2013 NHL CBA, § 12.9(n).
1429
2013 NHL CBA, § 11.12.
1430
2013 NHL CBA, § 50.6.
1431
2013 NHL CBA, § 50.7.
1432
2013 NHL CBA, § 50.5(d)(ii).
1433
NHL rejects Kovalchuk deal, ESPN (Jul. 21, 2010), http://sports.espn.go.com/new-
york/nhl/news/story?id=5397588, archived at https://perma.cc/88W2-CZY8.
1434
Id.

!
277!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1435
Greg Wyshynski, NHL lets NJ Devils off hook for Ilya Kovalchuk contract punishment, Yahoo! Sports (Mar. 6,
2014, 1:18 PM), http://sports.yahoo.com/blogs/nhl-puck-daddy/nhl-lets-nj-devils-off-hook-for-ilya-kovalchuk-contract-
punishment-181853523.html, archived at http://perma.cc/BM37-BDTJ.
1436
See 2013 NHL CBA, § 50.8(b)(iv).
1437
2011 NFL CBA, Art. 7 3(e) (“No Rookie Contract may provide for an annual increase of more than 25% of the
player’s Year-One Rookie Salary unless such contract provides only for Paragraph 5 Salary equal to the then-
applicable Minimum Active/Inactive Salary for each League Year of the Contract.”)
1438
2011 NFL CBA, Art. 12, § 7.
1439
See NHL Contracts, Spotrac.com, http://www.spotrac.com/nhl/contracts/ (last visited Jan. 30, 2017), archived at
https://perma.cc/3FR9-GNRQ.
1440
Id.
1441
NHL Standard Player Contract, ¶ 13.
1442
NHL Standard Player Contract, ¶ 13(d).
1443
Id.
1444
See James Mirtle, David Clarkson and His Buyout-Proof Contract, Globe & Mail, Apr. 2, 2014,
http://www.theglobeandmail.com/sports/hockey/leafs-beat/mirtle-david-clarkson-and-his-buyout-proof-
contract/article17783243/?cmpid=rss1&click=dlvr.it, archived at http://perma.cc/L4GE-WF5Y (describing David
Clarkson’s signing-bonus-laden contract as “buyout-proof”); Lightning to Buy Out Vincent Lecavalier, Canoe, June 27,
2013, http://slam.canoe.com/Slam/Hockey/NHL/TampaBay/2013/06/27/20933546.html?cid=rsssportsslam!, archived
at http://perma.cc/A7MA-3QE6 (reporting that the club would pay “the full amount of what’s left on [Lecavalier’s]
signing bonus” as part of his buy-out).
1445
2013 NHL Standard Player Contract, ¶5(d).
1446
See 2014 CFL CBA, § 30.01. The CFL’s Salary Cap is formally known as the “Salary Expenditure CAP.” Id.
1447
2014 CFL CBA, § 14.09.
1448
2016 Adjusted Team Salary Caps, Nat’l Football League Players Ass’n, Mar. 7, 2016,
https://www.nflpa.com/news/all-news/2016-adjusted-team-salary-caps, archived at https://perma.cc/K9GZ-ZDGN.
1449
2006 CFL CBA, § 30.02 (“The parties agree that if during any one calendar year during the term of this
Agreement the current economic conditions prevailing in the C.F.L. shall improve to the extent that the defined
player’s compensation is less than 56% of the defined gross revenue on a league wide basis, the C.F.L. and the
Member Clubs in the C.F.L. shall pay to the C.F.L.P.A. the difference.”)
1450
Andrew Bucholtz, What percentage of league-wide revenues did CFL players get in 2013 under the old CBA?,
Yahoo! Sports Can. (June 9, 2014, 6:49 PM), https://ca.sports.yahoo.com/blogs/cfl-55-yard-line/percentage-league-
wide-revenues-did-cfl-players-2013-224954281.html, archived at http://perma.cc/F5NU-FWE3.
1451
Id.
1452
CFL Standard Player Contract, ¶ 15; New five-year CBA ratified by CFL and CFLPA, Can. Football League (June
13, 2014, 3:00 PM), http://www.cfl.ca/article/new-five-year-cba-ratified-by-cfl-and-cflpa, archived at
http://perma.cc/EBL2-NRDA.
1453
CFL Standard Player Contract, ¶ 15.
1454
Id.
1455
See 2014 CFL CBA, § 14.03 (discussing rights of free agents).
1456
2014 CFL CBA, § 9.
1457
Emily Kaplan, The CFL’s Most Outstanding Player Moonlights as a Banker, Monday Morning Quarterback with
Peter King, Jun. 26, 2014, http://mmqb.si.com/2014/06/26/cfl-off-season-jobs-jon-cornish-calgary-stampeders/,
archived at http://perma.cc/K6C7-2CM9.
1458
Signing bonuses for non-veterans are rare, but signing bonuses of up to $75,000 for veterans have occurred. See
Frequently Asked Questions About Compensation, Can. Football League Database,
https://cfldb.ca/faq/compensation/ (last visited Aug. 28, 2015), archived at https://perma.cc/5VGW-3V9B; see also
Victoria Revay, Show me the money: CFL players’ salaries, Global News, Nov. 20, 2012,
http://globalnews.ca/news/310679/show-me-the-money-cfl-players-salaries/, archived at http://perma.cc/Q373-RETY.
1459
Emily Kaplan, The CFL’s Most Outstanding Player Moonlights as a Banker, Monday Morning Quarterback with
Peter King, Jun. 26, 2014, http://mmqb.si.com/2014/06/26/cfl-off-season-jobs-jon-cornish-calgary-stampeders/,
archived at http://perma.cc/K6C7-2CM9.
1460
Id.
1461
Roughriders sign quarterback Durant to contract extension, Globe & Mail, Apr. 16, 2014,
http://www.theglobeandmail.com/sports/football/roughriders-sign-quarterback-durant-to-contract-
extension/article18042091/, archived at http://perma.cc/26WW-WDJU.
1462
Aside from guarantees for veteran players, “CFL contracts are not guaranteed in the case of a player being
released or beyond the current season in the case of a football-related injury.” See Can. Football League Database
supra note 1458.
1463
CFL Standard Player Contract, ¶ 6.
1464
CFL Standard Player Contract, ¶10(a).

!
278!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1465
CFL Standard Player Contract, ¶10(b).
1466
CFL Standard Player Contract, ¶10(c).
1467
CFL Standard Player Contract, ¶10(d).
1468
2014 CFL CBA, Art. 15.
1469
Where a player is injured in one season, fails the pre-season physical the next season because of that injury, and
is terminated by the club as a result, the player is entitled to 50% of his salary for that season up to a maximum of
$1.1 million in the 2015 season. If the player is still physically unable to play two seasons after the injury, he is
entitled to 30% of his salary up to a maximum for $525,000 in 2015. A player is only entitled to Injury Protection once
in his career. See 2011 NFL CBA, Art. 45.
1470
A player with at least four years of experience who has his contract terminated after the first game of the season
is entitled to the remainder of his salary for that season once in his career. 2011 NFL CBA, Art. 30.
1471
Justin Dunk, Top CFL picks land rookie-record signing bonuses, SportsNet (May 15, 2015, 11:19 AM),
http://www.sportsnet.ca/football/cfl/top-cfl-picks-land-rookie-record-signing-bonuses/, archived at
http://perma.cc/8NUF-A5J6.
1472
See Fraser v. Major League Soccer, L.L.C., 97 F.Supp. 2d 130, 132-34 (D. Mass. 2000) (discussing MLS’
structure, operations and origin, including meetings with NFL’s antitrust counsel).
1473
See Fraser v. Major League Soccer, L.L.C., 284 F.3d 47, 53–55 (1st Cir. 2002) (discussing MLS’ structure and
operations).
1474
Id.
1475
Id.
1476
Id.; Kevin O’Riordan, Dempsey Transfer Highlights Influence of MLS Single-Entity Economic Structure, Bus. Of
Soccer, Aug. 26, 2013, http://www.businessofsoccer.com/2013/08/26/dempsey-transfer-highlights-mls-single-entity-
economic-structure/, archived at http://perma.cc/2TKQ-BQ4R.
1477
See Order, Namoff v. D.C. Soccer LLC, No. 2012-CA-7050, at *2 (D.C.Sup.Ct. May 8, 2014) (“MLS has sole
discretion to hire players and provides their salary and benefits[.]”)
1478
See Fraser v. Major League Soccer, L.L.C., 97 F.Supp. 2d 130, 132–34 (D. Mass. 2000) (discussing MLS’
structure, operations and origin, including meetings with NFL’s antitrust counsel); Michael McCann, In pursuit of free
agency, players could challenge MLS as single entity, Sports Illustrated, Jan. 27, 2015, http://www.si.com/planet-
futbol/2015/01/26/mls-cba-players-union-free-agency-single-entity-lawsuit, archived at http://perma.cc/JUV9-BGGP;
Matthew J. Jakobsze, Kicking “Single-Entity” to the Sidelines: Reevaluating the Competitive Reality of Major League
Soccer After American Needle and the 2010 Collective Bargaining Agreement, 31 N. Ill. U. L. Rev. 131, 132-33
(2010).
1479
See American Needle, Inc. v. Nat’l Football League, 560 U.S. 183, 186 (2010), citing 15 U.S.C. § 1.
1480
See Copperweld Corp. v. Independence Tube Corp., 467 U.S. 752 (1984) (parent corporation and wholly owned
subsidiary were not legally capable of conspiring with each other under Section 1 of the Sherman Act).
1481
See Fraser v. Major League Soccer, L.L.C., 97 F.Supp.2d 130, 135–36 (D.Mass. 2000).
1482
See Fraser v. Major League Soccer, L.L.C., 284 F.3d 47, 55 (1st Cir. 2002).
1483
The plaintiffs had also alleged that MLS had violated Section 2 of the Sherman Antitrust Act by monopolizing the
market for the services of Division I professional soccer players in the United States, and Section 7 of the Clayton Act
by combining in such a way as to substantially lessen competition. See Fraser v. Major League Soccer, L.L.C., 284
F.3d 47, 55 (1st Cir. 2002).
1484
Id. at 56–59.
1485
See id.
1486
See About the MLS Players Union, Major League Soccer Players Union,
https://www.mlsplayers.org/about_mlspu.html (last visited Aug. 28, 2015), archived at http://perma.cc/P2XJ-MN4R.
1487
See Michael McCann, In pursuit of free agency, players could challenge MLS as single entity, Sports Illustrated,
Jan. 27, 2015, http://www.si.com/planet-futbol/2015/01/26/mls-cba-players-union-free-agency-single-entity-lawsuit,
archived at http://perma.cc/JUV9-BGGP (discussing risks of MLSPU decertifying as players’ labor representative and
filing antitrust lawsuit); Matthew J. Jakobsze, Kicking “Single-Entity” to the Sidelines: Reevaluating the Competitive
Reality of Major League Soccer After American Needle and the 2010 Collective Bargaining Agreement, 31 N. Ill. U. L.
Rev. 131, 155 (2010) (same).
1488
See, e.g., id.; Diana C. Taylor, Aimed at the Goal?: The Sustainability of Major League Soccer’s Structure, 9
Willamette Sports L.J. 1 (2011); Order, Namoff v. D.C. Soccer LLC, No. 2012-CA-7050 (D.C.Sup.Ct. May 8, 2014)
(finding MLS and D.C. United to be “concurrent employers” of players).
1489
15 U.S.C. § 15 (“any person who shall be injured in his business or property by reason of anything forbidden in
the antitrust laws may sue therefor in any district court of the United States in the district in which the defendant
resides or is found or has an agent, without respect to the amount in controversy, and shall recover threefold the
damages by him sustained, and the cost of suit, including a reasonable attorney’s fee”).
1490
MLS Roster Rules and Regulations, Major League Soccer, http://www.mlssoccer.com/league/official-rules/mls-
roster-rules-and-regulations (last visited Mar. 8, 2017), archived at https://perma.cc/SC9V-2TW3.

!
279!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1491
Paul Tenorio, Foose: New MLS CBA a ‘watershed moment’, Orlando Sentinel, Mar. 7, 2015, available at 2015
WLNR 7038891.
1492
MLS Roster Rules and Regulations, Major League Soccer, http://www.mlssoccer.com/league/official-rules/mls-
roster-rules-and-regulations (last visited Mar. 8, 2017), archived at https://perma.cc/SC9V-2TW3.
1493
This information was provided by the MLSPU.
1494
See Steven Goff, D.C. United news and notes, Wash. Post, Apr. 14, 2015, available at 2015 WLNR 10882564
(discussing D.C. United player Bill Hamid’s weighing playing in Europe against earning a designated player salary);
Daniel Boniface, Kevin Doyle, Colorado Rapids agree to contract; June arrival expected, Mar. 21, 2015, Denver Post,
available at 2015 WLNR 8515066 (discussing Colorado Rapids’ acquisition of English soccer player Kevin Doyle as a
designated player); Steven Goff, New CBA called ‘win’ for MLS players, Wash. Post, Mar. 9, 2015, available at 2015
WLNR 7003801 (discussing designated player salaries and exception to Salary Cap); Gary Kingston, As MLS
evolves, so does the Beckham Rule; League’s designated player clause is helping keep talented players in North
America, Vancouver Sun, Aug. 9, 2014, available at 2014 WLNR 21837206.
1495
For the list of Designated Players, see Designated Players, As of August 10, 2016, Major League Soccer,
http://pressbox.mlssoccer.com/content/designated-players (last visited Sept. 14, 2016), archived at
https://perma.cc/S5L7-ECRW..
1496
These figures were calculated using data provided by the MLSPU at https://www.mlsplayers.org/salary_info.html,
archived at https://perma.cc/54D9-22JG. The list of Designated Players is available at Designated Players, MLS
(Aug. 3, 2016), http://pressbox.mlssoccer.com/content/designated-players, archived at https://perma.cc/8HT2-E9DT.
1497
The American-born players were Jozy Altidore, DaMarcus Beasley, Alejandro Bedoya, Matt Besler, Michael
Bradley, Clint Dempsey, Maurice Edu, Tim Howard, and Graham Zusi.
1498
See Chris Smith, Major League Soccer’s Most Valuable Teams 2016, Forbes (Sep. 7, 2016, 10:32 AM),
http://www.forbes.com/sites/chrissmith/2016/09/07/major-league-soccers-most-valuable-teams-2016-new-york-
orlando-thrive-in-first-seasons/, archived at https://perma.cc/K7B6-DJ86.
1499
Richard Sandomir, M.L.S. and Union Reach Deal Giving Free Agency to Veterans, N.Y. Times, Mar. 4, 2015,
http://www.nytimes.com/2015/03/05/sports/soccer/mls-and-union-reach-deal-giving-free-agency-to-
veterans.html?_r=0, archived at http://perma.cc/7KUK-FVWE.
1500
Roster Rules and Regulations, Major League Soccer, http://pressbox.mlssoccer.com/content/roster-rules-and-
regulations (last visited Aug. 28, 2015), archived at http://perma.cc/D885-JCL9, at § II(G)(2); 2015 MLS CBA, §
29.6(a)(i).
1501
Jeff Carlisle, The details on Major League Soccer’s new collective bargaining agreement, ESPN (Mar 4, 2015)
http://www.espnfc.us/major-league-soccer/19/blog/post/2332341/the-details-on-major-league-soccers-new-collective-
bargaining-agreement, archived at http://perma.cc/QF79-8XLB; 2015 MLS CBA, § 29.6(b)(iii).
1502
2015 MLS CBA, § 10.1.
1503
This information was provided by MLSPU.
1504
Roster Rules and Regulations, Major League Soccer, http://pressbox.mlssoccer.com/content/roster-rules-and-
regulations (last visited June 23, 2016), archived at https://perma.cc/2S5S-WHNQ.
1505
See id.
1506
These figures were calculated using data provided by the MLSPU. See 2016 MLS Player Salaries: May 15, 2016:
Alphabetical, Major League Soccer Players Union,
https://www.mlsplayers.org/images/May%2015,%202016%20Salary%20Information%20-%20Alphabetical.pdf (last
visited Sept. 14, 2016), archived at https://perma.cc/PX9E-KMTX..
1507
See id.
1508
See id.
1509
See 2016 MLS Player Salaries: May, 2016: Alphabetical supra n. 1506.
1510
See Steven Goff, MLS union and management preparing for collective bargaining negotiations, Wash. Post, Nov.
21, 2014, available at 2014 WLNR 32859557.
1511
2015 MLS CBA, § 18.6(b).
1512
2015 MLS CBA, § 2(x).
1513
MLS Announces CBA Changes, U.S. Nat’l Soccer Players, Mar. 23, 2010,
http://www.ussoccerplayers.com/2010/03/mls-announces-cba-changes.html, archived at http://perma.cc/HW5N-
TSAV.
1514
See 2016 MLS Player Salaries: May, 2016: Alphabetical supra n. 1506.
1515
Id.
1516
See What is average NFL player’s career length? Longer than you might think, Commissioner Goodell says, Nat’l
Football League, Apr. 18, 2011, http://nflcommunications.com/2011/04/18/what-is-average-nfl-player%E2%80%99s-
career-length-longer-than-you-might-think-commissioner-goodell-says/, archived at http://perma.cc/8UHQ-JMVX
(discussing dispute between NFLPA’s assertion that the average career is 3.5 years and the NFL’s assertion that the
average career is 6 years); Average NFL Career Length, Sharp Football Analysis, Apr. 30, 2014,
http://www.sharpfootballanalysis.com/blog/?p=2133, archived at http://perma.cc/4EZY-E7ML (discussing
disagreement between NFLPA and NFL and determining that the average drafted player plays about 5 years).

!
280!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1517
William D. Witnauer, Richard G. Rogers & Jarron M. Saint Onge, Major league baseball career length in the 20th
century, 26 Population Res. & Pol’y Rev. 4, 371-386 (2007).
1518
Susan Konig, Financial Planning for the Pros, 34 Registered Representative (Apr. 2010), available at 2010
WLNR 26366417.
1519
Average Length of an NHL Player Career, QuantHockey.com,
http://www.quanthockey.com/Distributions/CareerLengthGP.php (last visited Aug. 28, 2015), archived at
http://perma.cc/95QB-X9P9.
1520
Matthew Black, Players rely on education, experience after CFL career, Thunderbird, Mar. 31, 2011,
http://thethunderbird.ca/2011/03/31/players-bet-on-education-after-cfl-career/, archived at http://perma.cc/M92S-
KNQ8.
1521
Nick Schwartz, The average career earnings of athletes across America’s major sports will shock you, For the
Win Blog - USA Today (Oct. 24, 2013, 10:07 AM), http://ftw.usatoday.com/2013/10/average-career-earnings-nfl-nba-
mlb-nhl-mls, archived at http://perma.cc/J8QL-Q3RG. Nevertheless, as pointed by the MLPSU in its review of this
Report, the author of this article did not indicate how he arrived at the 3.2 years statistic. Moreover, MLSPU Executive
Director Bob Foose stated that “this number is significantly misleading given the global nature of soccer (there are, I
believe, professional leagues in over 80 countries around the world, typically with multiple such leagues in each
country). We have not consistently tracked the total average career length of MLS players, but when we last did an
exhaustive study, in 2013, the average MLS player (whose career was over) had played a total of just under 8.8
years of professional soccer over the course of that career. We haven’t updated these numbers since then, but I don’t
have any reason to believe that these numbers have changed significantly.” We believe this is a valid point and thus
suggest caution in considering the mean career length of MLS players. Athletes in the other leagues rarely play in
multiple professional leagues and thus the same concern is not present.
1522
The CFL and MLS cannot realistically be compared to the Big Four due to their relatively small amounts of
revenue and also the MLS’ attempted single-entity structure.
1523
See, e.g., Matt Bowen, Concussion in the NFL: The cost can be hard to calculate, Chi. Trib., Sep. 16, 2010,
available at 2010 WLNR 18355633 (“Without the guaranteed contracts we see in Major League Baseball or the NBA,
NFL players will continue to sacrifice their health and their future by playing through concussions.”); A. Jason
Huebinger, Beyond the Injured Reserve: The Struggle Facing Former NFL Players in Obtaining Much Needed
Disability Assistance, 16 Sport Law. J. 279, 283 (2009) (“The NFL is also fairly unique in its implementation of a hard
salary cap, which also works to artificially reduce player salaries. Under a hard cap system, no team may exceed a
given salary amount. Conversely, MLB and the NBA have much more relaxed caps, allowing for greater flexibility in
negotiations between the team and a player. Arguably the greatest disadvantage facing current NFL players… is the
lack of guaranteed contracts.”).
1524
Information about salaries and contracts was derived from data available on spotrac.com, the most reliable public
source for information about professional sports contracts based on our analysis. Indeed, as of February 2017, there
are 41 MLB contracts worth over $100 million while there are only 18 such contracts in the NBA, 12 in the NFL, and
three in the NHL.
1525
See, e.g., Mike Florio, Adrian Peterson takes aim at the NFLPA, ProFootballTalk (May 28, 2015, 9:18 PM),
http://profootballtalk.nbcsports.com/2015/05/28/adrian-peterson-takes-aim-at-the-nflpa/, archived at
http://perma.cc/GFQ6-QSCG (discussing Minnesota Vikings running back Adrian Peterson’s complaints about
guaranteed money in the NFL).
1526
See, e.g., Paul Needell, Upshaw’s legacy transcended the field, Star-Ledger (Newark, NJ), Aug. 22, 2008,
available at 2008 WLNR 15896505; Tim Tucker, No guarantees in the NFL inside ball, Atlanta J. & Const., Mar. 3,
2002, available at 2002 WLNR 4687719.
1527
See A. Jason Huebinger, Beyond the Injured Reserve: The Struggle Facing Former NFL Players in Obtaining
Much Needed Disability Assistance, 16 Sport Law. J. 279, 283 (2009); Matthew Levine, Despite His Antics, T.O. Has
a Valid Point: Why NFL Players Deserve a Bigger Piece of the Pie, 13 Vill. Sports & Ent. L.J. 425 (2006).
1528
Gene Upshaw, NFLPA’s Upshaw Responds, Wash. Post, Dec. 22, 2002, available at 2002 WLNR 15865309.
1529
NFLPA, A New Look at Guaranteed Contracts in the NFL (circa 2002) (on file with authors) (“Over half of all
salary earned by NFL players now is guaranteed”); Nat’l Football League Players Ass’n, Guaranteed Contracts in
Professional Team Sports: How Does the NFL Compare? (circa 2007) (on file with authors) (“at least 52% of all
compensation in the NFL is, in fact, ‘guaranteed’ to players.’”)
1530
Mike Florio, Fully-guaranteed contracts could cause problems for teams, players, ProFootballTalk (May 29, 2015,
9:55 AM), http://profootballtalk.nbcsports.com/2015/05/29/fully-guaranteed-contracts-could-cause-problems-for-
teams-players/, archived at http://perma.cc/GE9E-YSME (discussing potential problems with guaranteed contracts in
the NFL).
1531
For example, one rule that would likely have to be removed is the NFL’s requirement that clubs deposit into a
separate account the present value, less $2 million, of guaranteed compensation to be paid in future years. 2011
CBA, Art. 26 § 9. Former NFL club executive Andrew Brandt believes clubs “hide behind” the funding rule to avoid
guaranteeing player compensation, and have been largely successful in doing so. Andrew Brandt, Supplemental
Peer Review Response (Nov. 6, 2015).

!
281!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1532
See Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of
NFL Players: Legal and Ethical Analysis and Recommendations, Recommendation 2:1-A (2016).
1533
MLS’ unique structure is discussed at length in Chapter 5: Compensation, Section F: Compensation in MLS.
1534
See American Needle, Inc. v. Nat’l Football League, 560 U.S. 183, 196-97 (2010) (“The teams compete with one
another, not only on the playing field, but to attract fans, for gate receipts, and for contracts with managerial and
playing personnel.”)
1535
See Clarett v. Nat’l Football League, 369 F.3d 124, 137 (2d Cir. 2004) (discussing application of antitrust law to
NFL’s eligibility rule).
1536
See Am. Needle, Inc. v. Nat’l Football League, 560 U.S. 183, 186 (2010), citing 15 U.S.C. § 1.
1537
See id. at 203, n.10, quoting Board of Trade of Chicago v. United States, 246 U.S. 231, 238 (1918) (“The true test
of legality is whether the restraint imposed is such as merely regulates and perhaps thereby promotes competition or
whether it is such as may suppress or even destroy competition. To determine that question the court must ordinarily
consider the facts peculiar to the business to which the restraint is applied; its condition before and after the restraint
is imposed; the nature of the restraint and its effect, actual or probable. The history of the restraint, the evil believed
to exist, the reason for adopting the particular remedy, the purpose or end sought to be attained, are all relevant
facts. This is not because a good intention will save an otherwise objectionable regulation or the reverse; but because
knowledge of intent may help the court to interpret facts and to predict consequences.”)
1538
See Brown v. Pro Football, Inc., 518 U.S. 231 (1996).
1539
See Clarett v. Nat’l Football League, 369 F.3d 124 (2d Cir. 2004) (NFL’s eligibility rule immune from antitrust
scrutiny as a result of non-statutory labor exemption).
1540
Some scholars have debated whether other Circuit Courts would find that eligibility rules are protected by the
non-statutory labor exemption. See Marc Edelman and Joseph A. Wacker, Collectively Bargained Age/Education
Requirements: A Source of Antitrust Risk for Sports Club-Owners or Labor Risk for Players Unions? 115 Penn St. L.
Rev. 341 (2010); Michael A. McCann, Justice Sonia Sotomayor and the Relationship Between Leagues and Players:
Insights and Implications, 42 Conn. L. Rev. 901 (2010). Also of note, in two cases involving now defunct professional
sports league eligibility rules that were not negotiated with a union, the courts found that the rules did violate antitrust
laws. See Linseman v. World Hockey Ass’n, 439 F. Supp. 1315 (D. Conn. 1977); Boris v. U.S. Football League, 83-
cv-4980, 1984 WL 894 (C.D. Cal. Feb. 28, 1984).
1541
Unions are empowered to negotiate terms and conditions that might affect future employees, even if those
employees are not yet a part of the union’s bargaining unit. See Clarett v. Nat’l Football League, 369 F.3d 124, 139
(2d Cir. 2004) (discussing union’s rights to “preserve jobs for current players to the detriment of new employees and
the exclusion of outsiders”); Wood v. Nat’l Basketball Assoc., 809 F.2d 954 (2d Cir. 1987) (denying prospective NBA
player’s antitrust challenge to CBA provisions negotiated between NBA and NBPA).
1542
2011 NFL CBA, Art. 6, § 2(a).
1543
Draft FAQ, Major League Baseball, http://mlb.mlb.com/mlb/draftday/faq.jsp (last visited May 13, 2015), archived
at http://perma.cc/4HA7-4D8L.
1544
2017 NBA CBA, Art. X, § 3.
1545
2013 NHL CBA, Art. 8, § 8.2.
1546
CFL Draft Expanded to seven rounds, Can. Football League, May 1, 2013, http://cfl.ca/article/cfl-draft-expanded-
to-seven-rounds, available at http://perma.cc/SB4N-ZJYQ.
1547
Roster Rules and Regulations, Major League Soccer, http://pressbox.mlssoccer.com/content/roster-rules-and-
regulations (last visited Sept. 22, 2015), archived at http://perma.cc/9BLN-R7QD.
1548
See Who We Are, Nat’l Collegiate Athletics Ass’n, http://www.ncaa.org/about/who-we-are (last visited Sept. 23,
2015), archived at http://perma.cc/RXA5-4FLL; Membership, Nat’l Collegiate Athletics Ass’n,
http://www.ncaa.org/about/who-we-are/membership (last visited Sept. 23, 2015), archived at http://perma.cc/6BTQ-
G7QS (describing membership as more than 1,200 schools).
1549
NCAA Division I Manual, Bylaw 12.01.1.
1550
NCAA Division I Manual, Bylaw 12.01.2.
1551
See NCAA Division I Manual, Bylaw 12.02.9 (“Pay is the receipt of funds, awards or benefits not permitted by the
governing legislation of the Association for participation in athletics.”); id. at Bylaw 12.02.10 (“A professional athlete is
one who receives any kind of payment, directly or indirectly, for athletics participation except as permitted by the
governing legislation of the [National Collegiate Athletic] Association.”); id. at Bylaw 12.1.2.1 (discussing “Prohibited
Forms of Pay”); id. at 12.2 (regulating “Involvement With Professional Teams”); id. at 12.4 (regulating employment of
student-athletes and requiring that student-athlete compensation be “[a]t a rate commensurate with the going rate in
that locality for similar services”); id. at 12.5 (regulating “Promotional Activities); id. at Bylaw 12.01.4 (“A grant-in-aid
[a scholarship] administered by an educational institution is not considered to be pay or the promise of pay for
athletics skill, provided it does not exceed the financial aid limitations set by the [National Collegiate Athletic]
Association’s membership.”)
1552
See O’Bannon v. Nat’l Collegiate Athletic Ass’n, 802 F.3d 1049, 1054-55 (9th Cir. 2015) (“In August 2014, the
NCAA announced it would allow athletic conferences to authorize their member schools to increase scholarships up

!
282!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
to the full cost of attendance. The 80 member schools of the five largest athletic conferences in the country voted in
January 2015 to take that step, and the scholarship cap at those schools is now at the full cost of attendance.”)
1553
NCAA Division I Manual, Bylaw 12.1.2 (“An individual loses amateur status and thus shall not be eligible for
intercollegiate competition in a particular sport if the individual… [e]nters into an agreement with an agent.”).
1554
NCAA Division I Manual, Bylaw 12.3.2.
1555
NCAA Division I Manual, Bylaw 12.3.2.1 (“A lawyer may not be present during discussions of a contract offer with
a professional organization or have any direct contact (in person, by telephone or by mail) with a professional sports
organization on behalf of the individual. A lawyer’s presence during such discussions is considered representation by
an agent.”) In Oliver v. Natl. Collegiate Athletic Assn., 920 N.E.2d 203 (Ohio Com.Pl. 2009), a college baseball
player obtained a permanent injunction against the enforcement of this Bylaw. However, to avoid that result, the
NCAA appealed the decision, and settled with the player for $750,000 in exchange for the vacatur of the court’s
decision. Thus, the rule stands. See Glenn M. Wong, Warren Zola, Chris Deubert, Going Pro in Sports: Providing
Guidance to Student-Athletes in a Complicated Legal & Regulatory Environment, 28 Cardozo Arts & Ent. L.J. 553,
583-85 (2011) (discussing the Oliver case).
1556
Brian Bennett, NCAA board votes to allow autonomy, ESPN (Aug. 8, 2014), http://espn.go.com/college-
sports/story/_/id/11321551/ncaa-board-votes-allow-autonomy-five-power-conferences, archived at
https://perma.cc/Y6B9-5FP8.
1557
Teddy Cahill, High School Draftees Permitted to Have Agent, Baseball America, Jan. 15, 2016,
http://www.baseballamerica.com/draft/high-school-draftees-permitted-agent/#gFU7SYIRjVxSdxzY.97, archived at
https://perma.cc/YS4K-4ZHX.
1558
Id.
1559
The NCAA’s Bylaws suggest that these players can return but in reality they cannot. A basketball student-athlete
can return to college if he declares his intention to do so “before the first day of the spring National Letter of Intent
signing period for the applicable year.” NCAA Division I Manual, Bylaw 12.2.4.2.1.1. The first day of the National
Letter of Intent signing period for basketball is in April. NLI Signing Dates for Prospective Student-Athletes Signing
2015–16 and Enrolling 2016–17, Nat’l Letter of Intent, http://www.nationalletter.org/signingDates/
http://www.nationalletter.org/signingDates/ (last visited Sept. 23, 2015), archived at http://perma.cc/65MQ-DBAN. The
NBA Draft is in June. Thus, the player cannot go through the Draft in June and still meet the April deadline to declare
his intention to return in college. Similarly, a football student-athlete can return to college if he declares his intention to
do so “within 72 hours following the National Football League draft declaration date.” NCAA Division I Manual, Bylaw
12.2.4.2.3. The NFL requires student-athletes to declare for the NFL Draft by January 15. See Unofficial
underclassmen early entry list for 2015 NFL Draft, NAT’L FOOT LEAGUE, Jan. 2, 2015,
http://www.nfl.com/news/story/0ap3000000441827/article/unofficial-underclassmen-early-entry-list-for-2015-nfl-draft,
archived at http://perma.cc/SD8M-PUXV. The NFL Draft is in April or May. Thus, the player cannot go through the
Draft in April or May and still meet the January deadline to declare his intention to return to college.
1560
See, e.g., O’Bannon v. Nat’l Collegiate Athletic Ass’n, 802 F.3d 1049, 1054-55 (9th Cir. 2015); In re Nat’l
Collegiate Athletic Ass’n Grant-in-Aid Cap Antitrust Litigation, 14-md-2541, 2016 WL 4154855 (N.D. Cal. Aug. 5,
2016).
1561
See Student-Athlete Insurance Programs, Nat’l Collegiate Athletics Ass’n,
http://www.ncaa.org/about/resources/insurance/student-athlete-insurance-programs (last visited Sept. 23, 2015),
archived at http://perma.cc/MHL6-7T3A [hereinafter NCAA ESDI Program]. See also Glenn M. Wong & Chris
Deubert, The Legal and Business Aspects of Disability Insurance Policies in Professional and College Sports, 17 Vill.
Sports & Ent. L.J. 473, 506 (2010).
1562
See Wong & Deubert, supra n 1561.
1563
Id. at 507–08.
1564
Id.
1565
Id.
1566
Student-Athlete Insurance Programs, Nat’l Collegiate Athletics Ass’n,
http://www.ncaa.org/about/resources/insurance/student-athlete-insurance-programs (last visited Sept. 23, 2015),
archived at http://perma.cc/MHL6-7T3A.
1567
See Michael David Smith, Clemson buys $5m insurance policies for Deshaun Watson, ProFootballTalk (Aug. 17,
2016, 4:18 PM), http://nhl.nbcsports.com/2016/10/11/nhl-plans-on-fining-teams-who-violate-new-concussion-
protocol/, archived at https://perma.cc/M5PM-LS96; Barry Petchesky, FSU Paid For Jameis Winston’s Insurance
Policy On His Draft Stock, Deadspin (Aug. 5, 2014), http://deadspin.com/fsu-paid-for-jameis-winstons-insurance-
policy-on-his-dr-1616301588, archived at http://perma.cc/DVB5-YGN7.
1568
See Wong & Deubert, supra n 1561.
1569
See Wong & Deubert, supra n 1561 at 507; see also Petchesky, supra n. 1567.
1570
Wong & Deubert, supra n. 1561 at 495–96.
1571
Bryan Fischer, NCAA issues waiver allowing greater access to insurance, Nat’l Football League, Oct. 15, 2014,
http://www.nfl.com/news/story/0ap3000000411358/article/ncaa-issues-waiver-allowing-greater-access-to-insurance,
archived at http://perma.cc/E85A-ZZPM.

!
283!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1572
Zac Jackson, Report: Browns CB becoming first to collect loss of draft value insurance, ProFootballTalk (Oct. 2,
2015, 11:48 AM), http://profootballtalk.nbcsports.com/2015/10/02/report-browns-cb-becoming-first-to-collect-loss-of-
draft-value-insurance/, archived at https://perma.cc/KUG6-5CER (reporting that “many top college players are taking
out such policies”).
1573
Dennis Dodd, Ekpre-Olomu expected to be first to collect on loss of draft value insurance, CBS Sports (Oct. 2,
2015, 1:37 AM), http://www.cbssports.com/collegefootball/writer/dennis-dodd/25324664/ekpre-olomu-expected-to-be-
first-to-collect-on-loss-of-draft-value-insurance, archived at https://perma.cc/QT3Q-S4WE.
1574
Id.
1575
Id.
1576
Id.
1577
Michael David Smith, Jaylon Smith will receive insurance payment, Myles Jack won’t, ProFootballTalk (Apr. 29,
2016, 10:33 PM), http://profootballtalk.nbcsports.com/2016/04/29/jaylon-smith-will-receive-insurance-payment-myles-
jack-wont/, archived at https://perma.cc/7Q4P-3HAV.
1578
2011 NFL CBA, Art. 6 § 2(b).
1579
A notable exception was former University of Pittsburgh wide receiver Larry Fitzgerald. Fitzgerald had attended
five years of high school and was thus eligible for the 2004 Draft after only two years of college football. Paul Zeise,
Fitzgerald Leaving Pitt Early for NFL, PITTSBURGH POST-GAZETTE, Feb. 10, 2004, available at 2004 WLNR 4854116.
Fitzgerald was chosen with the third pick of the 2004 Draft and has had a stellar career with the Arizona Cardinals.
1580
See Clarett v. Nat’l Football League, 306 F.Supp.2d 379, 387 (S.D.N.Y. 2004), rev’d 369 F.3d 124 (2d Cir. 2004).
1581
See id.
1582
Clarett v. Nat’l Football League, 369 F.3d 124 (2d Cir. 2004).
1583
See South Carolina’s Jadeveon Clowney is Heisman frontrunner, Augusta Chronicle (GA), Aug. 11, 2013,
available at 2013 WLNR 19791739.
1584
Michael David Smith, Clowney sees himself as the No. 1 overall pick, ProFootballTalk (Feb. 6, 2014, 3:17 PM),
http://profootballtalk.nbcsports.com/2014/02/06/clowney-sees-himself-as-the-no-1-overall-pick/, archived at
http://perma.cc/T8FW-T28R (“Clowney almost certainly would have been the No. 1 overall pick in the 2013 NFL draft
if not for the NFL’s rule requiring players to be at least three years out of high school before they enter the draft.”)
1585
Mike Florio, Clowney passes on one game, Spurrier goes passive aggressive, ProFootballTalk (Oct. 6, 2013,
10:16 AM), http://profootballtalk.nbcsports.com/2013/10/06/clowney-passes-on-one-game-spurrier-goes-passive-
aggressive/, archived at http://perma.cc/2LJ4-WVND; Michael David Smith, Clowney: I’m fully committed, not thinking
about the NFL draft, ProFootballTalk (Oct. 6, 2013, 6:36 PM),
http://profootballtalk.nbcsports.com/2013/10/08/clowney-im-fully-committed-to-my-team-not-thinking-about-the-nfl/,
archived at http://perma.cc/9F2K-QUES.
1586
See Curtis Crabtree, Warren Sapp jumps on bandwagon of Jadeveon Clowney criticism, ProFootballTalk (Apr.
22, 2014, 1:33 AM), http://profootballtalk.nbcsports.com/2014/04/22/warren-sapp-jumps-on-bandwagon-of-jadeveon-
clowney-criticism/, archived at https://perma.cc/J4UR-ERK6; Michael David Smith, Mayock: Clowney can be the best
player in the NFL, if he wants it, ProFootballTalk (Apr. 23, 2014, 1:25 PM),
http://profootballtalk.nbcsports.com/2014/04/23/mayock-clowney-can-be-the-best-player-in-the-nfl-if-he-wants-it/,
archived at http://perma.cc/T5N6-696B.
1587
Rich Gosselin, Injured college stars have NFL value, Dallas Morning News, Sept. 20, 2002, available at 2002
WLNR 13720468.
1588
The SEC is widely regarded as the best college football conference. After the SEC, which is the best conference
in college football? NAT’L COLLEGIATE ATHLETICS ASS’N, Sept. 2, 2014, http://www.ncaa.com/news/football/head-
head/2014-08-22/after-sec-which-best-conference-college-football, archived at http://perma.cc/8JN2-AHAR; Clay
Travis, The SEC Is Dead, Long Live the SEC, FOX SPORTS, Jan. 5, 2015, http://www.foxsports.com/college-
football/outkick-the-coverage/the-sec-is-dead-long-live-the-sec-010515, archived at http://perma.cc/6C3W-LJVG.
1589
Cindy Boren, 49ers’ Marcus Lattimore considering retirement, Wash. Post, Nov. 3, 2014, available at 2014 WLNR
30777868.
1590
Cindy Boren, 49ers’ Marcus Lattimore retires, ends longshot NFL career before it even began, Wash. Post, Nov.
5, 2014, available at 2014 WLNR 31019273.
1591
Drawing on Lattimore’s story, some recommended that Leonard Fournette, a star running back at LSU, not play
his 2016 college season to avoid the risk of injury before becoming eligible for the 2017 NFL Draft. See Mike Florio,
Fournette definitely should take a year off in 2016, ProFootballTalk (Sept. 30, 2015, 9:33 AM),
http://profootballtalk.nbcsports.com/2015/09/30/fournette-definitely-should-take-a-year-off-in-2016/, archived at
https://perma.cc/5XL4-6NJ4. Instead, Fournette obtained $20 million in insurance policies and played in the 2016
season. Mike Florio, Leonard Fournette gets a pair of insurance policies, ProFootballTalk (May 12, 2016, 10:05 PM),
http://profootballtalk.nbcsports.com/2016/05/12/leonard-fourtnette-gets-a-pair-of-insurance-policies/, archived at
https://perma.cc/2R2M-5DWK.
1592
Id.
1593
See What is average NFL player’s career length? Longer than you might think, Commissioner Goodell says, Nat’l
Football League, Apr. 18, 2011, http://nflcommunications.com/2011/04/18/what-is-average-nfl-player%E2%80%99s-

!
284!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
career-length-longer-than-you-might-think-commissioner-goodell-says/, archived at http://perma.cc/8UHQ-JMVX
(discussing dispute between NFLPA’s assertion that the average career is 3.5 years and the NFL’s assertion that the
average career is 6 years); Average NFL Career Length, Sharp Football Analysis, Apr. 30, 2014,
http://www.sharpfootballanalysis.com/blog/?p=2133, archived at http://perma.cc/4EZY-E7ML (discussing
disagreement between NFLPA and NFL and determining that the average drafted player plays about 5 years).
1594
2011 NFL CBA, Art. 7, § 3.
1595
An Unrestricted Free Agent is a “player with four or more Accrued Seasons [who]… at the expiration of his Player
Contract… shall be completely free to negotiate and sign a Player Contract with any Club, and any Club shall be
completely free to negotiate and sign a Player Contract with such player without penalty or restriction[.]” 2011 NFL
CBA, Art. 9, § 1(a).
1596
Chris Deubert, Glenn M. Wong, John Howe, All Four Quarters: A Retrospective and Analysis of the 2011
Collective Bargaining Process and Agreement in the National Football League, 19 UCLA Ent. L. Rev. 1, 52-61
(2012).
1597
Id.
1598
See Willie T. Smith III, For the love of Mike, Greenville News (Greenville, SC), Aug. 24, 2014, available at
2014 WLNR 23306853 (South Carolina head coach Steve Spurrier saying he would recommend running back Mike
Davis enter the NFL because “The lifespan of a running back is only a certain number of years.”); Paolo Bovin,
Cardinals, RB Gordon appear to be perfect fit, Ariz. Republic, Apr. 26, 2015, available at 2015 WLNR 12199272
(discussing the short “lifespan” on NFL running backs); Evan Woodbery, Hightower still pursuing a dream, Hopes for
comeback rest with the Saints, New Orleans Times Picayune, Feb. 15, 2015, available at 2015 WLNR 4668527
(same); Greg Logan, Johnson a good fit in Jets’ Attack, Newsday, Sept. 20, 2014, available at 2014 WLNR 26127868
(discussing the “tread” on veteran running back Chris Johnson’s “tires”).
1599
See Mike Chappell, Chancy Proposition: Underclassmen who Enter Draft Weigh the Risks; Colts’ Bashir Doesn’t
Regret Leaving School, Indianapolis Star, Apr. 14, 2002, at C1; John McClain, ‘Bama’s Palmer to Enter Draft
Now/All-America Receiver Alters Decision, Hous. Chron., Jan. 11, 1994, available at 1994 WLNR 4953475.
1600
See Brent Schrotenboer, Dad: Brown Will Be Back in Scarlet and Black in 2010, San Diego Union-Trib., Jan. 16,
2010, http://www.sandiegouniontribune.com/news/2010/jan/16/dad-brown-will-be-back-scarlet-and-black-10/,
archived at https://perma.cc/GU6Z-WFP6 (discussing decision of San Diego State wide receiver Vincent Brown to
return for his senior season after receiving a projection that he would not be taken in the first three rounds).
1601
See Scott Hotard, LSU’s Black a Forgotten Man by NFL, Baton Rouge Advoc., May 3, 2010, available at 2010
WLNR 9154729; Manish Mehta, Warren Steps Up for Jets, Star-Ledger (Newark, N.J.), May 1, 2010, available at
2010 WLNR 9064474.
1602
Albert Breer, NFL implementing changes to address underclassmen issue, Nat’l Football League, Jul. 18, 2014,
http://www.nfl.com/news/story/0ap2000000365987/article/nfl-implementing-changes-to-address-underclassmen-
issue, archived at https://perma.cc/M7BM-DYL7.
1603
Id.
1604
Michael David Smith, 24 early entries went undrafted, ProFootballTalk (May 3, 2015, 4:49 PM),
http://profootballtalk.nbcsports.com/2015/05/03/24-early-entries-went-undrafted/, archived at https://perma.cc/XKE3-
42AS.
1605
Zac Jackson, 30 early entrants go undrafted, ProFootballTalk (Apr. 30, 2016, 7:21 PM),
http://profootballtalk.nbcsports.com/2016/04/30/30-early-entries-go-undrafted/, archived at https://perma.cc/8UVC-
4PQH.
1606
It is important to know that while many (if not most) of the players who left college early did so because they
thought they had the skill necessary to play in the NFL, at least some were likely forced to leave college for
academic, personal, or institutional reasons.
1607
See Average NFL Career Length, Sharp Football Analysis, Apr. 30, 2014,
http://www.sharpfootballanalysis.com/blog/?p=2133, archived at http://perma.cc/4EZY-E7ML (showing that drafted
players tend to have longer careers).
1608
NCAA Division I Manual, Bylaw 12.2.4.2.3 (providing that a football student-athlete can only return to college
football if “the student-athlete declares his intention to resume intercollegiate participation within 72 hours following
the National Football League draft declaration date.”)
1609
See Unofficial underclassmen early entry list for 2015 NFL Draft, Nat’l Football League, Jan. 2, 2015,
http://www.nfl.com/news/story/0ap3000000441827/article/unofficial-underclassmen-early-entry-list-for-2015-nfl-draft,
archived at http://perma.cc/SD8M-PUXV.
1610
Some college coaches have expressed their disappointment in not permitting undrafted underclassmen the
opportunity to return to college football. See Mike Florio, Should undrafted underclassmen be allowed to return to
college? ProFootballTalk (May 11, 2016, 11:50 AM), http://profootballtalk.nbcsports.com/2016/05/11/should-
undrafted-underclassmen-be-allowed-to-return-to-college/, archived at https://perma.cc/J9RY-ZJH5.
1611
See Clarett v. Nat’l Football League, 306 F.Supp.2d 379, 408 (S.D.N.Y. 2004), rev’d 369 F.3d 124 (2004).
1612
The “United States” includes “the 50 States of the United States of America, the District of Columbia, Puerto Rico,
and any other Commonwealth, Territory or Possession of the United States.” Major League Rule 3(a)(1). Additionally,

!
285!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
a “resident of the United States” includes anyone who “enrolls in a United States high school or college or establishes
a legal residence in the United States on the date of the player’s contract or within one year prior to that date.” Major
League Rule 3(a)(1)(A).
1613
Minor league baseball generally refers to lower levels of baseball in which players almost always play before
reaching MLB. Minor League Baseball (“MiLB”) is an organization of 15 different minor leagues with 176 teams,
almost all of which are affiliated with an MLB club. See General History, MINOR LEAGUE BASEBALL,
http://www.milb.com/milb/history/general_history.jsp (last visited June 23, 2016), archived at http://perma.cc/2WHA-
44D2. In addition to MiLB, there are independent minor leagues that are not affiliated with MLB or MLB clubs in any
way.
1614
In addition to the CBA, many of MLB’s rules are set out in a document entitled Major League Rules. Many of the
Major League Rules have not been collectively bargained with the MLBPA, but the CBA does mention and amend
some of the Rules. To the extent the Major League Rules and CBA conflict, the CBA controls.
1615
The Major League Rules are not the CBA and are not necessarily collectively bargained with the MLBPA. While
the CBA mentions multiple Major League Rules, and news reports indicate that changes to the Rule 4 Draft resulted
from negotiations of the 2011 CBA, see MLB, MLBPA reach new five-year labor agreement, MAJOR LEAGUE BASEBALL,
Nov. 22, 2011, http://m.mlb.com/news/article/26025138/, archived at http://perma.cc/48JZ-CUHX. MLB’s eligibility
rules are not an explicit part of the CBA and thus might be slightly more prone to an antitrust attack as compared to
the eligibility rules of the NFL, NBA, NHL, and CFL for the reasons discussed in the Introduction of this Chapter.
1616
Major League Rule 3(a)(2)(A).
1617
See, e.g., Eligibility Guide for Participation in High School Athletics, Ohio High School Athletic Ass’n, June 8,
2014, http://www.ohsaa.org/eligibility/EligibilityGuideHS.pdf, archived at http://perma.cc/5MAB-Q64V.
1618
Major League Rule 3(a)(2)(A)(i)–(iii).
1619
Major League Rule 3(a)(2)(A).
1620
Draft 2016 – Draft Tracker, Major League Baseball, http://m.mlb.com/draft/tracker/#!ft=round&fv=1 (last visited
Feb. 7, 2017), archived at https://perma.cc/2YGN-JDAK.
1621
For purposes of the Major League Rules, a “college” is an institution that confers four-year degrees and is
“represented by a baseball team which participates in inter-collegiate competition,” a definition that “includes but is
not limited to all members of the NCAA and the National Association of Intercollegiate Athletics (“NAIA”).” Major
League Rule 3(a)(3)(A).
1622
Major League Rule 3(a)(3)(B).
1623
A college player seeking eligibility because he was terminated due to scholastic deficiency must apply to the
Commissioner for eligibility. Major League Rule 3(a)(3)(F)(i).
1624
Major League Rule 3(a)(3)(E)(i)–(v).
1625
First-Year Player Draft, Major League Baseball, http://mlb.mlb.com/mlb/draftday/rules.jsp (last visited Oct. 24,
2016), archived at https://perma.cc/RA2T-A8YN.
1626
It is even possible to be drafted four times. Some players go from high school to junior college, where you can be
drafted after your second year. Hypothetically, a player could be drafted after high school, enter a junior college and
be drafted after junior college, then enroll in a four-year college, be drafted after his junior year, and be drafted a
fourth time after graduating from, or completing his eligibility at, the four-year college.
1627
Matt Youmans, Harper ready to give college try, Las Vegas Rev.-J., Jun. 14, 2009,
http://www.reviewjournal.com/sports/harper-ready-give-college-try, archived at http://perma.cc/452J-6DPK.
1628
See Major League Rule 4(a) (restricting Rule 4 Draft eligibility).
1629
Major League Rule 3(a)(1)(B)(i)–(ii).
1630
Craig Calcaterra, Opening Day Rosters Have 238 Players Born Outside of the United States, Hardball Talk (Apr.
4, 2016, 4:44 PM), http://mlb.nbcsports.com/2016/04/04/opening-day-rosters-have-238-players-born-outside-of-the-
united-states/, archived at https://perma.cc/AP4J-4PLY.
1631
Id.
1632
Matt Kalthoff, Out of Sight, Out of Mind: Confronting the Legal, Economic and Social Issues Raised by Major
League Baseball’s Peculiar Treatment of Foreign Talent, 29 Conn. J. Int’l L. 353, 360-65 (2014) (describing the
buscon industry).
1633
Id.
1634
Id.
1635
Id.
1636
See id.; Dustin Williamson, Part of the Team: Building Closer Relationships Between MLB Teams and
Independent Agents in the Dominican Republic Through an MLB Code of Conduct, 2 NYU J. Intell. Prop. & Ent. L.
369 (2013); Rick J. Lopez, Signing Bonus Skimming and a Premature Call for a Global Draft in Major League
Baseball, 41 Ariz. St. L.J. 349 (2009).
1637
2012 MLB CBA Attachment 46 § I(A).
1638
Id. § I(D)(2).

!
286!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1639
International Talent Committee to seek input from foreign baseball experts, Major League Baseball, Jan. 18,
2012, http://m.mlb.com/news/article/26379998/international-talent-committee-to-seek-input-from-foreign-baseball-
experts, archived at http://perma.cc/82KF-4ZNY.
1640
Craig Calcaterra, Report: MLB, Union Negotiating the Implementation of An International Draft, Hardball Talk
(Oct. 17, 2016, 4:23 PM), http://mlb.nbcsports.com/2016/10/17/report-mlb-union-negotiating-the-implementation-of-
an-international-draft/, archived at https://perma.cc/4GGM-DGNV.
1641
MLBPA, MLB Announce Details of New Labor Agreement, MLBPA (Dec. 2, 2016),
http://www.mlbplayers.com/ViewArticle.dbml?DB_OEM_ID=34000&ATCLID=211336390, archived at
https://perma.cc/4XUA-2DAW
1642
Id.
1643
Players drafted in the Rule 4 Draft must sign minor league contracts. See MLB, MLBPA reach new five-year labor
agreement, Major League Baseball, Nov. 22, 2011, http://m.mlb.com/news/article/26025138/, archived at
http://perma.cc/48JZ-CUHX.
1644
Matt Eddy, One In Six Picks Will Click On Trek From Draft To Majors, Baseball Am., Jul. 22, 2013,
http://www.baseballamerica.com/draft/one-in-six-draft-picks-will-click/, archived at http://perma.cc/X89T-7K2M.
1645
See Michael McCann, In lawsuit minor leaguers charge they are members of ‘working poor’, Sports Illustrated,
Feb. 12, 2012, http://www.si.com/mlb/2014/02/12/minor-league-baseball-players-lawsuit, archived at
http://perma.cc/A89J-YTHJ (discussing lawsuit brought by minor league players against MLB concerning their
wages).
1646
2012 MLB CBA, Art. VI, § A(1).
1647
Michael McCann, In lawsuit minor leaguers charge they are members of ‘working poor’, Sports Illustrated, Feb.
12, 2012, http://www.si.com/mlb/2014/02/12/minor-league-baseball-players-lawsuit, archived at http://perma.cc/A89J-
YTHJ.
1648
NCAA Division I Manual, § 12.1.2 (“An individual loses amateur status and thus shall not be eligible for
intercollegiate competition in a particular sport if the individual… [e]nters into an agreement with an agent.”).
1649
An “‘international player’ is a player: (i) who has maintained permanent residence outside of the United States for
at least the three (3) years prior to the Draft while participating in the game of basketball as an amateur or as a
professional outside of the United States; (ii) who has never previously enrolled in a college or university in the United
States; and, (iii) who did not complete high school in the United States.” 2017 NBA CBA Art. X § 1(c).
1650
See 2017 NBA CBA, Art. X § 1(b)(i).
1651
Id.
1652
As a result of this specific rule, some players can be eligible for the NBA Draft by intentionally not graduating from
high school. For example, prior to the 2016 NBA Draft, it was reported that Jonathan Isaac, a high school player, was
considering going straight from high school to the NBA. Isaac was in his 5th year of high school and thus the class
with which Isaac entered high school had already graduated. Provided Isaac did not complete high school, he would
have been eligible for the 2016 NBA Draft. Nevertheless, Isaac ultimately chose to attend college instead. See Dan
Feldman, Will Jonathan Isaac Jump from High School to NBA Draft?, Pro Basketball Talk (Feb. 11, 2016, 10:40 PM),
http://nba.nbcsports.com/2016/02/11/will-jonathan-isaac-jump-from-high-school-to-nba-draft/, archived at
https://perma.cc/XPB4-NYYB. Had Isaac graduated from high school but did not enroll in college, he would have had
to wait four calendar years until he would be eligible for the Draft. 2017 NBA CBA, Art. X, § 1(b)(ii)(C).
1653
See 2017 NBA CBA, Art. X § 1(b)(ii)(A)-(G).
1654
See 2017 NBA CBA, Art. X § 1(b)(i).
1655
!2017!NBA!CBA,!Art.!X,!§!(1)(b)(ii)(G).!
1656
Denver Rockets v. All-Pro Management, Inc., 325 F.Supp. 1049, 1055 (C.D.Ca. 1971).
1657
The ABA was a professional basketball league that attempted to compete against the NBA from 1967–1976. See
Remember the ABA - Home, Remember the ABA, http://www.remembertheaba.com/ (last visited Sept. 24, 2015),
archived at http://perma.cc/WR9N-DME8. When the ABA folded, four of its clubs (New York Nets, Denver Nuggets,
Indiana Pacers, and San Antonio Spurs) merged into the NBA. Id.
1658
Denver Rockets, supra n. 1656 at 1060.
1659
See id. at 1067.
1660
Denver Rockets v. All-Pro Management, Inc., 71-cv-1089, 1971 WL 3015 (9th Cir. Feb. 16, 1971).
1661
Haywood v. Nat’l Basketball Ass’n, 401 U.S. 1204 (1971).
1662
How NBA Policy Changed, Seattle Times, Oct. 29, 1997, available at 1997 WLNR 1485502.
1663
Id.
1664
Moses Malone (1974), Darryl Dawkins (1975), and Bill Willoughby (1975) were the only players to join the NBA
straight from high school in the years immediately following the Haywood case. High School Star Seeks Jump to
NBA, Orlando Sentinel, May 12, 1995, available at 1995 WLNR 4649503.
1665
See id.
1666
This information was provided by the NBA.
1667
The players would have been unable to pursue college basketball if they had signed an agreement with an agent,
see NCAA Division I Manual, § 12.1.2 (“An individual loses amateur status and thus shall not be eligible for

!
287!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
intercollegiate competition in a particular sport if the individual… [e]nters into an agreement with an agent.”). Most, if
not all, of the players signed with agents in hopes of increasing their chances of being drafted.
1668
See Roscoe Nance, Teen draftees grounded until 19 under new deal, USA Today, Jun. 22, 2005, available at
2005 WLNR 9883069.
1669
Id.
1670
See Tim Sullivan, You can blame NCAA for a lot, but not for the one-and-done rule, Courier-J. (Louisville, KY),
Mar. 6, 2014, available at 2014 WLNR 6290752; Bill Dwyre, One-and-done shouldn’t be satisfying to anyone, L.A.
Times, Apr. 11, 2009, available at 2009 WLNR 6798286.
1671
Glenn M. Wong, Warren Zola, Chris Deubert, Going Pro in Sports: Providing Guidance to Student-Athletes in a
Complicated Legal & Regulatory Environment, 28 Cardozo Arts & Ent. L.J. 553, 578 (2011).
1672
Neil Greenberg, A look at how one-and-done players perform in the NBA, Wash. Post, Apr. 8, 2015,
http://www.washingtonpost.com/news/fancy-stats/wp/2015/04/08/a-look-at-how-one-and-done-players-perform-in-
the-nba/, archived at http://perma.cc/U5N4-ZJ9H (describing 68 players as having left college after only one season
beginning with the 2006 NBA Draft through the 2014 NBA Draft); There were 13 one-and-done players in the 2015
NBA Draft and 14 in the 2016 NBA Draft.
1673
Jim Vertuno, NCAA rule change to allow NBA evaluation flexibility, NBA (Jan. 13, 2016, 7:06 PM),
http://www.nba.com/2016/news/01/13/ncaa-convention-draft-status-flexibility/, archived at https://perma.cc/BR97-
U23T.
1674
Id.
1675
See Scott Cacciola, Australia Emerges as the New Front in the College Recruiting Wars, N.Y. Times, Nov. 12,
2016, https://www.nytimes.com/2016/11/13/sports/basketball/australia-college-basketball-recruiting.html, archived at
https://perma.cc/KC49-6WQ4.
1676
Dave Telep, NBA Star Jennings’ Advice to Aquille Carr, ESPN, Mar. 13, 2013,
http://insider.espn.go.com/blog/dave-telep/post/_/id/3311/nba-star-jennings-advice-to-aquille-carr, archived at
https://perma.cc/V8R6-B63E.
1677
Ethan Sherwood Strauss, A Moment of Clarity for Jeremy Tyler, ESPN, July 13, 2013,
http://espn.go.com/blog/truehoop/post/_/id/61544/a-moment-of-clarity-for-jeremy-tyler, archived at
http://perma.cc/V27B-N3WB.
1678
Tyler decided to leave high school after his junior year and play professional basketball in Israel and Japan until
he was NBA eligible. While Tyler eventually made it to the NBA as a second round NBA Draft pick in 2011, he was
not a successful NBA player and currently plays in China. As another example, in 2014, Emmanuel Mudiay from
Texas went to play in China rather than for an American college. Mudiay, who escaped from war in the Congo as a
child, chose playing overseas due to potential problems concerning the NCAA’s academic eligibility and amateurism
requirements. In the 2015 NBA Draft, Mudiay was selected with the seventh overall pick by the Denver Nuggets.
1679
Beginning with the 2017-18 season, the D-League will officially be known as the “G-League” as part of a
sponsorship agreement with Gatorade. Dan Feldman, D-League? It’s Now the G-League, Pro Basketball Talk (Feb.
14, 2016, 9:50 AM), http://nba.nbcsports.com/2017/02/14/d-league-its-now-the-g-league/, archived at
https://perma.cc/8KN3-GL8J.
1680
Frequently Asked Questions: NBA Development League, NBA Development League, http://dleague.nba.com/faq/
(last visited Feb. 3, 2017), archived at https://perma.cc/8QKN-VKYC.
1681
Id.
1682
NBA D-League FAQ, Nat’l Basketball League, http://www.nba.com/dleague/santacruz/dleague_faqs.html (last
visited Sept. 24, 2015), archived at http://perma.cc/34EW-7QVY.
1683
In 2009, Latavious Williams did go directly from high school to the D-League. However, Williams had little
choice—after committing to play at the University of Memphis, Williams could not meet NCAA academic requirements
to play.
1684
Id. Some NBA owners and analysts argue that the D-League should replace collegiate sports as the traditional
path for NBA players, but believe that the D-League must improve its incentives and competitiveness before this can
happen. See Time MacMahon, Cuban: D-League better for prospects, ESPN, Mar. 6, 2014,
http://espn.go.com/dallas/nba/story/_/id/10538276/mark-cuban-says-nba-d-league-better-option-ncaa, archived at
https://perma.cc/6FNR-Q3WC.
1685
Chris Reichert, Source: NBA D-League to change salary structure in 2016/17, Upside & Motor (2016),
http://upsidemotor.com/2016/07/15/nba-d-league-salary-money/, archived at https://perma.cc/C7H2-N2UQ.
1686
Players that entered the D-League would be ineligible to play NCAA basketball.
1687
Art Tellem, Turn One-and-Done Into None-and-Done, N.Y. Times, Jun. 28, 2014,
http://www.nytimes.com/2014/06/29/sports/basketball/turn-one-and-done-into-none-and-done.html, archived at
http://perma.cc/KQ4Z-36R4.
1688
Kiki VanDeweghe, N.B.A. Eligibility Rule Is Good for the Game, N.Y. Times, Jul. 12, 2014,
http://www.nytimes.com/2014/07/13/sports/basketball/nba-eligibility-rule-is-good-for-the-game.html, archived at
http://perma.cc/WJ3U-CC2T.

!
288!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1689
See Zach Harper, Commissioner Adam Silver still wants age limit of 20 for draft eligibility, CBS Sports (Nov. 24,
2014, 7:38 PM), http://www.cbssports.com/nba/eye-on-basketball/24838071/commissioner-adam-silver-still-wants-
age-limit-of-20-for-draft-eligibility, archived at https://perma.cc/TX6U-QH6M; Steve Kerr, The Case for the 20-Year-
Old Age Limit in the NBA, Grantland, May 8, 2012, http://grantland.com/features/steve-kerr-problems-age-limit-nba/,
archived at https://perma.cc/BU6U-8T8R.
1690
NBPA leader Michele Roberts: ‘Be happy with one-and-done,’ Sports Illustrated, Feb. 15, 2015,
http://www.si.com/nba/2015/02/15/nba-age-limit-michele-roberts-adam-silver-one-and-done, archived at
http://perma.cc/38K7-QGUN.
1691
See David Aldridge, NBA, NBPA reach tentative seven-year CBA agreement, NBA.com (Dec. 14, 2016, 8:18
PM), http://www.nba.com/article/2016/12/14/nba-and-nbpa-reach-tentative-labor-deal, archived at
https://perma.cc/X5U4-YA73.
1692
2013 NHL CBA, Art. 8, § 8.4(a); NHL By-Law § 12.7.
1693
News reports have indicated that the NHL is considering trying to raise the minimum age to 19. See Allan Muir,
Notebook: Draft age change in store? SPORTS ILLUSTRATED (Mar. 8, 2016), http://www.si.com/nhl/2016/03/07/nhl-draft-
age-change-world-cup-over-35-team-players, archived at https://perma.cc/9L6C-8CL4.
1694
2013 NHL CBA, Art. 8, § 8.4(a).
1695
See Active NHL Players Totals by Nationality - Career Stats, QuantHockey.com,
http://www.quanthockey.com/nhl/nationality-totals/active-nhl-players-career-stats.html (last visited Nov. 30, 2016),
archived at https://perma.cc/8682-9DBY.
1696
Generally only about 20 players are drafted out of high schools each year, or about 10% of drafted players. See
Mike Morreale, NHL teams grab 20 high-schoolers in draft, Nat’l Hockey League (Jun. 23, 2010, 4:31 PM),
http://www.nhl.com/ice/news.htm?id=635956, archived at http://perma.cc/Q4ZR-VHC3; Mike Morreale, NHL teams
draft record 22 high school players, Nat’l Hockey League, Jun. 26, 2010,
http://www.nhl.com/ice/news.htm?id=533004, archived at http://perma.cc/PFZ4-GCW8.
1697
See Katie Strang, Lawsuit seeks to have junior players paid minimum wage, ESPN, Jan. 29, 2015,
http://espn.go.com/blog/nhl/post/_/id/34346/lawsuit-seeks-to-have-junior-players-paid-minimum-wage, archived at
https://perma.cc/5DAL-NPGU.
1698
NCAA Division I Manual Bylaw 12.2.3.2.4 (“Ice hockey teams in the United States and Canada, classified by the
Canadian Hockey Association as major junior teams, are considered professional teams under NCAA legislation.”)
1699
Andrew Podnieks, A Battle Across the Border in Recruiting, Feb. 9, 2011, N.Y. Times
http://www.nytimes.com/2011/02/10/sports/hockey/10hockey.html, archived at http://perma.cc/E9TP-UW5N.; Marc
Bianchi, Guardian of Amateurism or Legal Defiant? The Dichotomous Nature of NCAA Men’s Ice Hockey Regulation,
20 Seton Hall J. Sports & Ent. L. 165 (2010).
1700
Marc Bianchi, Guardian of Amateurism or Legal Defiant? The Dichotomous Nature of NCAA Men’s Ice Hockey
Regulation, 20 Seton Hall J. Sports & Ent. L. 165, 175 (2010).
1701
Andrew Podnieks, A Battle Across the Border in Recruiting, Feb. 9, 2011, N.Y. Times
http://www.nytimes.com/2011/02/10/sports/hockey/10hockey.html, archived at http://perma.cc/E9TP-UW5N.
1702
2013 NHL CBA, Art. 8, § 8.6(c).
1703
2013 NHL CBA, Art. 8, § 8.6(d).
1704
See, e.g., Aaron Portzline, Blue Jackets: Defenseman Mike Reilly to Return to College, Add to Game and Frame,
Columbus Dispatch, July 11, 2014, http://bluejacketsxtra.dispatch.com/content/stories/2014/07/11/still-room-for-
growth.html, archived at http://perma.cc/L3XW-HBT7 (explaining University of Minnesota’s Mike Reilly’s decision to
return to college to put on muscle after adding 36 pounds already in two years of college); Colin Dambrauskas,
Johnny Gaudreau Playing Big – Wants to Join Flames, HockeyBuzz (July 16, 2013, 12:35 p.m.),
http://www.hockeybuzz.com/blog/Colin-Dambrauskas/Johnny-Gaudreau-Playing-Big---Wants-to-Join-
Flames/171/52843, archived at http://perma.cc/9MZN-NSWC (quoting Calgary Flames’ prospect Johnny Gaudreau
as saying, “Hopefully they want me next year at the end of the year and hopefully I can come in and make an impact
for them. If I play well this year and put on the right weight, I think I might be able to do it.”) (emphasis added);
Lightning’s Jonathan Drouin Selected Top Prospect by NHL.com, Tampa Bay Lightning, Sept. 9, 2014,
http://lightning.nhl.com/club/news.htm?id=729872, archived at http://perma.cc/4R9A-X6DG (noting that David
Pastrnak will “need at least one more season in Sweden to get bigger and stronger” and that “[a]t 5-10 and 180
pounds . . . 18-year-old [Kevin Fiala] will need at least one more season with HV 71 in Sweden to get bigger and
stronger).
1705
NHL By-Law § 12.7.
1706
Neeld v. Nat’l Hockey League, 594 F.2d 1297, 1300 (9th Cir. 1979) (“the record amply supports the
reasonableness of the by-law”). Under the rule of reason, “the factfinder weighs all of the circumstances of a case in
deciding whether a restrictive practice should be prohibited as imposing an unreasonable restraint on competition,”
including “‘specific information about the relevant business’ and ‘the restraint’s history, nature, and effect.’” Leegin
Creative Leather Products, Inc. v. PSKS, Inc., 551 U.S. 877, 885 (2007) (citations omitted).
1707
Neeld, 594 F.2d at 1300. In addition to the Neeld case, there was a legal challenge to the age eligibility
requirements of professional hockey—albeit a challenge to the World Hockey Association (“WHA”), a 1970s

!
289!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
competitor of the NHL. In Linseman v. World Hockey Ass’n, 439 F. Supp. 1315 (D.Conn. 1977), 19-year-old Ken
Linseman challenged the WHA’s requirement that players be at least 20 years old. The United States District Court
for the District of Connecticut granted Linseman a preliminary injunction against the application of the rule, finding
that it was not “directed to any valid purpose.” Linseman played one year in the WHA before it folded in 1979.
1708
2014 CFL CBA, § 14.02.
1709
Id.
1710
CFL adjusts eligibility rules for Draft, Can. Football League, Sept. 6, 2013, http://cfl.ca/article/cfl-adjusts-eligibility-
rules-for-draft, archived at http://perma.cc/YWE9-J535.
1711
CIS By-laws, Policies and Procedures, § 40.10.4.1.3(c), available at http://en.cis-
sic.ca/information/members_info/bylaws_policies_procedures.
1712
Student-athletes red-shirt for several reasons: (1) as freshman, to allow for a transition to the athletic and
academic rigors of college; (2) due to an injury; and, (3) to improve their academic standing.
1713
CFL adjusts eligibility rules for Draft, supra n. 1710.
1714
Id.
1715
Murray McCormick, Forde heats up CFL draft talk, Postmedia News (Can.), May 9, 2014.
1716
See Greg Mancina, CFL drafts Saginaw Valley back, Saginaw News (Mich.), Oct. 3, 2008, available at 2008
WLNR 19073005.
1717
See Lowell Ullrich, Ullrich: CFL draft as mysterious as ever, Postmedia News (Can.), May 12, 2014 (discussing
changes to CFL Draft structure); Murray McCormick, Forde heats up CFL draft talk, Postmedia News (Can.), May 9,
2014.
1718
See id.
1719
See Pete Thamel, Bryce Brown to the C.F.L.?, N.Y. Times, Feb. 4, 2009, available at
http://thequad.blogs.nytimes.com/2009/02/04/bryce-brown-to-the-cfl/?_r=0, archived at http://perma.cc/3DPM-XSY5.
1720
Id.
1721
See Players, Major League Soccer, http://www.mlssoccer.com/players?sort=age&order=ASC (last visited June
23, 2016), archived at https://perma.cc/8Y7N-FQEW; see also Paul Tenorio Young stars increasingly on fast track,
Wash. Post, Apr. 14, 2010, available at 2010 WLNR 26726087 (discussing lack of age requirement in MLS and the
number of teenage players).
1722
See Jenna Merten, Raising a Red Card: Why Freddy Adu Should Not Be Allowed to Play Professional Soccer, 15
Marq. Sports L. Rev. 205 (2004).
1723
Roster Rules and Regulations, Major League Soccer, http://pressbox.mlssoccer.com/content/roster-rules-and-
regulations (last visited May 18, 2015), archived at http://perma.cc/48QQ-VC4S.
1724
Although it is called the “SuperDraft,” the SuperDraft is simply MLS’ draft.
1725
“Generation adidas is a joint program between MLS and adidas that is dedicated to developing exceptional
domestic talent in a professional environment. Each year, a handful of top domestic collegiate underclassmen and
youth national team players are signed by the league and placed in the SuperDraft through this program.” Generation
adidas players may also receive an education stipend. Importantly, Generation adidas players are on a club’s
Supplemental Roster and are not charged against the team’s salary budget. Roster Rules and Regulations, § II(C),
MLS.com, http://pressbox.mlssoccer.com/content/roster-rules-and-regulations (last visited May 18, 2015), archived at
http://perma.cc/48QQ-VC4S. Generation adidas is designed to prevent the best underclassmen from going to play in
Europe. Brooke Tunstall, Does MLS Block College Underclassmen from Draft?, AM. SOCCER NOW (Jan 17, 2014, 6:39
PM), http://americansoccernow.com/articles/does-mls-block-college-underclassmen-from-draft, archived at
http://perma.cc/3862-WDCR. As a result of the Generation adidas program, generally only players who have
exhausted their collegiate eligibility are nominated to be in the SuperDraft. Roster Rules and Regulations, supra. The
impact of the Generation adidas program is also discussed in Chapter 3: Health-Related Benefits.
1726
Id.
1727
Avi Creditor, A look inside the MLS discovery process, Goal (Feb 26, 2013 1:00 AM), http://www.goal.com/en-
us/news/1110/major-league-soccer/2013/02/26/3780299/avi-creditor-a-look-inside-the-mls-discovery-process,
archived at https://perma.cc/8VQP-9A8C.
1728
Roster Rules and Regulations, MLS.com, http://pressbox.mlssoccer.com/content/roster-rules-and-regulations
(last visited May 18, 2015), archived at http://perma.cc/48QQ-VC4S.
1729
L. E. Eisenmenger, McCabe Explains Generation adidas, U.S. Soccer Players, Jan. 8, 2010,
http://www.ussoccerplayers.com/2010/01/mccabe-explains-generation-adidas.html, archived at
http://perma.cc/CS4G-2QY5 (quoting an MLS player agent as saying: “The challenge is how to keep players here in
the MLS. The only way is to overpay a little bit to keep them.”) The education related benefits of the Generation
adidas program are also discussed in Chapter 3: Health-Related Benefits.
1730
As a reminder and as discussed in the Introduction, Section F: Scope, we define health for purposes of this
Report as “a state of overall wellbeing in fundamental aspects of a person’s life, including physical, mental, emotional,
social, familial, and financial components.”
1731
On this point, it is interesting to note that in Europe, soccer and basketball players often begin playing
professionally in their mid-to-late teens. See, e.g., Next Generation 2015: 50 of the best young talents in world

!
290!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
football, The Guardian, Oct. 7, 2015, http://www.theguardian.com/football/ng-interactive/2015/oct/07/next-generation-
2015-50-of-the-best-young-talents-in-world-football, archived at https://perma.cc/PTR6-T8SJ; Lang Whitaker, Here’s
Footage of 14-Year-Old Ricky Rubio, NBA.com (Nov. 7, 2014, 10:22 AM),
http://allball.blogs.nba.com/2014/11/07/heres-footage-of-14-year-old-ricky-rubio/, archived at https://perma.cc/WK5W-
R777.
1732
Glenn M. Wong, Warren Zola, Chris Deubert, Going Pro in Sports: Providing Guidance to Student-Athletes in a
Complicated Legal & Regulatory Environment, 28 Cardozo Arts & Ent. L.J. 553, 577 (2011).
1733
Neil Greenberg, A look at how one-and-done players perform in the NBA, Wash. Post, Apr. 8, 2015,
http://www.washingtonpost.com/news/fancy-stats/wp/2015/04/08/a-look-at-how-one-and-done-players-perform-in-
the-nba/, archived at http://perma.cc/U5N4-ZJ9H (describing 68 players as having left college after only one season
beginning with the 2006 NBA Draft through the 2014 NBA Draft); There were 13 one-and-done players in the 2015
NBA Draft and 14 in the 2016 NBA Draft.
1734
Indeed, there has been some research on this issue. An analysis of first-round draft picks from 1989–2000 by
Ryan Rodenberg and Jun Woo Kim concluded that “players who are drafted at a younger age relative to other
draftees have, on average, more successful NBA careers.” Moreover, the authors concluded that “there is no
evidence that players who played one year of college basketball, while controlling for other factors, perform better
than individuals who moved into the NBA straight from high school.” Ryan Rodenberg and Jun Woo Kim, Testing the
On-Court Efficacy of the NBA’s Age Eligibility Rule, 8 J. QUANTITATIVE ANALYSIS IN SPORTS 1 (2012). While this
analysis is interesting, some might argue that it does not address one of the core purposes of the eligibility rule:
preventing young men who give up their eligibility to play at the college level by entering the Draft early from having
their careers derailed by being drafted in the second round or not drafted at all.
1735
Ohm Youngmisuk, Adam Silver: Age issue ‘needs to be studied’ outside CBA negotiations, ESPN (Feb. 19, 2017,
12:10 PM), http://www.espn.com/nba/story/_/id/18715853/nba-commissioner-adam-silver-says-age-issue-worth-
looking-deeper-cba, archived at https://perma.cc/SB5P-H549.
1736
See Bartlett H. McGuire, Age Restrictions in Women’s Professional Tennis: A Case Study of Procompetitive
Restraints of Trade, 1 J. Int’l Media & Ent. L. 199 (2007).
1737
Id. at 207.
1738
Id. at 207–08.
1739
Bartlett, supra n. 1736, at 209.
1740
Id.
1741
WTA 2016 Official Rulebook, § XV.
1742
Bartlett, supra n. 1736, at 211–12.
1743
Id. at 217–18.
1744
For example, in 2007, the Houston Texans drafted Amobi Okoye with the tenth overall pick at the age of 19.
Okoye, originally from Nigeria, began college at the age of 15 in light of his academic performance. See Steve E.
Cavezza, “Can I See Some ID?”: An Antitrust Analysis of NBA and NFL Draft Eligibility Rules, 2010 DEN. U. SPORTS &
ENT. L.J. 22, 50–51 (2010).
1745
Given more advances in health technology, it is theoretically possible that leagues could adopt an individualized
approach, using specific metrics to determine whether a particular player was “ready.” However, such an approach
also raises concerns with the Americans with Disabilities Act and the Genetic Information Nondiscrimination Act, as
discussed in our article, Evaluating NFL Player Health and Performance: Legal and Ethical Issues, 165 U. Penn. L.
Rev. 227 (2017).
1746
Despite criticism on this issue, the NFL reportedly is not considering any changes to its eligibility rules. See Mike
Florio, NFL not considering a change to the three-year rule, ProFootballTalk (Oct. 31, 2015, 10:38 PM),
http://profootballtalk.nbcsports.com/2015/10/31/nfl-not-considering-a-change-to-the-three-year-rule/, archived at
https://perma.cc/34JC-M66Y.
1747
As explained in the Introduction, Section F: Scope, we define health for purposes of this Report as “a state of
overall wellbeing in fundamental aspects of a person’s life, including physical, mental, emotional, social, familial, and
financial components.”
1748
2011 NFL CBA, Art. 45, § 2.
1749
An Injury Grievance is “a claim or complaint that, at the time a player’s NFL Player Contract or Practice Squad
Player Contract was terminated by a Club, the player was physically unable to perform the services required of him
by that contract because of an injury incurred in the performance of his services under that contract.” 2011 NFL CBA,
Art. 45, § 1.
1750
See Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of
NFL Players: Legal and Ethical Analysis and Recommendations, Recommendation 1:1-F (2016).
1751
In our Report Protecting and Promoting the Health of NFL Players: Legal and Ethical Analysis and
Recommendations we set forth a comprehensive recommendation to address this issue. We propose restructuring
NFL club medical staff in such a way that the doctor treating the players has as his or her only concern the well-being
of the player-patient and has no advisory role to the club.

!
291!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1752
See Am. Acad. Pediatrics, Preparticipation Physical Evaluation (4th ed. 2010). This monograph was created
through the coordination of the American Academy of Family Physicians, American Academy of Pediatrics, American
College of Sports Medicine, American Medical Society for Sports Medicine, American Orthopaedic Society for Sports
Medicine, and the American Osteopathic Academy of Sports Medicine.
1753
Am. Acad. Pediatrics, Preparticipation Physical Evaluation 3 (4th ed. 2010).
1754
For examples of such studies in high school and college sports, see Barry P. Boden et al., Catastrophic Injuries in
Pole Vaulters, A Prospective 9-Year Follow-up Study, 40 Am. J. Sports Med. 1488 (2012); Frederick O. Mueller and
Robert C. Cantu, Catastrophic injuries and fatalities in high school and college sports, fall 1982–spring 1988, 22 Med.
& Sci. in Sports & Exercise 737 (1990).
1755
Some of the studies discussed in this Report were the result of the leagues’ willingness to provide some injury
data upon request. While it is commendable that the leagues occasionally provide the data when requested, this does
not entirely address the concerns outlined in Recommendation 1.
1756
Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations, Recommendation 17:1-B (2016).
1757
See The Datalys Center for Sports Injury Research and Prevention, NCAA, http://www.ncaa.org/health-and-
safety/medical-conditions/datalys-center-sports-injury-research-and-prevention (last visited Aug. 3, 2016), archived at
https://perma.cc/2M75-B24L.
1758
See, e.g., Data transparency, GlaxoSmithKline, http://www.gsk.com/en-gb/behind-the-science/innovation/data-
transparency (last visited June 20, 2016), archived at https://perma.cc/M5HN-NLHN; Frequently Asked Questions,
the YODA Project, http://yoda.yale.edu/frequently-asked-questions-faqs#Data (last visited June 20, 2016), archived
at https://perma.cc/2Z98-R7HC.
1759
This recommendation also appears as Recommendation 7:1-E in our Report Protecting and Promoting the Health
of NFL Players: Legal and Ethical Analysis and Recommendations. Due to the fact that the recommendation was
inspired by MLB’s concussion-specific DL list, we include it here as well.
1760
See Paul McCrory et al., Consensus statement on concussion in sport: the 4th Int’l Conference on Concussion in
Sport held in Zurich, November 2012, 47 Br. J. Sports Med. 250, 251 (2013).
1761
Id. at 253.
1762
2012 MLB CBA, Att. 36, ¶ 2.
1763
See Paul McCrory et al., Consensus statement on concussion in sport: the 4th Int’l Conference on Concussion in
Sport held in Zurich, November 2012, 47 Br. J. Sports Med. 250, 250–58 (2013) (discussing the challenges of and
best practices for diagnosing concussions).
1764
See id.
1765
See id. at 252-58 (discussing generally the challenges of determining when an athlete has recovered from a
concussion).
1766
We recognize that this new injured reserve list is subject to gaming by clubs, whereby a club might designate a
player as concussed in order to add another player and effectively expand the roster. We do not view this this
concern to be sufficient to outweigh the health benefits of the proposal. Moreover, all injury lists are subject to some
risk of being gamed in this manner, and thus the issue is not unique to what we propose.
1767
Letter from Larry Ferazani, NFL, to authors (July 18, 2016).
1768
Id.
1769
Mike Florio, NFL tells teams to stop commenting about concussed players, ProFootballTalk (Nov. 11, 2016, 7:50
PM), http://profootballtalk.nbcsports.com/2016/11/11/nfl-tells-teams-to-stop-commenting-about-concussed-players/,
archived at https://perma.cc/Z7ML-ZP7W.
1770
Id.
1771
Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of NFL
Players: Legal and Ethical Analysis and Recommendations Recommendation 7:4-B (2016).
1772
Mike Florio, Disclosure of injury information continues to put NFL players in a delicate spot, ProFootballTalk (July
10, 2015, 12:34 PM), http://profootballtalk.nbcsports.com/2015/07/10/disclosure-of-injury-information-continues-to-
put-nfl-players-in-a-delicate-spot/, archived at http://perma.cc/PYL4-KMRY (“many players would like to keep [injury
information] secret, in order to keep an opponent from hitting, poking, and/or kicking the injured region.”)
1773
For more on this issue, see Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and
Promoting the Health of NFL Players: Legal and Ethical Analysis and Recommendations, Recommendation 7:3-B
(2016).
1774
According to columnist Mike Freeman, the NFLPA did analyze the potential costs of providing NFL players with
health insurance for life and found the cost to be approximately $2 billion. Mike Freeman, Two Minute Warning: How
Concussions, Crime, and Controversy Could Kill the NFL (and What the League Can Do to Survive), xxv (2015).
1775
The principal distinction would be that employers require a certain number of years of service to, in part,
encourage employees to continue working for them rather than obtaining employment elsewhere. This incentive
structure is not needed in the NFL—where the vast majority of players play in the NFL for as long as they are able.
1776
Gene Upshaw, NFLPA’s Upshaw Responds, Wash. Post, Dec. 22, 2002, available at 2002 WLNR 15865309.

!
292!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1777
NFLPA, A New Look at Guaranteed Contracts in the NFL (circa 2002) (on file with authors) (“Over half of all
salary earned by NFL players now is guaranteed”); Nat’l Football League Players Ass’n, Guaranteed Contracts in
Professional Team Sports: How Does the NFL Compare? (circa 2007) (on file with authors) (“at least 52% of all
compensation in the NFL is, in fact, ‘guaranteed’ to players.’”)
1778
Mike Florio, Fully-guaranteed contracts could cause problems for teams, players, ProFootballTalk (May 29, 2015,
9:55 AM), http://profootballtalk.nbcsports.com/2015/05/29/fully-guaranteed-contracts-could-cause-problems-for-
teams-players/, archived at http://perma.cc/GE9E-YSME (discussing potential problems with guaranteed contracts in
the NFL).
1779
For example, one rule that would likely have to be removed is the NFL’s requirement that clubs deposit into a
separate account the present value, less $2 million, of guaranteed compensation to be paid in future years. 2011
CBA, Art. 26 § 9. Former NFL club executive Andrew Brandt believes clubs “hide behind” the funding rule to avoid
guaranteeing player compensation, and have been largely successful in doing so. Andrew Brandt, Supplemental
Peer Review Response (Nov. 6, 2015).
1780
See Christopher R. Deubert, I. Glenn Cohen, Holly Fernandez Lynch, Protecting and Promoting the Health of
NFL Players: Legal and Ethical Analysis and Recommendations, Recommendation 2:1-A (2016).
1781
Given more advances in health technology, it is theoretically possible that leagues could adopt an individualized
approach, using specific metrics to determine whether a particular player was “ready.” However, such an approach
also raises concerns with the Americans with Disabilities Act and the Genetic Information Nondiscrimination Act, as
discussed in our article, Evaluating NFL Player Health and Performance: Legal and Ethical Issues, 165 U. Penn. L.
Rev. 227 (2017).
1782
Despite criticism on this issue, the NFL reportedly is not considering any changes to its eligibility rules. See Mike
Florio, NFL not considering a change to the three-year rule, ProFootballTalk (Oct. 31, 2015, 10:38 PM),
http://profootballtalk.nbcsports.com/2015/10/31/nfl-not-considering-a-change-to-the-three-year-rule/, archived at
https://perma.cc/34JC-M66Y.
1783
As discussed above, when asked specifically about this issue, MLB directed us to its minimum game day
standards and the MLBTPA mission statement, both of which were discussed above. However, neither the game day
standards nor the mission statement sets forth a standard of care for club doctors specific to MLB club doctors or that
goes beyond what is already required by codes of ethics and relevant law applicable to all doctors. By comparison,
the NFL, NHL and MLS CBAs all set forth standards of care for their club doctors which, in particular, attempt to
address the conflict of interest inherent in having doctors that treat players while also providing services to the club.
1784
In reviewing a draft of this Report, MLB stated that our indication that MLB players do not have the right to the
surgeon of their choice was “inaccurate.” We disagree. As discussed above, while MLB clubs are directed to “take a
Player’s reasonable preferences into account when designating doctors to perform surgery,” “the Club has the right to
designate the doctors and hospitals when a Player is undergoing a surgery for an employment related injury[.]” 2012
MLB CBA, Attachment 35. In addition, “in no event should they force a Player to have a surgery performed by the
Club physician but should instead, in any case in which a Player has objected to the surgery being performed by the
Club physician, designate another physician to perform the surgery.” Id. Thus, the decision of which surgeon to use
ultimately rests with the club, subject to player’s ability to object to the club doctor performing the surgery.
1785
We remind the reader that we use the data that we consider the most reliable—and generally the most recent—in
order to provide the most accurate assessment of injury rates in sports today. We also remind the reader that our
data is limited to regular season data.
1786
As mentioned above, there was no publicly available data on CFL injuries.
1787
There is no recent data concerning player injuries in MLS.
1788
As mentioned above, UEFA is not a league but instead an organization of member clubs who participate in many
different leagues. Consequently, our review of UEFA here is constrained to injury data and does not include an
analysis of the policy issues covered in this Chart.
1789
This statistic includes injuries that occurred during regular season games, not practices, except for MLB. Data for
MLB only includes as injuries those injuries that caused a player to be placed on the Disabled List, regardless of the
reason the player was placed on the Disabled List. Nevertheless, we remind the reader that practices are infrequent
during the MLB regular season.
1790
The UEFA Report did not provide data on how many players played in the games for which injury data was
compiled and, due to the variations in season types and lengths among the different UEFA clubs, this figure is difficult
to calculate.
1791
This statistic only includes concussions that occurred during regular season games.
1792
It is unclear whether the CFL data concerning concussions includes pre-season or postseason games.
1793
The UEFA Report only provided data from a select number of clubs.
1794
MLS refuses to provide data on the number of concussions suffered by its players.
1795
Although some concussion data are available concerning the CFL, reliable data on the number of players per
season are not.

!
293!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1796
The UEFA Report did not provide data on how many players played in the games for which injury data was
compiled and, due to the variations in season types and lengths among the different UEFA clubs, this figure is difficult
to calculate.
1797
It is important to remember that this statistic is a relative statistic—it does not reflect the actual number of
concussions in the leagues.
1798
Here, we use the terminology from the studies relevant to each of the leagues—some identify the most common
injury while others identify the most commonly injured body part.
1799
We emphasize that this statistic is a mean of all player positions. As discussed in the full Report, we know that
rates vary depending on a player’s position. Unfortunately, we do not have sufficient data to do position-by-position
analysis. Nevertheless, even in the absence of that data we think the comparison of means is useful.
1800
For context, the NFL regular season is 16 games, the MLB regular season is 162 games, the NBA and NHL
regular seasons are 82 games, the CFL regular season is 18 games, and the MLS regular season is 34 games.
1801
See What is average NFL player’s career length? Longer than you might think, Commissioner Goodell says, Nat’l
Football League, Apr. 18, 2011, http://nflcommunications.com/2011/04/18/what-is-average-nfl-player%E2%80%99s-
career-length-longer-than-you-might-think-commissioner-goodell-says/, archived at http://perma.cc/8UHQ-JMVX
(discussing dispute between NFLPA’s assertion that the average career is 3.5 years and the NFL’s assertion that the
average career is 6 years); Average NFL Career Length, Sharp Football Analysis, Apr. 30, 2014,
http://www.sharpfootballanalysis.com/blog/?p=2133, archived at http://perma.cc/4EZY-E7ML (discussing
disagreement between NFLPA and NFL and determining that the average drafted player plays about 5 years).
1802
William D. Witnauer, Richard G. Rogers & Jarron M. Saint Onge, Major league baseball career length in the 20th
century, 26 Population Res. & Pol’y Rev. 4, 371-386 (2007).
1803
Susan Konig, Financial Planning for the Pros, 34 Registered Representative (Apr. 2010), available at 2010
WLNR 26366417.
1804
Average Length of an NHL Player Career, QuantHockey.com,
http://www.quanthockey.com/Distributions/CareerLengthGP.php (last visited Aug. 28, 2015), archived at
http://perma.cc/95QB-X9P9.
1805
Matthew Black, Players rely on education, experience after CFL career, Thunderbird, Mar. 31, 2011,
http://thethunderbird.ca/2011/03/31/players-bet-on-education-after-cfl-career/, archived at http://perma.cc/M92S-
KNQ8.
1806
Nick Schwartz, The average career earnings of athletes across America’s major sports will shock you, For the
Win Blog - USA Today (Oct. 24, 2013, 10:07 AM), http://ftw.usatoday.com/2013/10/average-career-earnings-nfl-nba-
mlb-nhl-mls, archived at http://perma.cc/J8QL-Q3RG. Nevertheless, as pointed by the MLPSU in its review of this
Report, the author of this article did not indicate how he arrived at the 3.2 years statistic. Moreover, MLSPU Executive
Director Bob Foose stated that “this number is significantly misleading given the global nature of soccer (there are, I
believe, professional leagues in over 80 countries around the world, typically with multiple such leagues in each
country). We have not consistently tracked the total average career length of MLS players, but when we last did an
exhaustive study, in 2013, the average MLS player (whose career was over) had played a total of just under 8.8
years of professional soccer over the course of that career. We haven’t updated these numbers since then, but I don’t
have any reason to believe that these numbers have changed significantly.” We believe this is a valid point and thus
suggest caution in considering the mean career length of MLS players. Athletes in the other leagues rarely play in
multiple professional leagues and thus the same concern is not present.
1807
2011 NBA, CBA, Art. IV, § 2(a).
1808
See Jay MacDonald, Professional Athletes’ Big-League Tax Bills, Fox Bus., Mar. 15, 2012,
http://www.foxbusiness.com/personal-finance/2012/03/15/professional-athletes-big-league-tax-bills/; Sean Hanley,
Estate Planning Attorney Guide for Retirement, Hanley Law (Aug. 21, 2013), http://hanleylaw.com/estate-planning-
attorney-retirement; Mark Riddix, Top Pro Athlete Pension Plans, Investopedia, July 16, 2010,
http://www.investopedia.com/financial-edge/0710/top-pro-athlete-pension-plans.aspx. See also Top 15 Sports
Organizations with the Best 401k Plans, BrightScope, June 25, 2013, http://blog.brightscope.com/2013/06/25/top-15-
sports-organizations-with-the-best-401k-plans/ (rating the plan as the best in professional sports, in part because of
generous contributions of NBA clubs).
1809
2011 CBA, Art. 39, § 3.
1810
Id.
1811
Black’s Law Dictionary (9th ed. 2009).
1812
29 U.S.C. § 1163(2).
1813
2011 CBA, Art. 45, § 1.
1814
2011 CBA, Art. 50, § 1.
1815
2013 NHL CBA, § 34.9.
1816
2004 MLS CBA, § 24.1.
1817
See Glenn M. Wong, Essentials of Sports Law, § 11.3 (4th ed. 2010) (providing history of the unions in the Big
Four sports leagues).
1818
Id.

!
294!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1819
Home, Major League Baseball Team Physicians Association, http://mlbtpa.org/ (last visited Aug. 25, 2015),
archived at http://perma.cc/2JTM-XMJ5.
1820
Home, MLS Team Physician Society, http://www.mlsteamdocs.com/ (last visited Aug. 26, 2015), archived at
http://perma.cc/QJ7E-82SN.
1821
Id.
1822
History, Nat’l Football League Players Ass’n, https://www.nflpa.com/about/history (last visited Aug. 7, 2015),
archived at https://perma.cc/3D2R-8EQG?type=pdf [hereinafter “NFLPA History”].
1823
About, Professional Baseball Athletic Trainers Society, http://pbats.com/about/ (last visited Aug. 25, 2015),
archived at http://perma.cc/G9FP-42CS.
1824
2012 MLB CBA, Art. XIII, § A(1).
1825
Voluntary Employee Beneficiary Association - 501(c)(9), IRS (Jan. 13, 2015), http://www.irs.gov/Charities-&-Non-
Profits/Other-Non-Profits/Voluntary-Employee-Beneficiary-Association-501%28c%29%289%29. The VEBA is funded
through 1% of Basketball Related Income. 2011 NBA CBA Art. IV § 4(c).
